
Case Prep: Brachial Plexus Injury — Exploration, Repair, Grafting, and Nerve Transfer
Case / Approach Snapshot
- Anatomy at risk: nerve course, fascicles, compression points, motor and sensory branches, adjacent vessels, scar planes, and distal targets for repair or transfer.
- Operative steps: mark landmarks, expose normal nerve proximally/distally, decompress or mobilize gently, resect/repair/graft/transfer as indicated, verify tension-free alignment, and close to protect gliding tissue; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: iatrogenic nerve injury, neuroma or neuropathic pain, vascular injury, incomplete decompression, recurrence, wound problems, and therapy/splinting or revision plan.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [traumatic / obstetric / tumor] [left/right] brachial plexus injury ([upper trunk / pan-plexus / preganglionic vs postganglionic]) planned for brachial plexus exploration with [neurolysis / direct repair / nerve grafting / nerve transfer (neurotization)].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Spinal accessory nerve transfer for shoulder abduction has no benefit over supraclavicular exploration and nerve grafting in brachial plexus birth injury: a systematic review — Mendiratta D. Frontiers in pediatrics 2024. PubMed
- Treatment of brachial plexus injury — Nagano A. Journal of orthopaedic science : official journal of the Japanese Orthopaedic Association 1998. PubMed
- Management of Adult Traumatic Brachial Plexus Injury — Datta NK. Mymensingh medical journal : MMJ 2023. PubMed
- Management of Adult Brachial Plexus Injuries — Hill JR. The Journal of hand surgery 2021. PubMed
- High radial nerve palsy — Laulan J. Hand surgery & rehabilitation 2019. PubMed
- Traumatic upper plexus palsy: Is the exploration of brachial plexus necessary? — Gkiatas I. European journal of orthopaedic surgery & traumatology : orthopedie traumatologie 2019. PubMed
- Combined injury of the accessory nerve and brachial plexus — Bertelli JA. Neurosurgery 2011. PubMed
- Adjunctive Dorsal Scapular Nerve Transfer to Suprascapular Nerve for Brachial Plexus Birth Injuries: Case Series — Augustine HFM. The Journal of hand surgery 2019. PubMed
- Proximal and Distal Nerve Transfers in the Management of Brachial Plexus Injuries — Woo SJ. Clinics in plastic surgery 2024. PubMed
- A systematic review of nerve transfer and nerve repair for the treatment of adult upper brachial plexus injury — Yang LJ. Neurosurgery 2012. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
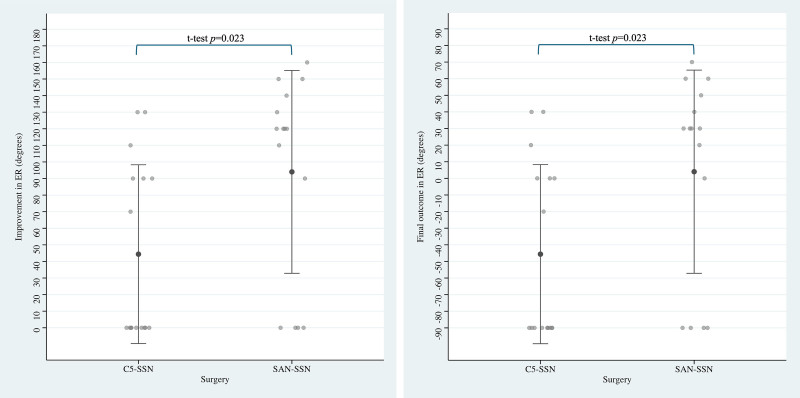 Fig. 2.. (Left) Improvement and (right) final outcome in active shoulder ER range of motion in degrees after brachial plexus reconstruction surgery with C5–SSN or SAN–SSN. Gray dots represent… Source: Comparison of Spinal Accessory Nerve Transfer versus C5 Grafting for Suprascapular Nerve Reinnervation in Brachial Plexus Birth Injury — Plastic and Reconstructive Surgery 2025; CC BY.
Fig. 2.. (Left) Improvement and (right) final outcome in active shoulder ER range of motion in degrees after brachial plexus reconstruction surgery with C5–SSN or SAN–SSN. Gray dots represent… Source: Comparison of Spinal Accessory Nerve Transfer versus C5 Grafting for Suprascapular Nerve Reinnervation in Brachial Plexus Birth Injury — Plastic and Reconstructive Surgery 2025; CC BY.
