
Case Prep: Cubital Tunnel Release / Ulnar Nerve Transposition
Case / Approach Snapshot
- Anatomy at risk: nerve course, fascicles, compression points, motor and sensory branches, adjacent vessels, scar planes, and distal targets for repair or transfer.
- Operative steps: mark landmarks, expose normal nerve proximally/distally, decompress or mobilize gently, resect/repair/graft/transfer as indicated, verify tension-free alignment, and close to protect gliding tissue; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: iatrogenic nerve injury, neuroma or neuropathic pain, vascular injury, incomplete decompression, recurrence, wound problems, and therapy/splinting or revision plan.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [left/right] cubital tunnel syndrome (ulnar neuropathy at the elbow) refractory to conservative management planned for [in situ decompression / anterior (subcutaneous/submuscular) transposition] of the ulnar nerve.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
CNS Video Library
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Cubital Tunnel Syndrome: Current Concepts — Staples JR. The Journal of the American Academy of Orthopaedic Surgeons 2017. PubMed
- Ulnar neuropathy at the elbow — Cambon-Binder A. Orthopaedics & traumatology, surgery & research : OTSR 2021. PubMed
- Modern Treatment of Cubital Tunnel Syndrome: Evidence and Controversy — Graf A. Journal of hand surgery global online 2023. PubMed
- A Comprehensive Review of Cubital Tunnel Syndrome — Anderson D. Orthopedic reviews 2022. PubMed
- Higher Revision Rates With In Situ Decompression as Compared to Ulnar Nerve Transposition for Cubital Tunnel Syndrome: A Meta-Regression Analysis — Reichenbach R. Cureus 2024. PubMed
- Challenging the dogma: anterior transposition of the ulnar nerve is indicated in recurrent cubital tunnel syndrome — Ruettermann M. The Journal of hand surgery, European volume 2021. PubMed
- Novel Technique for Ulnar Nerve Transposition at the Elbow: The Neocubital Tunnel — Bakhach J. Plastic and reconstructive surgery. Global open 2024. PubMed
- Decision-Making Factors for Ulnar Nerve Transposition in Cubital Tunnel Surgery — DeGeorge BR Jr. Journal of wrist surgery 2019. PubMed
- Subcutaneous Versus Submuscular Anterior Transposition of the Ulnar Nerve for Cubital Tunnel Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials and Observational Studies — Liu CH. Medicine 2015. PubMed
- Ulnar Nerve Decompression With Subcutaneous Transposition — Jurgensmeier K. Video journal of sports medicine 2024. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
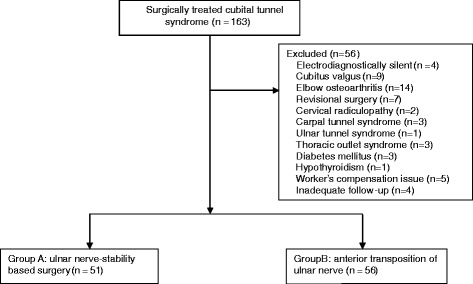 Fig. 1. The CONSORT diagram of enrollment and analysis in this study Source: Ulnar nerve stability-based surgery for cubital tunnel syndrome via a small incision: a comparison with classic anterior nerve transposition — Journal of Orthopaedic Surgery and Research 2015; CC BY.
Fig. 1. The CONSORT diagram of enrollment and analysis in this study Source: Ulnar nerve stability-based surgery for cubital tunnel syndrome via a small incision: a comparison with classic anterior nerve transposition — Journal of Orthopaedic Surgery and Research 2015; CC BY.
 Fig. 2. While introducing and opening a long nasal speculum over the brachial fascia, the proximal nerve compression structures including the arcade of Struthers were completely released Source: Ulnar nerve stability-based surgery for cubital tunnel syndrome via a small incision: a comparison with classic anterior nerve transposition — Journal of Orthopaedic Surgery and Research 2015; CC BY.
Fig. 2. While introducing and opening a long nasal speculum over the brachial fascia, the proximal nerve compression structures including the arcade of Struthers were completely released Source: Ulnar nerve stability-based surgery for cubital tunnel syndrome via a small incision: a comparison with classic anterior nerve transposition — Journal of Orthopaedic Surgery and Research 2015; CC BY.
