
Case Prep: Anterior Thoracic Corpectomy and Reconstruction (Transthoracic / Thoracoscopic)
Case / Approach Snapshot
- Anatomy at risk: level localization, cord/cauda equina, exiting and traversing roots, dura, vertebral artery or segmental vessels, esophagus/trachea/pleura/viscera by approach, and fusion/instrumentation landmarks.
- Operative steps: position and pad carefully, confirm level, expose the planned corridor, decompress neural elements, reconstruct or instrument when indicated, verify alignment/hardware, and close with attention to hematoma and wound risk; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: wrong level, durotomy, neurologic change, vertebral artery/visceral/pleural injury, graft or hardware problem, epidural hematoma, dysphagia/airway issue, and infection prevention/escalation.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [T_] [burst fracture / tumor / infection / calcified central disc with myelopathy] requiring anterior column reconstruction planned for [transthoracic open / thoracoscopic / lateral] thoracic corpectomy and reconstruction.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Transthoracic approach — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Transpedicular partial corpectomy without anterior vertebral reconstruction in thoracic spinal metastases — Chen YJ. Spine 2007. PubMed
- Long-term outcomes of the nano-hydroxyapatite/polyamide-66 cage versus the titanium mesh cage for anterior reconstruction of thoracic and lumbar corpectomy: a retrospective study with at least 7 years of follow-up — Hu B. Journal of orthopaedic surgery and research 2023. PubMed
- Palliative transpedicular partial corpectomy without anterior vertebral reconstruction in lower thoracic and thoracolumbar junction spinal metastases — Chang CC. Journal of orthopaedic surgery and research 2015. PubMed
- Thoracic lateral extracavitary corpectomy for anterior column reconstruction with expandable and static titanium cages: clinical outcomes and surgical considerations in a consecutive case series — Holland CM. Clinical neurology and neurosurgery 2015. PubMed
- Anterior reconstruction with nano-hydroxyapatite/polyamide-66 cage after thoracic and lumbar corpectomy — Yang X. Orthopedics 2012. PubMed
- Low Anterior Cervical Approach Without Sternotomy or Clavicle Resection for Upper Thoracic Vertebra Corpectomy — Babici D. Cureus 2021. PubMed
- Anterior thoracic spine reconstruction using a titanium mesh cage and pedicled rib flap — O’Shaughnessy BA. Spine 2006. PubMed
- Coaxial double-lumen methylmethacrylate reconstruction in the anterior cervical and upper thoracic spine after tumor resection — Miller DJ. Journal of neurosurgery 2000. PubMed
- Vascularized Bone Flap Options for Complex Thoracic Spinal Reconstruction — Asaad M. Plastic and reconstructive surgery 2022. PubMed
- Posterior thoracic corpectomy with cage reconstruction for metastatic spinal tumors: comparing the mini-open approach to the open approach — Lau D. Journal of neurosurgery. Spine 2015. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
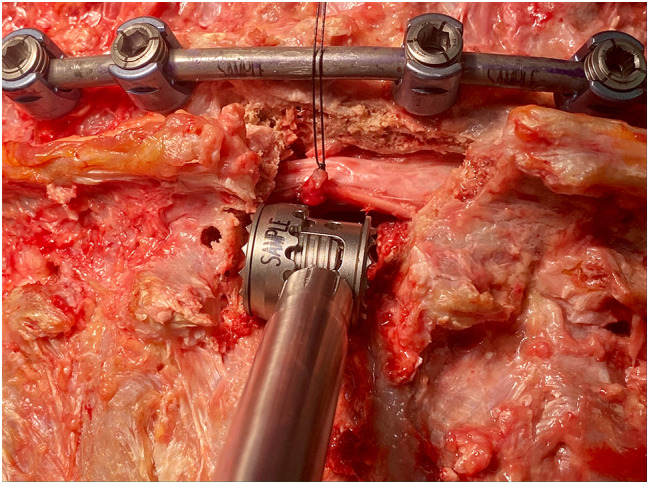 Fig. 2. A titanium expandable corpectomy cage fits into the bespoke bony window using only the tagged nerve for gentle gravity retraction as demonstrated in this cadaveric specimen Source: A rib-sparing unilateral transpedicular thoracic corpectomy using the ultrasonic bone scalpel: a novel technique and pictorial guide — BMC Surgery 2024; CC BY-NC-ND.
