
Case Prep: Carpal Tunnel Release
Case / Approach Snapshot
- Anatomy at risk: nerve course, fascicles, compression points, motor and sensory branches, adjacent vessels, scar planes, and distal targets for repair or transfer.
- Operative steps: mark landmarks, expose normal nerve proximally/distally, decompress or mobilize gently, resect/repair/graft/transfer as indicated, verify tension-free alignment, and close to protect gliding tissue; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: iatrogenic nerve injury, neuroma or neuropathic pain, vascular injury, incomplete decompression, recurrence, wound problems, and therapy/splinting or revision plan.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [left/right] carpal tunnel syndrome refractory to conservative management planned for [open / endoscopic] carpal tunnel release (median nerve decompression at the wrist).
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
CNS Video Library
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Carpal Tunnel Syndrome — Rotem G. The Israel Medical Association journal : IMAJ 2023. PubMed
- [Carpal tunnel syndrome] — Koehl P. MMW Fortschritte der Medizin 2022. PubMed
- Carpal tunnel syndrome — Middleton SD. BMJ (Clinical research ed.) 2014. PubMed
- Carpal Tunnel Syndrome — Alvarez CA. American family physician 2024. PubMed
- Carpal Tunnel Syndrome and Distal Radius Fractures — Pope D. Hand clinics 2018. PubMed
- Acute Carpal Tunnel Syndrome and Median Nerve Neurapraxia: A Review — Holbrook HS. The Orthopedic clinics of North America 2022. PubMed
- Carpal Tunnel Syndrome: Making Evidence-Based Treatment Decisions — Calandruccio JH. The Orthopedic clinics of North America 2018. PubMed
- [Carpal Tunnel Syndrome] — Erni S. Praxis 2023. PubMed
- Recurrent carpal tunnel syndrome — Mosier BA. Hand clinics 2013. PubMed
- Carpal tunnel syndrome — Belmonte K. Journal of the American Academy of Nurse Practitioners 1996. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
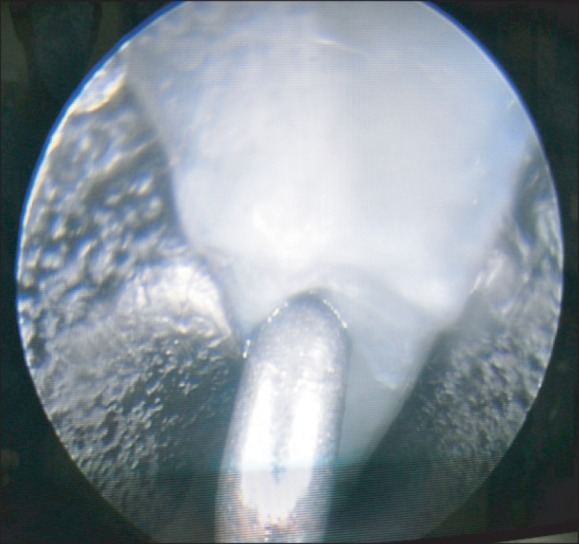 Fig. 2. Undersurface of transverse carpal ligament with washboard appearance. Source: Current Approaches for Carpal Tunnel Syndrome — Clinics in Orthopedic Surgery 2014; CC BY-NC.
Fig. 2. Undersurface of transverse carpal ligament with washboard appearance. Source: Current Approaches for Carpal Tunnel Syndrome — Clinics in Orthopedic Surgery 2014; CC BY-NC.