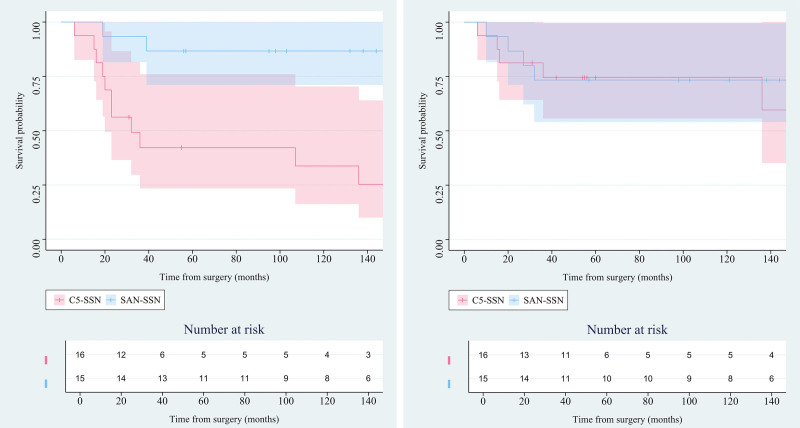 Fig. 3.. (Left) Survival probability without secondary surgery for shoulder ER after brachial plexus reconstruction surgery with C5–SSN or SAN–SSN, with 95% confidence intervals. Secondary… Source: Comparison of Spinal Accessory Nerve Transfer versus C5 Grafting for Suprascapular Nerve Reinnervation in Brachial Plexus Birth Injury — Plastic and Reconstructive Surgery 2025; CC BY.
Fig. 3.. (Left) Survival probability without secondary surgery for shoulder ER after brachial plexus reconstruction surgery with C5–SSN or SAN–SSN, with 95% confidence intervals. Secondary… Source: Comparison of Spinal Accessory Nerve Transfer versus C5 Grafting for Suprascapular Nerve Reinnervation in Brachial Plexus Birth Injury — Plastic and Reconstructive Surgery 2025; CC BY.
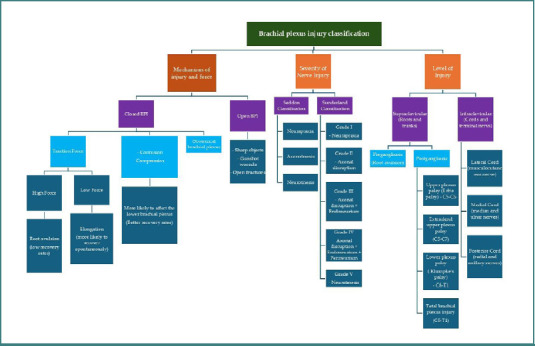 Figure 1. Classification of brachial plexus injuries [3,7,21,22] Source: Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study — Journal of Medicine and Life 2025; CC BY.
Figure 1. Classification of brachial plexus injuries [3,7,21,22] Source: Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study — Journal of Medicine and Life 2025; CC BY.
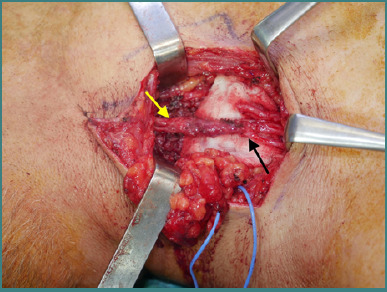 Figure 2. Spinal accessory to suprascapular nerve transfer. The yellow arrow points towards the spinal accessory nerve, and the black arrow points towards the suprascapular nerve. Source: Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study — Journal of Medicine and Life 2025; CC BY.
Figure 2. Spinal accessory to suprascapular nerve transfer. The yellow arrow points towards the spinal accessory nerve, and the black arrow points towards the suprascapular nerve. Source: Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study — Journal of Medicine and Life 2025; CC BY.
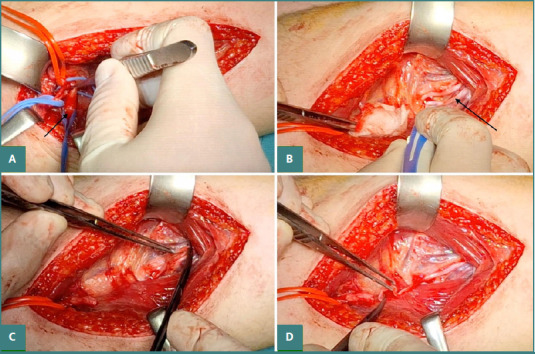 Figure 3. Radial nerve fascicle to axillary nerve transfer. A, Axillary nerve identification (black arrow); B, Radial nerve fascicle identification with nerve stimulator (black arrow pointing… Source: Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study — Journal of Medicine and Life 2025; CC BY.