Fig. 2. A titanium expandable corpectomy cage fits into the bespoke bony window using only the tagged nerve for gentle gravity retraction as demonstrated in this cadaveric specimen Source: A rib-sparing unilateral transpedicular thoracic corpectomy using the ultrasonic bone scalpel: a novel technique and pictorial guide — BMC Surgery 2024; CC BY-NC-ND.
 Fig. 1. (Left) Swimmer’s view radiograph demonstrating kyphosis related to C4–T2 osteomyelitis. (Right) Sagittal reformatted CT scan demonstrating extensive osseous erosion with kyphotic… Source: Successful outcome of six-level cervicothoracic corpectomy and circumferential reconstruction: case report and review of literature on multilevel cervicothoracic corpectomy — European Spine Journal 2006; open access.
Fig. 1. (Left) Swimmer’s view radiograph demonstrating kyphosis related to C4–T2 osteomyelitis. (Right) Sagittal reformatted CT scan demonstrating extensive osseous erosion with kyphotic… Source: Successful outcome of six-level cervicothoracic corpectomy and circumferential reconstruction: case report and review of literature on multilevel cervicothoracic corpectomy — European Spine Journal 2006; open access.
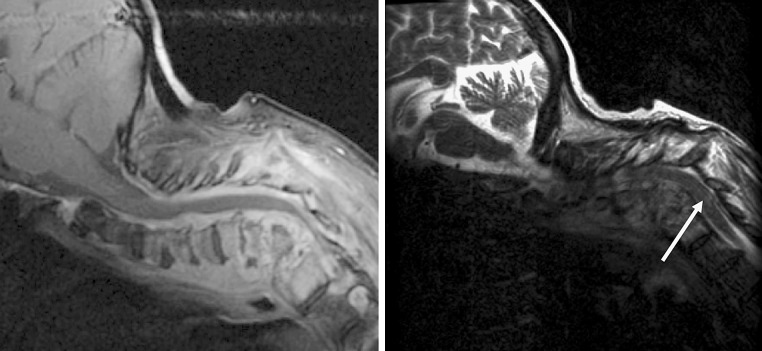 Fig. 2. (Left) Sagittal T1 post-gadolinium MR sequence revealing extensive prevertebral and circumferential enhancing epidural abscess and enhancing vertebrae, compatible with osteomyelitis…. Source: Successful outcome of six-level cervicothoracic corpectomy and circumferential reconstruction: case report and review of literature on multilevel cervicothoracic corpectomy — European Spine Journal 2006; open access.
Fig. 2. (Left) Sagittal T1 post-gadolinium MR sequence revealing extensive prevertebral and circumferential enhancing epidural abscess and enhancing vertebrae, compatible with osteomyelitis…. Source: Successful outcome of six-level cervicothoracic corpectomy and circumferential reconstruction: case report and review of literature on multilevel cervicothoracic corpectomy — European Spine Journal 2006; open access.
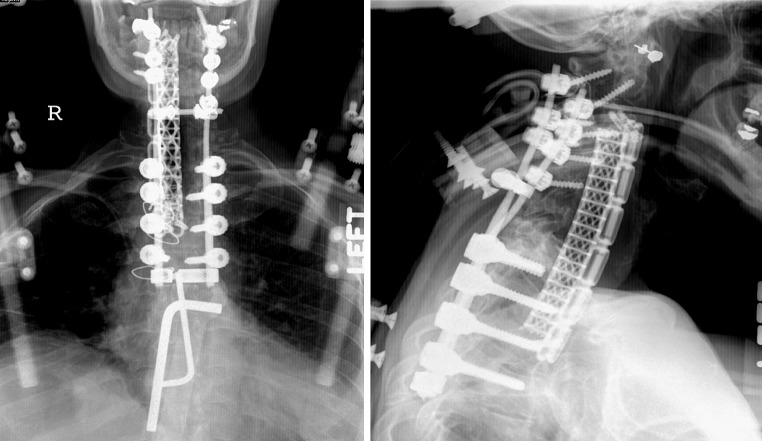 Fig. 3. Postoperative AP and lateral radiographs after six-level corpectomy from C4–T2, anterior interbody contoured cage and anterior plating from C3–T3. Posterior screw-rod fusion is evident… Source: Successful outcome of six-level cervicothoracic corpectomy and circumferential reconstruction: case report and review of literature on multilevel cervicothoracic corpectomy — European Spine Journal 2006; open access.