 Fig. 3. After releasing the proximal nerve compression structures, Osborne’s ligament, Osborne’s fascia, and the deep flexor-pronator aponeurosis were sequentially released Source: Ulnar nerve stability-based surgery for cubital tunnel syndrome via a small incision: a comparison with classic anterior nerve transposition — Journal of Orthopaedic Surgery and Research 2015; CC BY.
Fig. 3. After releasing the proximal nerve compression structures, Osborne’s ligament, Osborne’s fascia, and the deep flexor-pronator aponeurosis were sequentially released Source: Ulnar nerve stability-based surgery for cubital tunnel syndrome via a small incision: a comparison with classic anterior nerve transposition — Journal of Orthopaedic Surgery and Research 2015; CC BY.
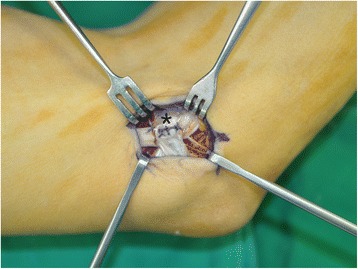 Fig. 4. In patients with an unstable ulnar nerve, the nerve was anteriorly transposed, and a fascial sling () was created Source: Ulnar nerve stability-based surgery for cubital tunnel syndrome via a small incision: a comparison with classic anterior nerve transposition — Journal of Orthopaedic Surgery and Research 2015; CC BY.*
Fig. 4. In patients with an unstable ulnar nerve, the nerve was anteriorly transposed, and a fascial sling () was created Source: Ulnar nerve stability-based surgery for cubital tunnel syndrome via a small incision: a comparison with classic anterior nerve transposition — Journal of Orthopaedic Surgery and Research 2015; CC BY.*
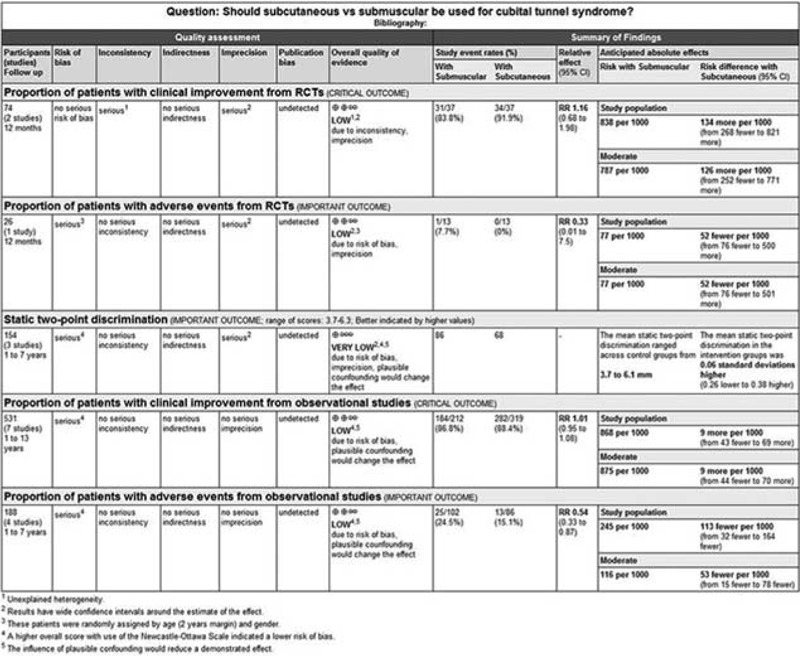 FIGURE 4. The quality of the evidences for each outcome. Source: Subcutaneous Versus Submuscular Anterior Transposition of the Ulnar Nerve for Cubital Tunnel Syndrome — Medicine 2015; CC BY.
FIGURE 4. The quality of the evidences for each outcome. Source: Subcutaneous Versus Submuscular Anterior Transposition of the Ulnar Nerve for Cubital Tunnel Syndrome — Medicine 2015; CC BY.