Figure 3. Radial nerve fascicle to axillary nerve transfer. A, Axillary nerve identification (black arrow); B, Radial nerve fascicle identification with nerve stimulator (black arrow pointing… Source: Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study — Journal of Medicine and Life 2025; CC BY.
 Figure 4. Intercostal nerves to the musculocutaneous nerve transfer. A, Intercostal nerve harvested for transfer (black arrow); B, Musculocutaneous nerve identification (black arrow); C,… Source: Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study — Journal of Medicine and Life 2025; CC BY.
Figure 4. Intercostal nerves to the musculocutaneous nerve transfer. A, Intercostal nerve harvested for transfer (black arrow); B, Musculocutaneous nerve identification (black arrow); C,… Source: Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study — Journal of Medicine and Life 2025; CC BY.
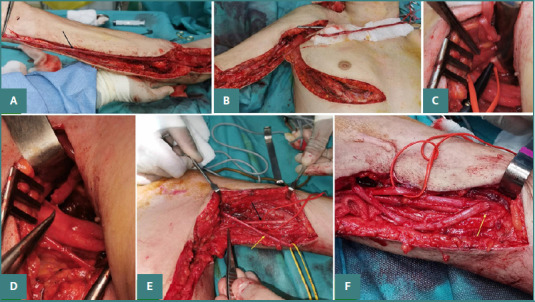 Figure 5. Contralateral C7 to median nerve transfer A, Ulnar nerve harvested for transfer (black arrow); B, Ulnar nerve reflected towards contralateral C7 through a subcutaneous tunnel C; C, C7… Source: Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study — Journal of Medicine and Life 2025; CC BY.
Figure 5. Contralateral C7 to median nerve transfer A, Ulnar nerve harvested for transfer (black arrow); B, Ulnar nerve reflected towards contralateral C7 through a subcutaneous tunnel C; C, C7… Source: Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study — Journal of Medicine and Life 2025; CC BY.
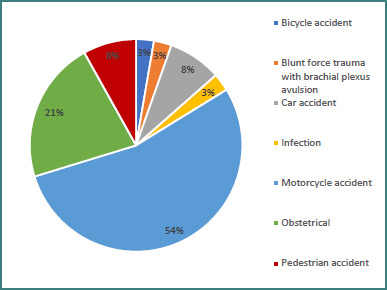 Figure 6. Mechanism of injury to the brachial plexus Source: Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study — Journal of Medicine and Life 2025; CC BY.
Figure 6. Mechanism of injury to the brachial plexus Source: Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study — Journal of Medicine and Life 2025; CC BY.
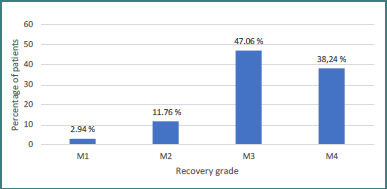 Figure 7. Global shoulder function recovery grade Source: Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study — Journal of Medicine and Life 2025; CC BY.
Figure 7. Global shoulder function recovery grade Source: Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study — Journal of Medicine and Life 2025; CC BY.
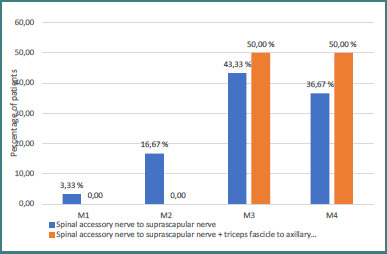 Figure 8. Global shoulder function recovery in relation to the surgical procedure used Source: Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study — Journal of Medicine and Life 2025; CC BY.
Figure 8. Global shoulder function recovery in relation to the surgical procedure used Source: Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study — Journal of Medicine and Life 2025; CC BY.