Fig. 3. Postoperative AP and lateral radiographs after six-level corpectomy from C4–T2, anterior interbody contoured cage and anterior plating from C3–T3. Posterior screw-rod fusion is evident… Source: Successful outcome of six-level cervicothoracic corpectomy and circumferential reconstruction: case report and review of literature on multilevel cervicothoracic corpectomy — European Spine Journal 2006; open access.
 Fig. 4. Flexion (left) and extension (right) plain radiographs obtained at 4-month follow-up demonstrate good hardware positioning without graft dislodgment. Note that the significant correction… Source: Successful outcome of six-level cervicothoracic corpectomy and circumferential reconstruction: case report and review of literature on multilevel cervicothoracic corpectomy — European Spine Journal 2006; open access.
Fig. 4. Flexion (left) and extension (right) plain radiographs obtained at 4-month follow-up demonstrate good hardware positioning without graft dislodgment. Note that the significant correction… Source: Successful outcome of six-level cervicothoracic corpectomy and circumferential reconstruction: case report and review of literature on multilevel cervicothoracic corpectomy — European Spine Journal 2006; open access.
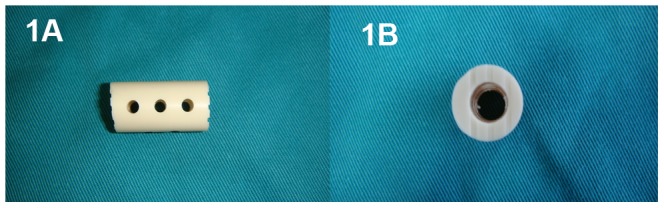 Figure 1. Photographs of lateral (1A) and superior (1B) views of the nano-hydroxyapatite/polyamide66 cage. Source: Evaluation of Anterior Cervical Reconstruction with Titanium Mesh Cages versus Nano-Hydroxyapatite/Polyamide66 Cages after 1- or 2-Level Corpectomy for Multilevel Cervical Spondylotic Myelopathy: A Retrospective Study of 117 Patients — PLoS ONE 2014; CC BY.
Figure 1. Photographs of lateral (1A) and superior (1B) views of the nano-hydroxyapatite/polyamide66 cage. Source: Evaluation of Anterior Cervical Reconstruction with Titanium Mesh Cages versus Nano-Hydroxyapatite/Polyamide66 Cages after 1- or 2-Level Corpectomy for Multilevel Cervical Spondylotic Myelopathy: A Retrospective Study of 117 Patients — PLoS ONE 2014; CC BY.
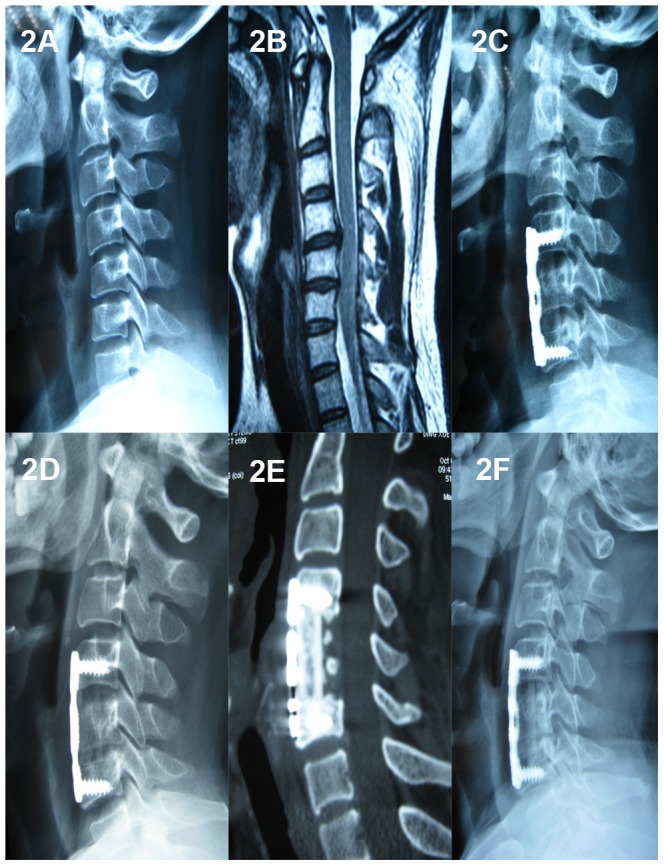 Figure 2. A 36-year-old male who underwent 1-level corpectomy with a nano-hydroxyapatite/polyamide66 cage used for cervical reconstruction.The preoperative cervical X-ray film (2A) and MRI scan… Source: Evaluation of Anterior Cervical Reconstruction with Titanium Mesh Cages versus Nano-Hydroxyapatite/Polyamide66 Cages after 1- or 2-Level Corpectomy for Multilevel Cervical Spondylotic Myelopathy: A Retrospective Study of 117 Patients — PLoS ONE 2014; CC BY.
