
Case Prep: Laser Interstitial Thermal Therapy (LITT)
Case / Approach Snapshot
- Anatomy at risk: target volume, organs at risk, cranial nerves, optic apparatus/brainstem/cord tolerance, vascular structures, and prior-treatment fields.
- Operative steps: define indication, fuse imaging, contour target and organs at risk, choose dose/fractionation, check constraints and conformity, deliver treatment, and plan imaging follow-up; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: edema, radionecrosis, cranial neuropathy, optic/brainstem tolerance issue, hemorrhage, progression versus treatment effect, steroids/bevacizumab, surgery, or repeat radiation strategy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [deep/eloquent glioma or metastasis / radiation necrosis / mesial temporal epilepsy / hypothalamic hamartoma] planned for MRI-guided stereotactic laser interstitial thermal therapy (LITT).
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — figures © linked; see media-sources.md
High-Yield Literature
- Laser interstitial thermal therapy — Holste KG. Neuro-oncology advances 2020. PubMed
- Laser Interstitial Thermal Therapy for Epilepsy — Van Gompel JJ. Neurosurgery clinics of North America 2023. PubMed
- Laser interstitial thermal therapy in gliomas — Bozinov O. Cancer letters 2020. PubMed
- Laser Interstitial Thermal Therapy for Radionecrosis — Terrapon APR. Neurosurgery clinics of North America 2023. PubMed
- Laser Interstitial Thermal Therapy for Cavernous Malformations: A Systematic Review — Yousefi O. Frontiers in surgery 2022. PubMed
- Laser interstitial thermal therapy in neuro-oncology applications — Hong CS. Surgical neurology international 2020. PubMed
- Laser Interstitial Thermal Therapy — Patel B. Missouri medicine 2020. PubMed
- Laser interstitial thermal therapy in drug-resistant epilepsy — Shimamoto S. Current opinion in neurology 2019. PubMed
- Laser interstitial thermal therapy for treatment of cerebral radiation necrosis — Hong CS. International journal of hyperthermia : the official journal of European Society for Hyperthermic Oncology, North American Hyperthermia Group 2020. PubMed
- Posterior Fossa Laser Interstitial Thermal Therapy in Children — Mirone G. Neurosurgery clinics of North America 2023. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
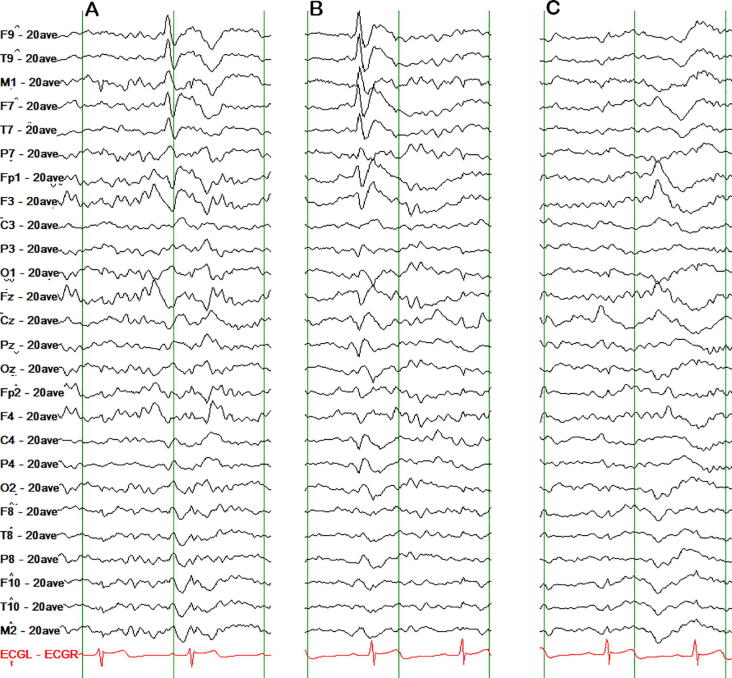 Fig. 1. Heterogeneous interictal epileptiform discharges. A: Left temporal sharp wave. B: Left frontotemporal sharp wave. C: Left orbitofrontal sharp wave. High pass filter: 1 Hz. Low pass… Source: Laser interstitial thermal therapy for NPRL3-related epilepsy with multiple seizure foci: A case report — Epilepsy & Behavior Reports 2021; CC BY-NC-ND.