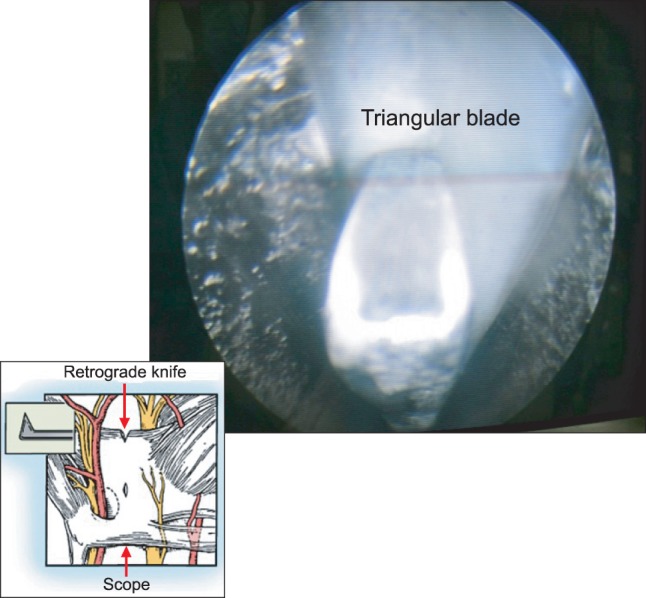 Fig. 3. Triangular blade cutting the middle of the transverse carpal ligament in retrograde fashion. Source: Current Approaches for Carpal Tunnel Syndrome — Clinics in Orthopedic Surgery 2014; CC BY-NC.
Fig. 3. Triangular blade cutting the middle of the transverse carpal ligament in retrograde fashion. Source: Current Approaches for Carpal Tunnel Syndrome — Clinics in Orthopedic Surgery 2014; CC BY-NC.
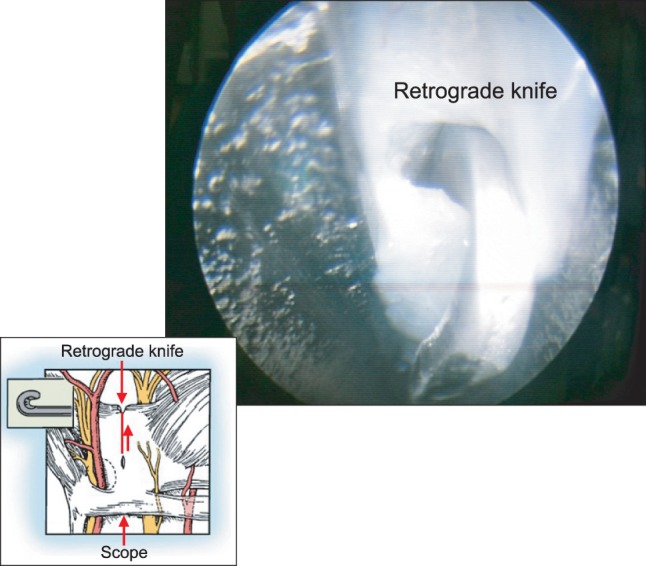 Fig. 4. Transection of the transverse carpal ligament by using a retrograde knife. Source: Current Approaches for Carpal Tunnel Syndrome — Clinics in Orthopedic Surgery 2014; CC BY-NC.
Fig. 4. Transection of the transverse carpal ligament by using a retrograde knife. Source: Current Approaches for Carpal Tunnel Syndrome — Clinics in Orthopedic Surgery 2014; CC BY-NC.
 Figure 5. Source: Current Approaches for Carpal Tunnel Syndrome — Clin Orthop Surg. 2014 Aug 5;6(3):253–7. doi: 10.4055/cios.2014.6.3.253; CC BY-NC.
Figure 5. Source: Current Approaches for Carpal Tunnel Syndrome — Clin Orthop Surg. 2014 Aug 5;6(3):253–7. doi: 10.4055/cios.2014.6.3.253; CC BY-NC.
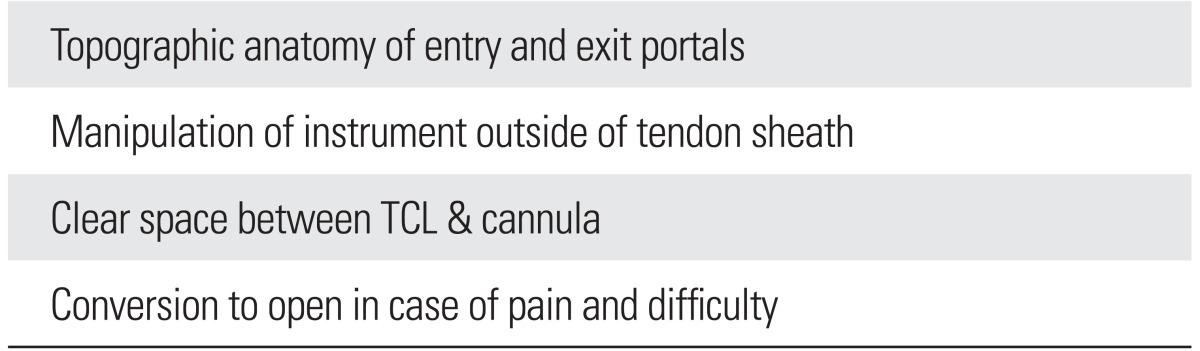 Figure 6. Source: Current Approaches for Carpal Tunnel Syndrome — Clin Orthop Surg. 2014 Aug 5;6(3):253–7. doi: 10.4055/cios.2014.6.3.253; CC BY-NC.