History of Present Illness
- Chief complaint: Flail/weak arm, sensory loss, neuropathic pain after [traction injury (MVC/motorcycle), penetrating, obstetric, gunshot, traction]
- Timing is critical — mechanism, date of injury (window for repair before irreversible motor endplate loss, ~6-12 months; nerve transfers time-sensitive)
- Pattern: upper trunk (C5-6 ± C7, Erb) vs lower (C8-T1, Klumpke) vs pan-plexus; supraclavicular vs infraclavicular
- Preganglionic (root avulsion — non-repairable directly) vs postganglionic (graftable) — distinguishing features below
- Pain, prior recovery/plateau, associated vascular/orthopedic injury
Past Medical History
- Associated injuries (subclavian/axillary vessels, clavicle/scapula fractures, head/chest), prior surgery
- Standard PMH; smoking (affects nerve healing)
Imaging Review
MRI brachial plexus / CT myelogram
- Pseudomeningocele / root avulsion (preganglionic — CT myelogram/MRI shows nerve root avulsion, empty root sleeve) → poor prognosis, favors nerve transfer
- Continuity vs discontinuity of trunks/cords, neuroma, tumor
EMG/NCS (timed — usually ~3-4 weeks+ and serial)
- Localize lesion(s), preganglionic vs postganglionic clues, SNAPs preserved with absent motor = preganglionic (avulsion — cell body intact, root avulsed), denervation, reinnervation
- Identify viable donors for transfer
CTA (if vascular injury)
Labs
- CBC, BMP, Coags, type and screen
Neurological Examination
- Detailed motor (each muscle/myotome) and sensory mapping, Horner syndrome (preganglionic C8-T1 — ptosis/miosis/anhidrosis = poor prognosis), Tinel along plexus (advancing = regeneration), winging (long thoracic), rhomboids/serratus (very proximal = preganglionic)
- Document baseline meticulously, MRC grades
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: hand table or radiolucent arm board, tourniquet when used, loupes/microscope available for nerve repair/tumor work, bipolar, microsuture/nerve-wrap options, and nerve stimulator for plexus or motor-branch cases.
- Special needs: regional/local/WALANT versus general anesthesia plan, antibiotic decision for implants/long exposure, anticoagulation plan, and clear laterality/site marking with preop motor/sensory baseline documented.
- Immediate postop orders: elevation, soft dressing or splint duration, early finger/limb ROM unless repair restricts it, oral analgesia, wound check/suture removal timing, therapy referral, and return precautions for hematoma or new motor deficit.
Timing & Strategy
- Sharp/penetrating transection: early (acute) repair
- Closed traction injuries: observe with serial exam/EMG ~3 months; operate if no recovery (~3-6 months) before motor endplates degenerate (~12-18 months limit)
- Root avulsion (preganglionic): not directly repairable → nerve transfer (neurotization) prioritized
- Goals (prioritized): elbow flexion, shoulder abduction/stability, then hand if feasible
Position
- Supine, head turned away, arm/shoulder and both legs (sural nerve graft donor) prepped; possible interscalene/supraclavicular + infraclavicular exposure
Key Surgical Steps
- Exposure — supraclavicular (roots/trunks; protect phrenic nerve on anterior scalene, spinal accessory, EJV, subclavian vessels, thoracic duct on left) ± infraclavicular extension (cords/branches)
- Identify and trace plexus elements; intraoperative nerve stimulation and NAP (nerve action potential) recording across lesions (NAP across a neuroma-in-continuity → neurolysis; no NAP → resect and graft)
- Neurolysis (lesion in continuity conducting) — external/internal
- Direct repair (sharp transection, tension-free) — rare; or
- Nerve grafting (postganglionic rupture) — resect neuroma to healthy fascicles, interpositional sural nerve grafts bridge the gap
- Nerve transfers (neurotization) for avulsions/unrepairable proximal injury — examples:
- Oberlin transfer (ulnar nerve fascicle → biceps motor branch of musculocutaneous) for elbow flexion
- Spinal accessory → suprascapular nerve (shoulder)
- Double fascicular (median+ulnar → biceps/brachialis), triceps branch → axillary, intercostals → musculocutaneous, contralateral C7 (select)
- Tension-free coaptation under microscope (microsuture ± fibrin glue), tag/document
- Closure; protect repairs (positioning/immobilization)
Critical Anatomy & Structures at Risk
- Phrenic nerve (anterior scalene — diaphragm), spinal accessory (donor/at risk), long thoracic
- Subclavian/axillary vessels (exposure)
- Thoracic duct (left supraclavicular — chyle leak)
- Donor nerve function (transfers trade minor donor deficit for major recipient gain)
- Plexus elements (preserve conducting fascicles — NAP-guided)
Equipment
- Microscope, microsurgical instruments, nerve stimulator + NAP recording, microsuture, fibrin glue