Fig. 1. Heterogeneous interictal epileptiform discharges. A: Left temporal sharp wave. B: Left frontotemporal sharp wave. C: Left orbitofrontal sharp wave. High pass filter: 1 Hz. Low pass… Source: Laser interstitial thermal therapy for NPRL3-related epilepsy with multiple seizure foci: A case report — Epilepsy & Behavior Reports 2021; CC BY-NC-ND.
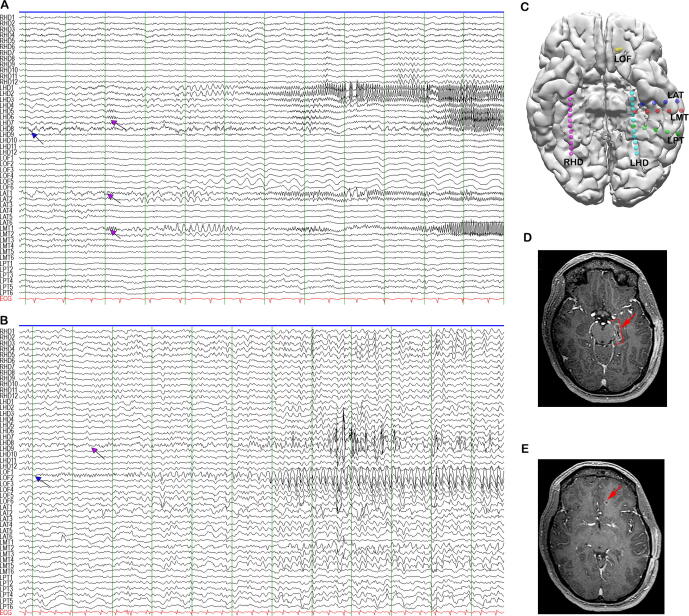 Fig. 2. Illustrations of two independent ictal onsets, depth electrode localization and post-ablation lesions. A: left hippocampal ictal onset (LHD7, 8) with propagation to the left anterior… Source: Laser interstitial thermal therapy for NPRL3-related epilepsy with multiple seizure foci: A case report — Epilepsy & Behavior Reports 2021; CC BY-NC-ND.
Fig. 2. Illustrations of two independent ictal onsets, depth electrode localization and post-ablation lesions. A: left hippocampal ictal onset (LHD7, 8) with propagation to the left anterior… Source: Laser interstitial thermal therapy for NPRL3-related epilepsy with multiple seizure foci: A case report — Epilepsy & Behavior Reports 2021; CC BY-NC-ND.