History of Present Illness
- Chief complaint: Numbness/tingling in ulnar distribution (small + ulnar ring finger), medial elbow pain, hand weakness/clumsiness, worse with elbow flexion (phone, sleeping)
- Intrinsic hand weakness, grip/pinch weakness; advanced: clawing, Wartenberg/Froment signs, intrinsic atrophy
- Failed conservative: night extension splinting, activity modification, padding
- Prior elbow trauma/fracture (tardy ulnar palsy), arthritis
Past Medical History
- Diabetes, prior elbow trauma/fracture/arthritis, prior surgery, occupational/positional factors
- Standard PMH
Imaging / Studies
EMG/NCS
- Ulnar neuropathy at the elbow — conduction slowing/block across the elbow, localizes lesion, severity, excludes C8-T1 radiculopathy/Guyon canal
X-ray / Ultrasound (selective)
- Elbow bony anatomy (cubitus valgus, osteophytes), nerve subluxation, mass
Labs
- Per comorbidity; routine pre-op
Neurological Examination
- Ulnar sensory (small/ulnar ring, dorsal ulnar hand), intrinsics (interossei, FDI, hypothenar, FDP to small/ring), Froment, Wartenberg, clawing, Tinel at elbow, elbow flexion test, nerve subluxation with flexion
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: hand table or radiolucent arm board, tourniquet when used, loupes/microscope available for nerve repair/tumor work, bipolar, microsuture/nerve-wrap options, and nerve stimulator for plexus or motor-branch cases.
- Special needs: regional/local/WALANT versus general anesthesia plan, antibiotic decision for implants/long exposure, anticoagulation plan, and clear laterality/site marking with preop motor/sensory baseline documented.
- Immediate postop orders: elevation, soft dressing or splint duration, early finger/limb ROM unless repair restricts it, oral analgesia, wound check/suture removal timing, therapy referral, and return precautions for hematoma or new motor deficit.
Procedure Selection
- In situ decompression (simple cubital tunnel release): release Osborne ligament/cubital tunnel retinaculum, FCU aponeurosis; for nerve that does NOT subluxate; less dissection, preserves blood supply
- Anterior transposition (subcutaneous or submuscular): for nerve subluxation/dislocation, recurrent cases, significant valgus, bony deformity — moves nerve anterior to flexion axis (relieves traction)
- Medial epicondylectomy: alternative
- Endoscopic in situ release: option
Decision Points Before Incision
- Match the operation to the failure mode: static compression alone often fits in situ release; dynamic subluxation, traction over a valgus elbow, post-traumatic deformity, scarring, or failed release pushes toward transposition.
- Document severity: sensory-only disease, intrinsic weakness, clawing, denervation on EMG, and chronic atrophy have different recovery expectations.
- Examine for double-crush or mimics: cervical radiculopathy, brachial plexopathy, Guyon canal compression, diabetic neuropathy, and medial epicondylitis can all cloud the outcome.
- Plan the postoperative immobilization and therapy around technique; submuscular transposition pays for its deeper bed with more soft-tissue morbidity and stiffness risk.
Position & Anesthesia
- Supine, arm on hand table, shoulder abducted/externally rotated, elbow flexed, tourniquet; regional/general
Key Surgical Steps (Transposition)
- Tourniquet, curvilinear incision posterior/medial elbow between medial epicondyle and olecranon
- Protect medial antebrachial cutaneous nerve (MABC) branches (cross the field — neuroma if injured)
- Identify ulnar nerve proximal to the cubital tunnel
- Decompress: release the cubital tunnel retinaculum (Osborne), arcade of Struthers proximally, and the FCU aponeurosis (two heads) distally — release all compression points
- Mobilize the nerve, preserving its segmental blood supply; ligate/divide tethering articular branches (preserve motor branches to FCU)
- Transpose anterior to the medial epicondyle:
- Subcutaneous: place anterior to epicondyle, secure with fascial sling (prevent subluxation back)
- Submuscular: under the flexor-pronator mass (release and reattach origin)
- Ensure no kinking/new compression along new course; check through full ROM
- Release tourniquet, hemostasis, closure, soft dressing ± splint
Critical Anatomy & Structures at Risk
- Ulnar nerve and its motor branches to FCU (preserve), articular branches (sacrifice)
- Medial antebrachial cutaneous nerve (MABC) — painful neuroma
- New compression/kinking at transposition site, devascularization (preserve vessels)
- Medial epicondyle, flexor-pronator origin (submuscular)
Equipment
- Minor/peripheral nerve set, tourniquet, loupes, bipolar, nerve stimulator
- Endoscopic system (if endoscopic in situ)
Anesthesia
- Regional/general; tourniquet
Potential Complications
- Persistent/recurrent symptoms (incomplete release, perineural scar)
- MABC neuroma, ulnar nerve injury/devascularization
- New compression at transposition, elbow stiffness/flexion contracture, instability of nerve
- Hematoma, infection
Failure and Revision Logic
- Persistent early symptoms: verify complete proximal/distal release, hematoma, excessive tension, and whether preoperative axonal loss makes recovery slow rather than failed.