Figure 2. A 36-year-old male who underwent 1-level corpectomy with a nano-hydroxyapatite/polyamide66 cage used for cervical reconstruction.The preoperative cervical X-ray film (2A) and MRI scan… Source: Evaluation of Anterior Cervical Reconstruction with Titanium Mesh Cages versus Nano-Hydroxyapatite/Polyamide66 Cages after 1- or 2-Level Corpectomy for Multilevel Cervical Spondylotic Myelopathy: A Retrospective Study of 117 Patients — PLoS ONE 2014; CC BY.
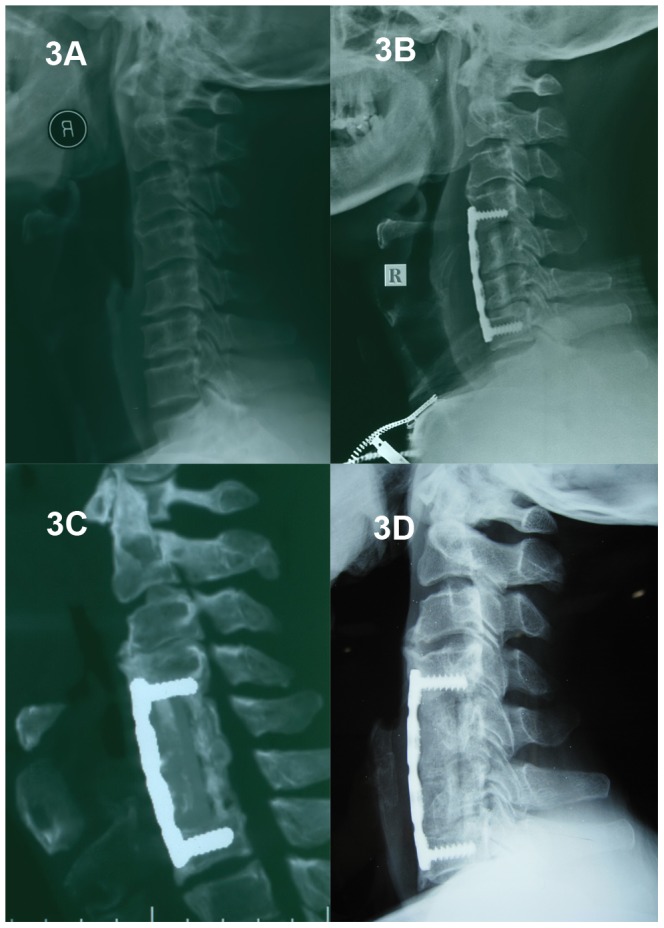 Figure 3. A 61-year-old male who underwent 2-level corpectomy with a nano-hydroxyapatite/polyamide66 cage used for cervical reconstruction.A preoperative cervical X-ray film (3A) shows a loss of… Source: Evaluation of Anterior Cervical Reconstruction with Titanium Mesh Cages versus Nano-Hydroxyapatite/Polyamide66 Cages after 1- or 2-Level Corpectomy for Multilevel Cervical Spondylotic Myelopathy: A Retrospective Study of 117 Patients — PLoS ONE 2014; CC BY.