Figure 6. Source: Current Approaches for Carpal Tunnel Syndrome — Clin Orthop Surg. 2014 Aug 5;6(3):253–7. doi: 10.4055/cios.2014.6.3.253; CC BY-NC.
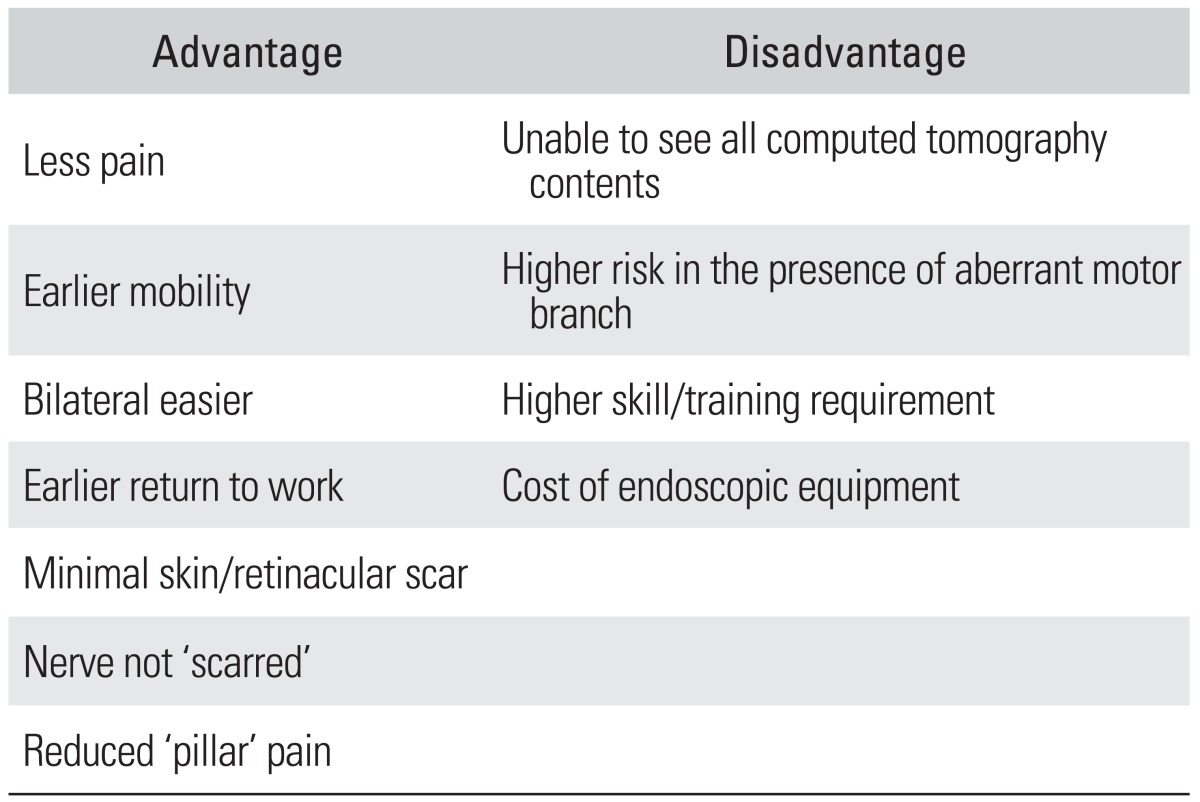 Figure 7. Source: Current Approaches for Carpal Tunnel Syndrome — Clin Orthop Surg. 2014 Aug 5;6(3):253–7. doi: 10.4055/cios.2014.6.3.253; CC BY-NC.