- Sural nerve graft harvest set, loupes, bipolar
- Vessel loops, possible vascular backup
Monitoring
- Intraoperative nerve stimulation / NAP / SSEP (preganglionic localization)
Anesthesia
- No long-acting paralytic (stimulation/NAP), general; positioning for multiple donor sites
Potential Complications
- Incomplete/failed reinnervation (timing/avulsion-dependent), donor-site deficit
- Phrenic/accessory/vascular/thoracic duct injury (chylothorax), pneumothorax
- Neuropathic pain (avulsion — may need DREZ later), neuroma, CSF leak (avulsion repairs)
Operative Note Template
Preoperative Diagnosis: [Left/Right] [traumatic/obstetric] brachial plexus injury ([upper trunk/pan-plexus]; [pre-/postganglionic])
Postoperative Diagnosis: Same
Procedure: [Left/Right] brachial plexus exploration with [neurolysis / sural nerve grafting / nerve transfer(s) — e.g., Oberlin, SAN→SSN]
Surgeon / Assistant: Anesthesia: General, no long-acting paralytic EBL / Fluids: Adjuncts: Microscope, nerve stimulator + NAP recording, microsuture/fibrin glue, sural nerve graft harvest Complications: None
Indications: [Age]yo [M/F] with a [traumatic] brachial plexus injury and [no recovery at ~3–6 months / sharp transection], within the window for reconstruction. Goals prioritized: elbow flexion, shoulder stability. Risks (incomplete recovery, donor deficit, phrenic/vascular/thoracic-duct injury) discussed.
Description of Procedure: After consent and time-out, general anesthesia (no paralytic) was induced and both legs prepped for sural graft. A [supraclavicular ± infraclavicular] exposure was performed, protecting the phrenic and spinal accessory nerves, subclavian vessels, and thoracic duct. Plexus elements were traced and intraoperative stimulation/NAP recording assessed lesions across neuromas.
Lesions were addressed: [neurolysis for conducting lesions-in-continuity / interpositional sural nerve grafting after resecting non-conducting neuromas to healthy fascicles / nerve transfer(s) for avulsions — e.g., Oberlin (ulnar fascicle→biceps), spinal accessory→suprascapular]. Coaptations were performed tension-free under the microscope with microsuture [± fibrin glue], and the donor/recipient and graft source/length documented.
Hemostasis was obtained and closure performed; the repairs were protected with [positioning/immobilization]. A CXR excluded pneumothorax. The patient was counseled on the prolonged reinnervation timeline.
Postoperative Plan
- Floor, neurovascular checks, CXR (pneumothorax — supraclavicular), monitor for chyle leak (left)
- Immobilize/protect repairs per surgeon (limit tension across coaptations for weeks)
- Donor site (sural — sensory loss lateral foot) care
- Reinnervation is slow (~1 mm/day; months to years) — Tinel advancement, serial EMG, intensive OT/PT, motor re-education (esp. transfers)
- Pain management (neuropathic), counsel realistic timeline/expectations; long-term follow-up
Chief-Level Case Review
Use these as the senior-level mental model for Brachial Plexus Injury — Exploration, Repair, Grafting, and Nerve Transfer:
- Decision point: Localization is everything: symptoms, exam, Tinel point, EMG/NCS, ultrasound/MRI, and provocative maneuvers must agree before incision.
- Technical lever: Protect fascicles and blood supply: internal neurolysis, tumor shelling, graft/transfer decisions, tourniquet time, and stimulation thresholds should be deliberate.
- Bailout: Know when not to chase: dense scarring, malignant features, unclear fascicular anatomy, or unexpected motor fascicle involvement may justify biopsy, subtotal resection, or staged reconstruction.
- Postop watch: Postop orders should preserve the repair: splint/immobilization interval, therapy timing, sensory protection, pain plan, and expected recovery timeline.
Common Pimp Questions
Use these to pressure-test preparation for Brachial Plexus Injury — Exploration, Repair, Grafting, and Nerve Transfer:
- Which nerve fascicles or branches must be identified before releasing or resecting tissue?
- What exam finding localizes the lesion and what alternative diagnosis could mimic it?
- What stimulation, ultrasound, microscope, tourniquet, or graft option should be ready?
- What motor/sensory function is at highest risk and how is it checked in PACU?
- What splint, therapy, wound, and neuropathic-pain plan should be written?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Tourniquet use, loupe versus microscope, stimulator settings, and incision length: [attending-specific]
- External neurolysis versus transposition/reconstruction threshold: [attending-specific]
- Graft/conduit/allograft availability and pathology handling: [attending-specific]
- Splinting position, therapy referral, and activity restrictions: [attending-specific]