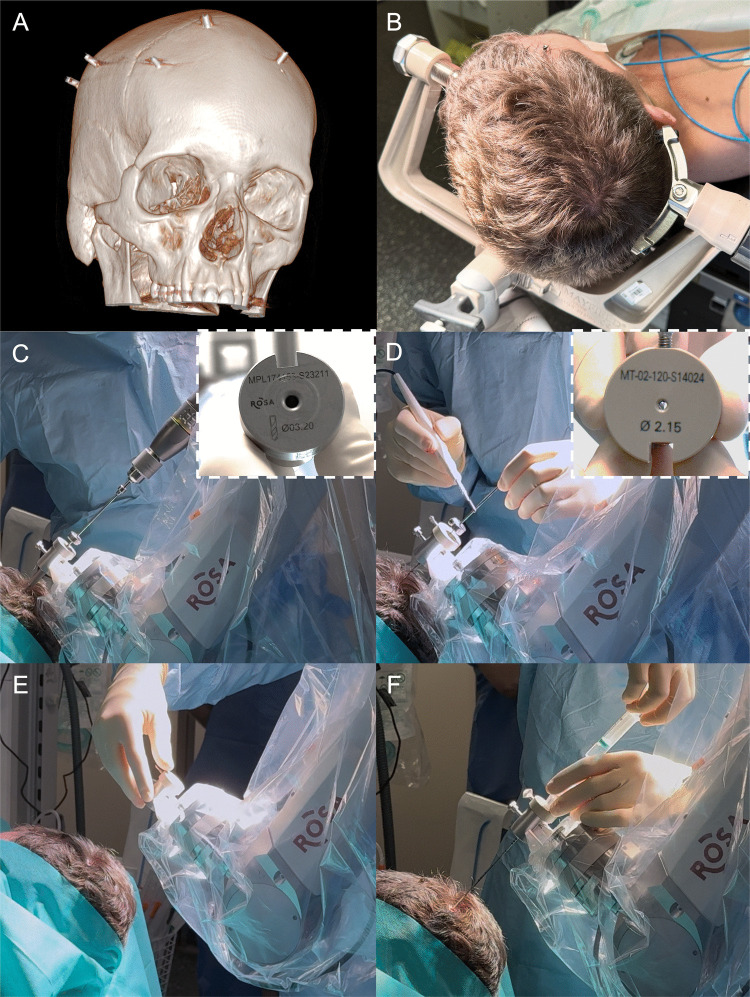 Fig. 1. Step 1: Robot-assisted stereotactic biopsy. A CT scan exhibiting five skull-implanted fiducials used for registration, B Skull immobilization and connection to the ROSA system using a… Source: How I do it: sequential robot-assisted stereotactic biopsy and laser interstitial thermal therapy for epilepsy associated with brain tumors — Acta Neurochirurgica 2025; CC BY-NC-ND.
Fig. 1. Step 1: Robot-assisted stereotactic biopsy. A CT scan exhibiting five skull-implanted fiducials used for registration, B Skull immobilization and connection to the ROSA system using a… Source: How I do it: sequential robot-assisted stereotactic biopsy and laser interstitial thermal therapy for epilepsy associated with brain tumors — Acta Neurochirurgica 2025; CC BY-NC-ND.
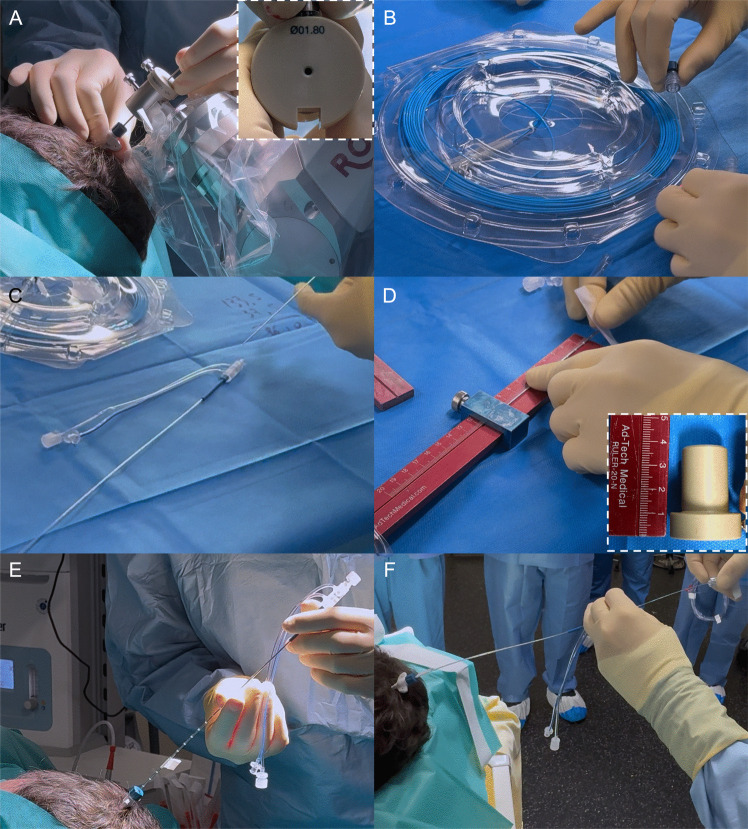 Fig. 2. Step 2: Robot-assisted laser interstitial thermal therapy. A Placement of the guidance bold using a 1.8 mm wide reducer, B Transitory insertion of the flexible optic fiber in the cooling… Source: How I do it: sequential robot-assisted stereotactic biopsy and laser interstitial thermal therapy for epilepsy associated with brain tumors — Acta Neurochirurgica 2025; CC BY-NC-ND.