Figure 7. Source: Current Approaches for Carpal Tunnel Syndrome — Clin Orthop Surg. 2014 Aug 5;6(3):253–7. doi: 10.4055/cios.2014.6.3.253; CC BY-NC.
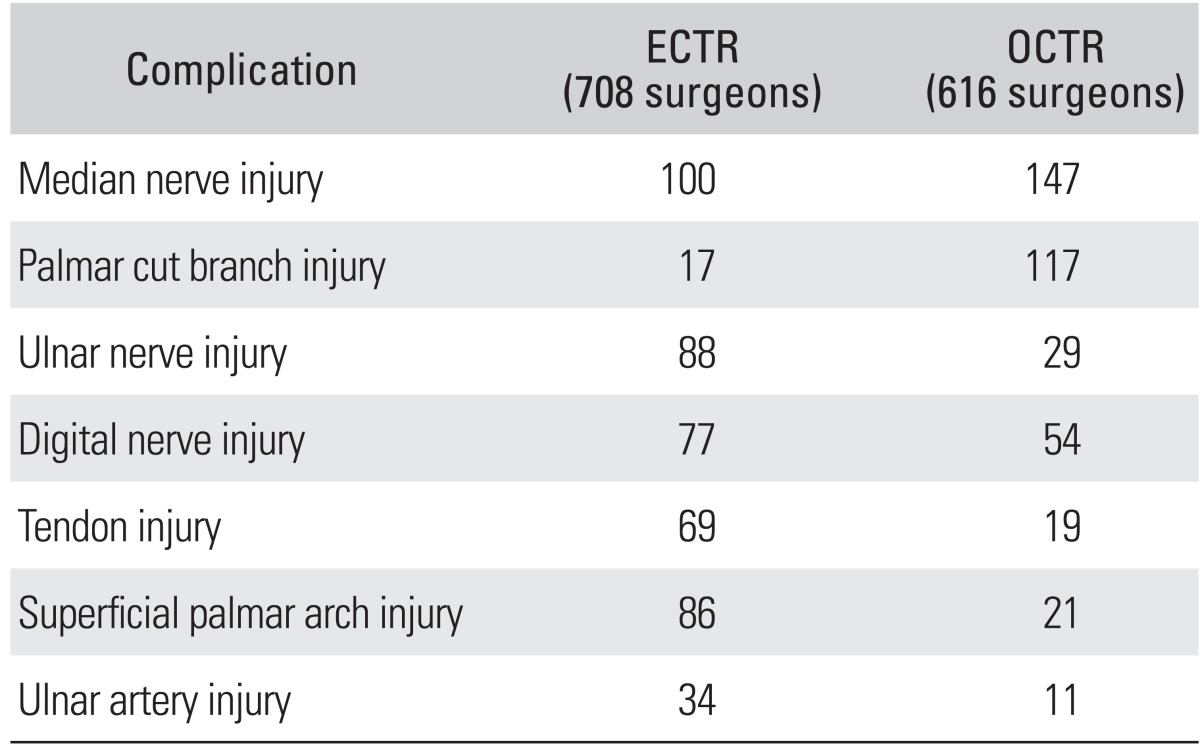 Figure 8. Source: Current Approaches for Carpal Tunnel Syndrome — Clin Orthop Surg. 2014 Aug 5;6(3):253–7. doi: 10.4055/cios.2014.6.3.253; CC BY-NC.
Figure 8. Source: Current Approaches for Carpal Tunnel Syndrome — Clin Orthop Surg. 2014 Aug 5;6(3):253–7. doi: 10.4055/cios.2014.6.3.253; CC BY-NC.