Figure 3. A 61-year-old male who underwent 2-level corpectomy with a nano-hydroxyapatite/polyamide66 cage used for cervical reconstruction.A preoperative cervical X-ray film (3A) shows a loss of… Source: Evaluation of Anterior Cervical Reconstruction with Titanium Mesh Cages versus Nano-Hydroxyapatite/Polyamide66 Cages after 1- or 2-Level Corpectomy for Multilevel Cervical Spondylotic Myelopathy: A Retrospective Study of 117 Patients — PLoS ONE 2014; CC BY.
History of Present Illness
- Chief complaint: Myelopathy from anterior cord compression, deformity, mechanical pain
- Indication for anterior corpectomy: significant ventral cord compression (retropulsed fragment, tumor, calcified disc, infection/abscess), anterior column deficiency needing reconstruction
- Etiology (trauma/tumor/infection) drives workup
Past Medical History
- Pulmonary function (thoracotomy/lung deflation), cardiac, prior thoracic surgery
- Etiology-specific (oncologic staging, infection source)
- Standard PMH
Imaging Review
MRI / CT Thoracic
- Ventral compression, vertebral body destruction, canal compromise, cord signal
- Level, adjacent levels, segmental vessels / artery of Adamkiewicz (CTA — thoracolumbar, usually left → influences approach side)
- Pleural/mediastinal anatomy, lung
Etiology workup
- Tumor (staging, embolization if vascular), infection (cultures, ESR/CRP), trauma (TLICS, alignment)
Labs
- CBC, BMP, Coags, type and crossmatch (2-4 units), etiology-specific (cultures, markers)
Neurological Examination
- Lower extremity motor/sensory (sensory level), reflexes, gait, sphincter, document baseline
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- OR setup: radiolucent/Jackson table, fluoroscopy or O-arm/navigation, microscope/loupes for decompression, implant trays/graft ready for fusion, neuromonitoring for myelopathy/cord-risk cases, and postop brace plan confirmed.
- Special needs: arterial line/Foley/type-screen for long fusion/corpectomy, no long paralytic when MEPs are used, MAP/normotension for myelopathy or cord-risk cases, antibiotic redosing, and anticoagulation/DVT plan.
- Immediate postop orders: neuro checks by myotome/sensory level, airway/dysphagia watch for anterior cervical cases, CT/X-rays per construct, drain care, brace/activity orders, DVT prophylaxis timing, bowel regimen, and PT/OT mobilization.
Approach & Side
- Open transthoracic (thoracotomy) vs thoracoscopic (VATS) vs mini-open lateral
- Side: generally left for mid-thoracic (avoid liver/IVC; aorta more forgiving/repairable), but right for upper thoracic (avoid heart/aortic arch) and per Adamkiewicz/lesion side
- Access/thoracic surgeon often assists
Position
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- Lateral decubitus, double-lumen ETT with lung deflation on the operative side, axillary roll, table flexed; fluoroscopy/IONM baseline
Key Surgical Steps
- Thoracotomy (rib resection over the level, often the rib 1-2 above) or thoracoscopic portals; deflate lung
- Reflect pleura, ligate segmental vessels at the involved level(s) (preserve Adamkiewicz per CTA), expose the vertebral body
- Confirm level (fluoroscopy)
- Discectomies above and below, then corpectomy (remove vertebral body, decompress the canal ventrally) — work toward but protect the PLL/dura/cord
- Complete ventral cord decompression (remove retropulsed fragment/tumor/abscess)
- Anterior reconstruction: expandable cage / mesh + graft (or PMMA) in the corpectomy defect
- Anterior instrumentation (lateral plate/rod-screw) for stability; ± posterior fixation (staged) for unstable/3-column injuries
- Hemostasis, chest tube, lung re-inflation, closure
Critical Anatomy & Structures at Risk
- Aorta, azygos, segmental vessels, great vessels — major hemorrhage
- Artery of Adamkiewicz / cord blood supply — cord infarction (CTA planning, ligate selectively)
- Spinal cord (ventral decompression), dura
- Lung/pleura (pneumothorax, effusion), thoracic duct (chylothorax — left upper), sympathetic chain/esophagus
Equipment
- Thoracotomy / thoracoscopic (VATS) set, double-lumen tube, chest tube