Fig. 2. Step 2: Robot-assisted laser interstitial thermal therapy. A Placement of the guidance bold using a 1.8 mm wide reducer, B Transitory insertion of the flexible optic fiber in the cooling… Source: How I do it: sequential robot-assisted stereotactic biopsy and laser interstitial thermal therapy for epilepsy associated with brain tumors — Acta Neurochirurgica 2025; CC BY-NC-ND.
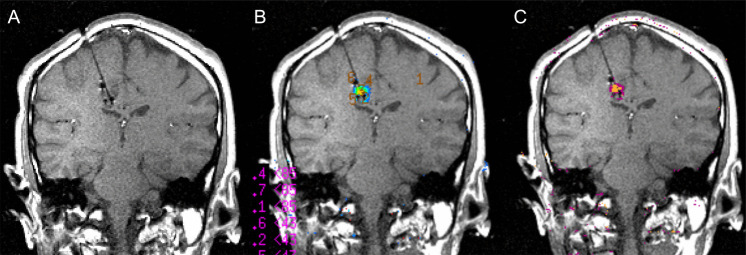 Fig. 3. Intraoperative installation and brain magnetic resonance imaging (MRI) of laser interstitial thermal therapy. A T1-weighted coronal view showing the position of the optical fiber and the… Source: How I do it: sequential robot-assisted stereotactic biopsy and laser interstitial thermal therapy for epilepsy associated with brain tumors — Acta Neurochirurgica 2025; CC BY-NC-ND.
Fig. 3. Intraoperative installation and brain magnetic resonance imaging (MRI) of laser interstitial thermal therapy. A T1-weighted coronal view showing the position of the optical fiber and the… Source: How I do it: sequential robot-assisted stereotactic biopsy and laser interstitial thermal therapy for epilepsy associated with brain tumors — Acta Neurochirurgica 2025; CC BY-NC-ND.
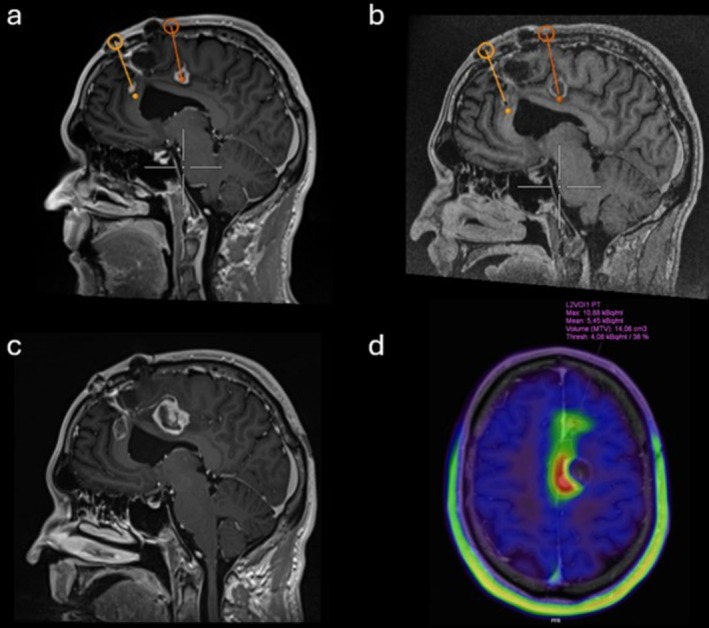 FIGURE 1. Pre‐ and post‐LITT neuroimaging. Pre‐operative (A) and post‐operative (B) T1‐weighted MRI obtained with half‐dose gadolinium show the trajectories of the laser fibres positioned anterior… Source: MR‐Guided Laser Interstitial Thermal Therapy for Recurrent Glioblastoma: A Case Report With Novel Insights Into Histopathological Changes and Immunological Responses — Neuropathology and Applied Neurobiology 2026; CC BY-NC.
FIGURE 1. Pre‐ and post‐LITT neuroimaging. Pre‐operative (A) and post‐operative (B) T1‐weighted MRI obtained with half‐dose gadolinium show the trajectories of the laser fibres positioned anterior… Source: MR‐Guided Laser Interstitial Thermal Therapy for Recurrent Glioblastoma: A Case Report With Novel Insights Into Histopathological Changes and Immunological Responses — Neuropathology and Applied Neurobiology 2026; CC BY-NC.