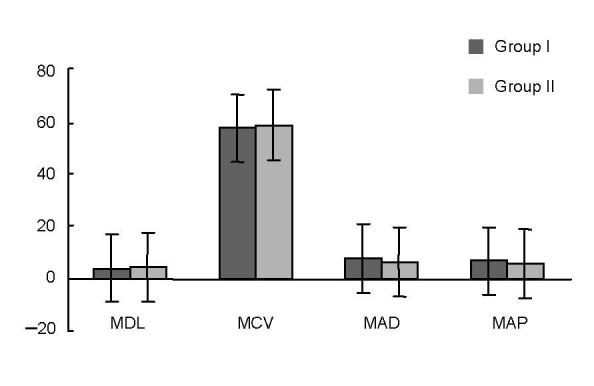 Figure 1. Results of median motor nerve studies in patients with carpal tunnel syndrome.Data are expressed as mean ± SD. Group I had minimal carpal tunnel syndrome, and group II had mild or… Source: Axonal degeneration of the ulnar nerve secondary to carpal tunnel syndrome: fact or fiction?☆ — Neural Regeneration Research 2013; CC BY-NC-SA.
Figure 1. Results of median motor nerve studies in patients with carpal tunnel syndrome.Data are expressed as mean ± SD. Group I had minimal carpal tunnel syndrome, and group II had mild or… Source: Axonal degeneration of the ulnar nerve secondary to carpal tunnel syndrome: fact or fiction?☆ — Neural Regeneration Research 2013; CC BY-NC-SA.
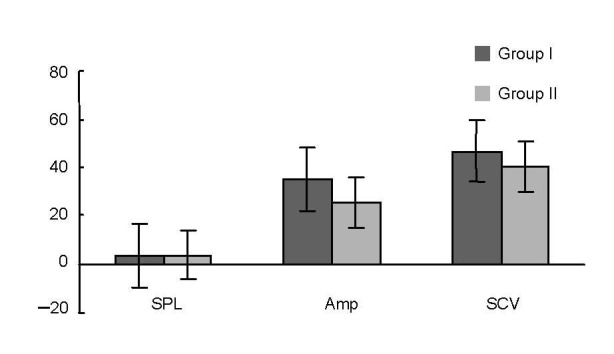 Figure 2. Results of median sensory nerve studies in patients with carpal tunnel syndrome.Data are expressed as mean ± SD. Group I had minimal carpal tunnel syndrome, and group II had mild or… Source: Axonal degeneration of the ulnar nerve secondary to carpal tunnel syndrome: fact or fiction?☆ — Neural Regeneration Research 2013; CC BY-NC-SA.
Figure 2. Results of median sensory nerve studies in patients with carpal tunnel syndrome.Data are expressed as mean ± SD. Group I had minimal carpal tunnel syndrome, and group II had mild or… Source: Axonal degeneration of the ulnar nerve secondary to carpal tunnel syndrome: fact or fiction?☆ — Neural Regeneration Research 2013; CC BY-NC-SA.
History of Present Illness
- Chief complaint: Numbness/tingling in median distribution (thumb, index, middle, radial ring), worse at night, shaking relieves (flick sign), dropping objects, thenar weakness
- Provocative: driving, phone, repetitive use
- Failed conservative: night splinting, NSAIDs, steroid injection, activity modification
- Thenar atrophy/weakness (advanced)
Past Medical History
- Diabetes, hypothyroidism, RA, pregnancy, obesity, amyloidosis, prior wrist trauma/fracture
- Bilateral symptoms, prior CTR
- Standard PMH
Imaging / Studies
EMG/NCS
- Median neuropathy at the wrist — prolonged distal motor/sensory latencies, confirms diagnosis and severity, excludes proximal/cervical cause
Ultrasound/MRI (selective)
- Median nerve cross-sectional area, masses, anatomy
Labs
- Per comorbidity (glucose, TSH); routine pre-op as needed
Neurological Examination
- Median sensory (2-point, monofilament), thenar strength (APB), atrophy, Tinel (wrist), Phalen, Durkan compression test; exclude cervical/proximal
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: hand table or radiolucent arm board, tourniquet when used, loupes/microscope available for nerve repair/tumor work, bipolar, microsuture/nerve-wrap options, and nerve stimulator for plexus or motor-branch cases.
- Special needs: regional/local/WALANT versus general anesthesia plan, antibiotic decision for implants/long exposure, anticoagulation plan, and clear laterality/site marking with preop motor/sensory baseline documented.