- High-speed drill, corpectomy instruments, expandable cage/mesh + anterior plate/rod, graft
- Fluoroscopy/navigation, cell saver, crossmatched blood, vascular repair backup
Monitoring
- SSEPs, MEPs, EMG
Anesthesia
- Lung isolation (double-lumen), arterial line, central access, crossmatched blood, MAP support (cord), no paralytic (IONM), thoracic/access surgeon
Potential Complications
- Vascular injury / major hemorrhage, cord infarction (segmental artery), cord injury
- Pulmonary (pneumothorax, effusion, atelectasis, prolonged air leak), chylothorax (thoracic duct)
- Hardware failure/subsidence, CSF leak, approach morbidity (intercostal neuralgia)
Operative Note Template
Preoperative Diagnosis: [T_] [burst fracture / tumor / infection / calcified disc] with ventral cord compression / anterior column deficiency
Postoperative Diagnosis: Same
Procedure: [Transthoracic (open) / thoracoscopic] [T_] corpectomy with anterior reconstruction (expandable cage) and instrumentation [± posterior fixation]
Surgeon / Assistant: Spine + [thoracic/access] surgeon Anesthesia: General endotracheal with double-lumen tube (lung isolation) EBL / Fluids / Blood products: [crossmatched; cell saver] Adjuncts: Fluoroscopy/navigation, high-speed drill; SSEP/MEP; MAP support; chest tube Implants: Expandable cage/mesh + anterior plate/rod-screw, graft Complications: None
Indications: [Age]yo [M/F] with [pathology] at [T_] causing ventral cord compression requiring direct decompression and anterior reconstruction. Approach side [left for mid-thoracic / right for upper-thoracic] per anatomy/Adamkiewicz. Risks (vascular/cord/pulmonary) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced with a double-lumen tube and neuromonitoring established. The patient was positioned in lateral decubitus and the operative-side lung deflated. [A thoracotomy over the appropriate rib / thoracoscopic portals] provided access; the pleura was reflected and the level confirmed. Segmental vessels at the involved level were ligated (preserving the artery of Adamkiewicz per CTA).
Discectomies above and below were followed by a corpectomy with ventral decompression of the canal. An expandable cage [/PMMA-mesh] reconstructed the anterior column, secured with anterior instrumentation [± staged posterior fixation], and alignment confirmed. Hemostasis was obtained. A chest tube was placed and the lung re-inflated.
Closure was performed in layers. The patient was transferred to the ICU with chest-tube/pulmonary care, MAP support, and serial neuro exams.
Postoperative Plan
- ICU, neuro checks (lower extremity/sensory level/sphincter), MAP support
- Chest tube management, CXR (pneumothorax, effusion, chyle — monitor output character)
- CT/X-ray postop (hardware, decompression), pulmonary toilet/incentive spirometry
- DVT prophylaxis, pain control (intercostal/epidural analgesia)
- Etiology-specific (oncology adjuvant/RT, IV antibiotics for infection), follow-up for fusion
Chief-Level Case Review
Use these as the senior-level mental model for Anterior Thoracic Corpectomy and Reconstruction (Transthoracic / Thoracoscopic):
- Decision point: Localize twice and instrument once: numbering, transitional anatomy, prior hardware, rib count, navigation dataset, and fluoroscopic level confirmation are mandatory.
- Technical lever: Positioning is treatment: table choice, abdomen-free prone setup, alignment goals, shoulders/hips, eyes/plexus pressure, neuromonitoring baselines, and fluoroscopic access all change the case.
- Bailout: Protect neural elements by sequence: decompression before correction when needed, MAP support for cord risk, no long paralytic with MEPs, and immediate response to signal change.
- Postop watch: Finish with construct logic: decompression adequacy, screw purchase, alignment, fusion bed/graft, drain plan, brace/activity orders, postop CT/X-rays, and DVT timing.
Common Pimp Questions
Use these to pressure-test preparation for Anterior Thoracic Corpectomy and Reconstruction (Transthoracic / Thoracoscopic):
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]