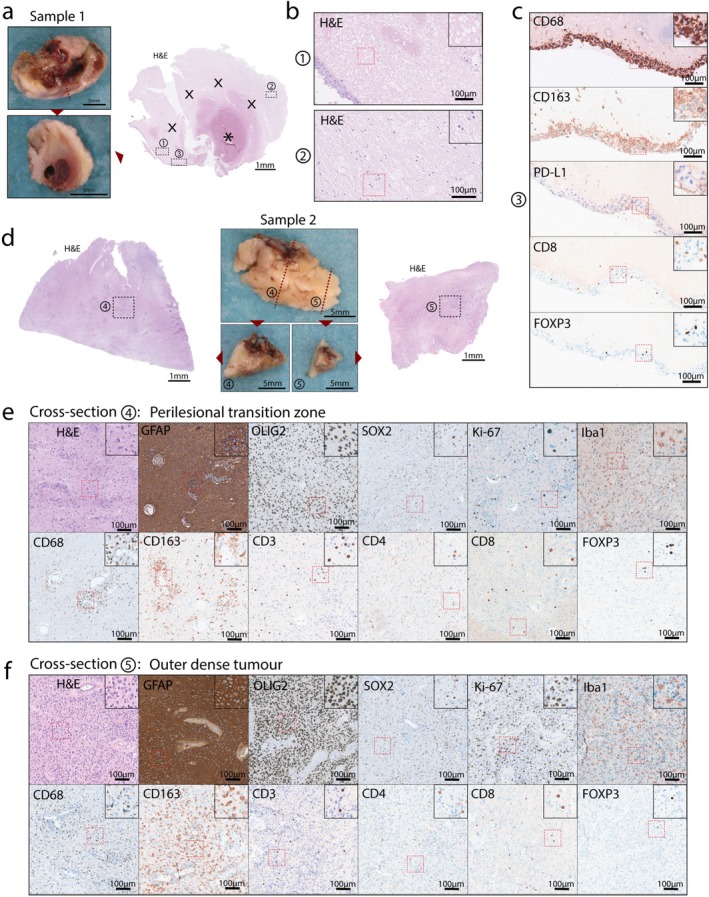 FIGURE 2. Histological analysis of the two lesions following thermal laser ablation. (A) Macroscopic photographs of the first sample taken before and after sectioning, along with an H&E overview… Source: MR‐Guided Laser Interstitial Thermal Therapy for Recurrent Glioblastoma: A Case Report With Novel Insights Into Histopathological Changes and Immunological Responses — Neuropathology and Applied Neurobiology 2026; CC BY-NC.
FIGURE 2. Histological analysis of the two lesions following thermal laser ablation. (A) Macroscopic photographs of the first sample taken before and after sectioning, along with an H&E overview… Source: MR‐Guided Laser Interstitial Thermal Therapy for Recurrent Glioblastoma: A Case Report With Novel Insights Into Histopathological Changes and Immunological Responses — Neuropathology and Applied Neurobiology 2026; CC BY-NC.
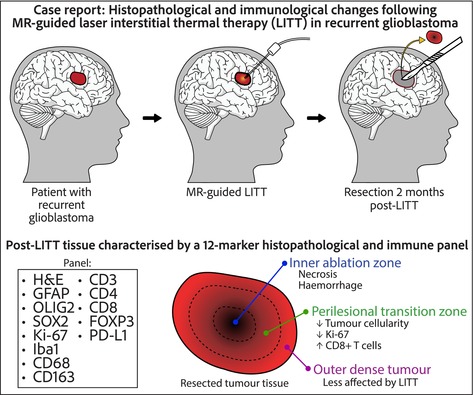 Figure 8. Source: MR‐Guided Laser Interstitial Thermal Therapy for Recurrent Glioblastoma: A Case Report With Novel Insights Into Histopathological Changes and Immunological Responses — Neuropathol Appl Neurobiol. 2026 Mar 30;52(2):e70071. doi: 10.1111/nan.70071; CC BY-NC.
Figure 8. Source: MR‐Guided Laser Interstitial Thermal Therapy for Recurrent Glioblastoma: A Case Report With Novel Insights Into Histopathological Changes and Immunological Responses — Neuropathol Appl Neurobiol. 2026 Mar 30;52(2):e70071. doi: 10.1111/nan.70071; CC BY-NC.