- Immediate postop orders: elevation, soft dressing or splint duration, early finger/limb ROM unless repair restricts it, oral analgesia, wound check/suture removal timing, therapy referral, and return precautions for hematoma or new motor deficit.
Procedure Selection
- Open CTR: direct visualization of transverse carpal ligament and nerve; gold standard, low complication
- Endoscopic CTR: smaller incision, faster recovery, but less direct visualization (nerve injury risk if anatomy unclear)
Operate vs Continue Nonoperative Care
- Proceed to surgery: persistent symptoms despite splinting/injection, EMG/NCS moderate-severe CTS, thenar weakness/atrophy, denervation, recurrent nighttime symptoms affecting function, or acute CTS.
- Consider injection/splinting first: mild intermittent symptoms, pregnancy-associated CTS, short duration without weakness, or high medical/wound risk.
- Urgent release: acute CTS after distal radius fracture, burn/compartment swelling, hemorrhage, infection, or rapidly progressive median nerve deficit.
- Revision workup: persistent symptoms suggest incomplete release or wrong diagnosis; recurrent symptoms after relief suggest scar/fibrosis, tenosynovitis, amyloid, mass, or systemic disease.
Anatomy Variants to Expect
- Recurrent motor branch can be extraligamentous, subligamentous, or transligamentous; the transligamentous branch is the trap during TCL division.
- Palmar cutaneous branch travels radial/proximal and is vulnerable to incisions crossing the wrist crease or radial dissection.
- Berrettini communicating branch between median and ulnar digital nerves can cross the distal field.
- Persistent median artery, bifid median nerve, synovial hypertrophy, ganglion, and anomalous muscle belly can explain atypical symptoms or intraoperative findings.
Position & Anesthesia
- Supine, arm on hand table, tourniquet, local/WALANT (wide-awake local anesthesia no tourniquet) or local + sedation / regional
Key Surgical Steps (Open)
- Tourniquet, exsanguinate, local anesthesia
- Longitudinal incision in line with the radial border of the ring finger, in the palm, ulnar to the thenar crease (avoid recurrent motor branch and palmar cutaneous branch — stay ulnar to midline), not crossing the wrist flexion crease at 90 degrees (or curve it)
- Divide skin, palmar fascia
- Identify the transverse carpal ligament (flexor retinaculum)
- Incise the TCL completely along its ulnar aspect under direct vision, from distal to proximal, protecting the median nerve beneath
- Confirm complete release proximally (antebrachial fascia) and distally (palmar fat) — nerve fully decompressed
- Inspect nerve, ensure no mass/anomaly; do NOT routinely neurolyse
- Release tourniquet, hemostasis, skin closure (nylon), soft dressing/splint
Completeness Check
- Distal release ends when palmar fat is seen and no distal band remains over the median nerve/common digital branches.
- Proximal release includes the distal antebrachial fascia enough to remove the proximal constriction without injuring the palmar cutaneous branch.
- The median nerve should be decompressed without routine internal neurolysis; external neurolysis is reserved for scarred revision or clear constricting tissue.
- If symptoms were atypical or severe, inspect for mass, synovitis, anomalous muscle, persistent median artery, or bifid nerve.
- Before closure, range the wrist/fingers gently and ensure no sharp fascial edge or hematoma compresses the nerve.
Critical Anatomy & Structures at Risk
- Median nerve (deep to TCL)
- Recurrent motor (thenar) branch — variable (extraligamentous/transligamentous/subligamentous); stay ulnar to avoid
- Palmar cutaneous branch of median (proximal, radial — incision placement)
- Superficial palmar arch (distal — don’t plunge), common digital nerves
- Ulnar nerve/artery (Guyon canal — ulnar; stay controlled)
Equipment
- Minor hand set, tourniquet, loupes, bipolar
- Endoscopic CTR system (if endoscopic)
Anesthesia
- Local/WALANT/regional ± sedation; antibiotics typically not required for clean soft-tissue (per practice)
Potential Complications
- Nerve injury (median/recurrent motor/palmar cutaneous — painful neuroma, thenar weakness)
- Incomplete release (persistent symptoms), pillar pain, scar tenderness
- Vascular injury (superficial arch), bowstringing (rare), CRPS, infection, stiffness
Rescue and Revision Logic
- Immediate thenar weakness after release: suspect recurrent motor branch injury or severe pre-existing denervation; examine early and consider exploration if an iatrogenic injury is plausible.