- New medial forearm pain: suspect MABC branch injury/neuroma or scar tethering; document sensory territory and avoid assuming recurrent cubital tunnel.
- Recurrent compression after in situ release: look for scarring, missed FCU/aponeurotic band, nerve subluxation, or valgus traction; revision often requires transposition with careful vascular preservation.
- Symptoms after transposition: check for kinking at the fascial sling, compression at the new tunnel edges, devascularization, or instability back over the epicondyle through elbow ROM.
- Severe intrinsic atrophy: counsel that decompression protects remaining function and may improve sensation/pain, but motor recovery can take months and may be incomplete.
Operative Note Template
Preoperative Diagnosis: [Left/Right] cubital tunnel syndrome (ulnar neuropathy at the elbow)
Postoperative Diagnosis: Same
Procedure: [Left/Right] [in situ cubital tunnel release / anterior subcutaneous (or submuscular) ulnar nerve transposition]
Surgeon / Assistant: Anesthesia: [Regional / general] Tourniquet / EBL: [Tourniquet] / minimal Adjuncts: Loupes, nerve stimulator Complications: None
Indications: [Age]yo [M/F] with [left/right] cubital tunnel syndrome (EMG-confirmed) refractory to conservative care [± nerve subluxation/intrinsic weakness]. [Transposition chosen for subluxation/valgus.] Risks (MABC neuroma, persistent symptoms, new compression) discussed.
Description of Procedure: After consent and time-out, [regional] anesthesia was given and the [tourniquet] inflated. A curvilinear medial elbow incision was made between the medial epicondyle and olecranon, protecting the medial antebrachial cutaneous nerve branches. The ulnar nerve was identified and all compression points released — the arcade of Struthers, the cubital tunnel retinaculum (Osborne), and the FCU aponeurosis.
[In situ: the release was confirmed adequate.] [Transposition: the nerve was mobilized preserving its segmental blood supply (dividing tethering articular branches, sparing FCU motor branches) and transposed anterior to the epicondyle (subcutaneous with a fascial sling / submuscular under the flexor-pronator origin), with a full-ROM check confirming no kinking/new compression.]
The tourniquet was released, hemostasis obtained, and closure performed [± splint]. The patient was discharged with early ROM.
Postoperative Plan
- Outpatient; soft dressing ± elbow splint (submuscular longer immobilization), elevate
- Early hand/finger ROM; elbow ROM progression per technique
- Suture removal ~10-14 days; therapy
- Counsel: sensory recovery before motor; atrophy/weakness slow to recover
- Follow-up 2 weeks
Chief-Level Case Review
Use these as the senior-level mental model for Cubital Tunnel Release / Ulnar Nerve Transposition:
- Decision point: Localization is everything: symptoms, exam, Tinel point, EMG/NCS, ultrasound/MRI, and provocative maneuvers must agree before incision.
- Technical lever: Protect fascicles and blood supply: internal neurolysis, tumor shelling, graft/transfer decisions, tourniquet time, and stimulation thresholds should be deliberate.
- Bailout: Know when not to chase: dense scarring, malignant features, unclear fascicular anatomy, or unexpected motor fascicle involvement may justify biopsy, subtotal resection, or staged reconstruction.
- Postop watch: Postop orders should preserve the repair: splint/immobilization interval, therapy timing, sensory protection, pain plan, and expected recovery timeline.
Common Pimp Questions
Use these to pressure-test preparation for Cubital Tunnel Release / Ulnar Nerve Transposition:
- Which nerve fascicles or branches must be identified before releasing or resecting tissue?
- What exam finding localizes the lesion and what alternative diagnosis could mimic it?
- What stimulation, ultrasound, microscope, tourniquet, or graft option should be ready?
- What motor/sensory function is at highest risk and how is it checked in PACU?
- What splint, therapy, wound, and neuropathic-pain plan should be written?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Tourniquet use, loupe versus microscope, stimulator settings, and incision length: [attending-specific]
- External neurolysis versus transposition/reconstruction threshold: [attending-specific]
- Graft/conduit/allograft availability and pathology handling: [attending-specific]
- Splinting position, therapy referral, and activity restrictions: [attending-specific]