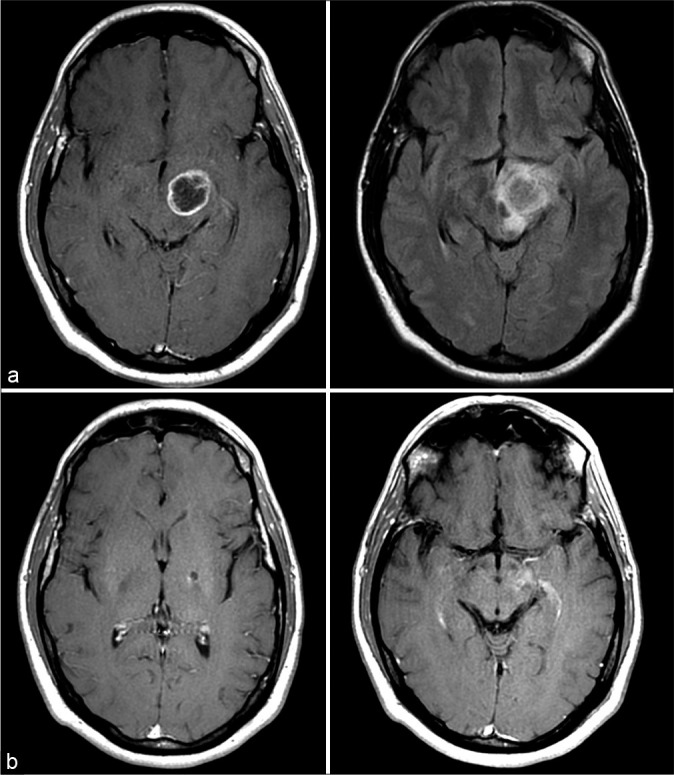 Figure 1:. Pre and postoperative MRI. (a) Representative preoperative T1 contrast enhanced (left) and FLAIR (right) images. (b) Representative 46.9-month post-LITT T1 contrast enhanced (left) and… Source: Prolonged survival after laser interstitial thermal therapy in glioblastoma — Surgical Neurology International 2021; CC BY-NC-SA.
Figure 1:. Pre and postoperative MRI. (a) Representative preoperative T1 contrast enhanced (left) and FLAIR (right) images. (b) Representative 46.9-month post-LITT T1 contrast enhanced (left) and… Source: Prolonged survival after laser interstitial thermal therapy in glioblastoma — Surgical Neurology International 2021; CC BY-NC-SA.
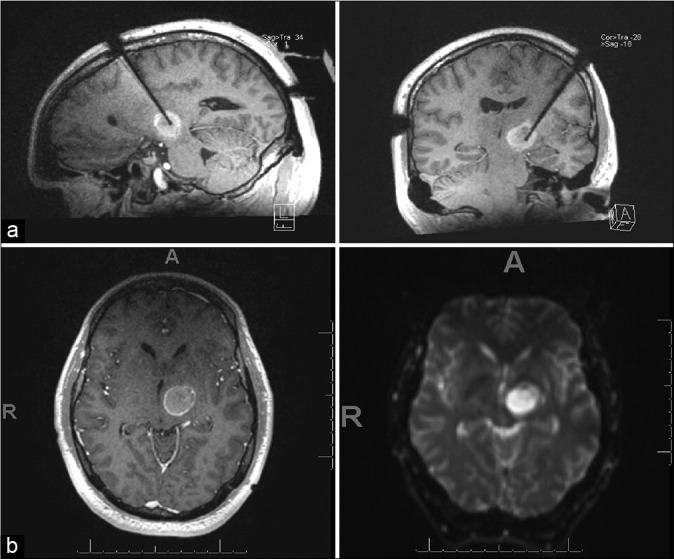 Figure 2:. Intraoperative and immediate postoperative MRI. (a) Intraoperative MRI demonstrating laser probe position. (b) Immediate postoperative T1-weighterd post-contrast and diffusion-weighted… Source: Prolonged survival after laser interstitial thermal therapy in glioblastoma — Surgical Neurology International 2021; CC BY-NC-SA.