- Persistent numbness without improvement: review pre-op severity, confirm complete release, and reassess cervical radiculopathy, pronator syndrome, polyneuropathy, diabetes, or amyloid.
- Recurrent symptoms after a symptom-free interval: suspect scar tethering, recurrent synovitis, incomplete distal/proximal release, or new systemic driver; ultrasound/MRI and repeat EMG help.
- Pillar pain: reassure and treat with time, scar massage, desensitization, therapy, and activity progression; avoid premature revision for isolated pillar pain.
- CRPS concern: early recognition, hand therapy, pain management, edema control, and avoid prolonged immobilization.
Operative Note Template
Preoperative Diagnosis: [Left/Right] carpal tunnel syndrome (median neuropathy at the wrist)
Postoperative Diagnosis: Same
Procedure: [Open/Endoscopic] [left/right] carpal tunnel release
Surgeon / Assistant: Anesthesia: [Local/WALANT / regional ± sedation] Tourniquet / EBL: [Tourniquet] / minimal Adjuncts: Loupes [endoscopic CTR system if endoscopic] Complications: None
Indications: [Age]yo [M/F] with [left/right] carpal tunnel syndrome (EMG-confirmed) refractory to splinting/injection [± thenar weakness/atrophy]. Risks (nerve injury, incomplete release, pillar pain) discussed.
Description of Procedure: After consent and time-out, [local/WALANT] anesthesia was given and the [tourniquet] inflated. A longitudinal palmar incision in line with the radial border of the ring finger, ulnar to the thenar crease (avoiding the recurrent motor and palmar cutaneous branches) was made through skin and palmar fascia, exposing the transverse carpal ligament. The TCL was completely divided along its ulnar aspect under direct vision, distal to proximal, protecting the median nerve beneath. Complete release was confirmed proximally (antebrachial fascia) and distally (palmar fat), with the nerve decompressed and no anomaly/mass.
The tourniquet was released, hemostasis obtained, and the skin closed. A soft dressing was applied. The patient was discharged with early finger ROM.
Postoperative Plan
- Outpatient; soft dressing/volar splint briefly, elevate, finger ROM immediately
- Suture removal ~10-14 days; expect night symptoms to improve quickly, strength/atrophy slower
- Activity progression, scar massage, pillar pain counseling
- Follow-up 2 weeks; therapy if needed
Chief-Level Case Review
Use these as the senior-level mental model for Carpal Tunnel Release:
- Decision point: Localization is everything: symptoms, exam, Tinel point, EMG/NCS, ultrasound/MRI, and provocative maneuvers must agree before incision.
- Technical lever: Protect fascicles and blood supply: internal neurolysis, tumor shelling, graft/transfer decisions, tourniquet time, and stimulation thresholds should be deliberate.
- Bailout: Know when not to chase: dense scarring, malignant features, unclear fascicular anatomy, or unexpected motor fascicle involvement may justify biopsy, subtotal resection, or staged reconstruction.
- Postop watch: Postop orders should preserve the repair: splint/immobilization interval, therapy timing, sensory protection, pain plan, and expected recovery timeline.
Common Pimp Questions
Use these to pressure-test preparation for Carpal Tunnel Release:
- Which nerve fascicles or branches must be identified before releasing or resecting tissue?
- What exam finding localizes the lesion and what alternative diagnosis could mimic it?
- What stimulation, ultrasound, microscope, tourniquet, or graft option should be ready?
- What motor/sensory function is at highest risk and how is it checked in PACU?
- What splint, therapy, wound, and neuropathic-pain plan should be written?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Tourniquet use, loupe versus microscope, stimulator settings, and incision length: [attending-specific]
- External neurolysis versus transposition/reconstruction threshold: [attending-specific]
- Graft/conduit/allograft availability and pathology handling: [attending-specific]
- Splinting position, therapy referral, and activity restrictions: [attending-specific]