Figure 2:. Intraoperative and immediate postoperative MRI. (a) Intraoperative MRI demonstrating laser probe position. (b) Immediate postoperative T1-weighterd post-contrast and diffusion-weighted… Source: Prolonged survival after laser interstitial thermal therapy in glioblastoma — Surgical Neurology International 2021; CC BY-NC-SA.
History of Present Illness
- Chief complaint / indication:
- Deep/eloquent or surgically inaccessible tumor (glioma, metastasis) — minimally invasive cytoreduction
- Radiation necrosis (post-SRS) refractory to steroids
- Mesial temporal lobe epilepsy (laser amygdalohippocampotomy — alternative to open ATL)
- Hypothalamic hamartoma (gelastic seizures), other epileptic foci (focal cortical dysplasia, periventricular nodular heterotopia)
- Prior treatments (surgery, SRS, chemo/RT), epilepsy workup (if epilepsy indication)
Past Medical History
- Coagulopathy/anticoagulation (correct — catheter hemorrhage), MRI compatibility, prior radiation/surgery
- Standard PMH; epilepsy workup if applicable (video-EEG, MRI, ± SEEG)
Imaging Review
MRI (target delineation) + planning
- Target (tumor/necrosis/epileptogenic focus) size and shape (LITT best for smaller, roughly ellipsoid lesions, ~≤3 cm), proximity to critical structures
- Trajectory planning — avascular path avoiding sulci/vessels/ventricles to the target long axis
- Proximity to heat-sensitive structures (large vessels = heat-sink; near optic apparatus/brainstem — caution)
Intraoperative MRI thermometry
- Real-time temperature mapping during ablation (the defining feature of LITT)
Labs
- CBC, Coags, BMP, type and screen
Neurological Examination
- Baseline focal exam (deficits near target), document; epilepsy baseline if applicable
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: stereotaxy/robot or frame, MRI-compatible laser system, thermal-damage monitoring workflow, biopsy supplies if planned, and MRI/anesthesia coordination before incision.
- Special needs: steroid plan for edema, antiepileptic plan for cortical/epilepsy lesions, temperature/thermal safety checks, and readiness for aborting if trajectory or heating is unsafe.
- Immediate postop orders: neuro checks, MRI/CT review for hemorrhage/edema, dexamethasone taper, seizure precautions when relevant, pain/nausea control, and follow-up MRI schedule for ablation evolution.
Workflow / Platform
- Stereotactic placement of a cooled laser fiber catheter along the planned trajectory, then MRI-guided thermal ablation with real-time MR thermometry
- Platforms: Visualase (Medtronic), NeuroBlate (Monteris)
- Stereotaxy: frame-based, frameless, or robotic (ROSA/Mazor); bone anchor; often done in or transferred to an MRI suite (iMRI or diagnostic MRI)
Position
- Per trajectory; head fixed (frame/robot reference); MRI-compatible setup
Key Surgical Steps
- Plan trajectory (target long axis, avascular path), register stereotactic system
- Small stab incision, twist-drill at entry, place a bone anchor along the trajectory
- Insert the laser fiber catheter to the planned depth at the target
- Confirm catheter position on MRI
- MRI-guided ablation: deliver laser energy while monitoring real-time MR thermometry; software predicts the thermal damage estimate; ablate the target while monitoring temperature at the margins to protect adjacent critical structures (automatic shutoff if OAR thresholds approached)
- Reposition/pull-back along the trajectory to ablate the lesion length as needed
- Confirm ablation coverage (thermal damage map / post-ablation MRI), remove catheter
- Single suture closure
Critical Anatomy & Structures at Risk
- Adjacent eloquent brain / tracts / cranial nerves / optic apparatus / brainstem — thermal spread (thermometry protects)
- Vessels along trajectory (hemorrhage) and large vessels near target (heat-sink → incomplete ablation)
- Ependyma/ventricle (trajectory)
Equipment
- LITT system (Visualase/NeuroBlate — laser, cooled catheter, thermometry software)
- Stereotactic platform (frame/frameless/robot), bone anchor, twist drill
- MRI suite (intraoperative or diagnostic) with thermometry, MRI-compatible instruments
Anesthesia
- General (MRI environment), BP control (hemorrhage), MRI-safe setup
Potential Complications
- Hemorrhage (catheter placement), thermal injury to adjacent structures (deficit), edema (post-ablation — often transient, steroids)
- Incomplete ablation (large/irregular lesions, heat-sink near vessels), catheter malposition
- Seizure, infection, transient neurological worsening (peri-ablation edema)
- For epilepsy: visual field deficit (mesial temporal — optic radiation), memory effects
Procedure Note Template
Preoperative Diagnosis: [Deep/eloquent tumor / radiation necrosis / mesial temporal epilepsy / hypothalamic hamartoma]
Postoperative Diagnosis: Same
Procedure: MRI-guided stereotactic laser interstitial thermal therapy (LITT) of [target] via [frame/frameless/robotic] stereotaxy
Surgeon / Assistant: Anesthesia: General endotracheal (MRI environment) EBL / Fluids: Minimal Adjuncts: LITT system [Visualase/NeuroBlate] with cooled laser catheter + real-time MR thermometry, stereotactic platform, bone anchor; intraoperative MRI Complications: None
Indications: [Age]yo [M/F] with a [deep/eloquent/small] [target] amenable to minimally invasive ablation. Risks (hemorrhage, thermal injury to adjacent structures, edema, incomplete ablation) discussed. [Biopsy obtained at the same setting as LITT yields no tissue.]
Description of Procedure: After consent and time-out, general anesthesia was induced and the patient registered to the [frame/robot] with an avascular trajectory planned along the target long axis. A stab incision and twist-drill were made, a bone anchor placed, and the cooled laser catheter inserted to the planned depth, with position confirmed on MRI.
MRI-guided ablation was performed with real-time MR thermometry, delivering laser energy to the target while monitoring margin temperatures to protect adjacent critical structures (automatic shutoff thresholds set); the catheter was repositioned along the trajectory to cover the lesion length. The thermal damage estimate / post-ablation MRI confirmed coverage, and the catheter was removed and the incision closed with a single suture.
The patient was transferred [to the ICU overnight] with a short steroid course for peri-ablation edema; a postoperative MRI was reviewed.
Post-Treatment Plan
- ICU/step-down overnight, neuro checks; short steroid course (peri-ablation edema)
- Postop MRI (ablation coverage, hemorrhage), watch for transient edema-related deficit
- DVT prophylaxis, seizure management (epilepsy/tumor)
- Pathology note: LITT does not provide tissue — biopsy at same setting if diagnosis needed
- Tumor: oncology follow-up, surveillance MRI (ablation cavity evolves); Epilepsy: seizure-outcome tracking, AED management; Radiation necrosis: symptom/steroid follow-up
Chief-Level Case Review
Use these as the senior-level mental model for Laser Interstitial Thermal Therapy (LITT):
- Decision point: The target must answer the question: choose tissue/trajectory/dose based on diagnostic yield, molecular testing, treatment impact, and safest corridor.
- Technical lever: Risk lives along the path: vessels, sulci, ventricles, necrotic center, eloquent tracts, prior radiation, and anticoagulation decide whether the plan is acceptable.
- Bailout: Confirm before committing: frame/robot registration, coordinates, fiducials, trajectory collision, specimen adequacy, and postop scan threshold should be explicit.
- Postop watch: Postop plan should anticipate the rare catastrophe: hemorrhage, edema, seizure, steroid need, neurologic checks, pathology handoff, and treatment-board timing.
Common Pimp Questions
Use these to pressure-test preparation for Laser Interstitial Thermal Therapy (LITT):
- What target coordinate, trajectory, and no-fly-zone were chosen?
- What imaging confirms target accuracy and avoids vessel/ventricle/sulcus violation?
- What specimen, pathology, culture, or molecular study must be obtained?
- What hemorrhage, edema, seizure, or thermal-injury sign must be watched for tonight?
- What postop scan timing and steroid/antiepileptic plan is appropriate?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Frame versus frameless/robot platform and planning software: [attending-specific]
- Trajectory constraints, number of cores/targets, and frozen/permanent pathology plan: [attending-specific]
- Steroid/antiepileptic prophylaxis and postop scan timing: [attending-specific]
- Admit versus discharge threshold and neuro-check frequency: [attending-specific]