
Case Prep: Selective Dorsal Rhizotomy (SDR)
Case / Approach Snapshot
- Anatomy at risk: age-specific skull/soft tissue, developing brain and tracts, CSF pathways, brainstem/lower cranial nerves, tumor or congenital lesion relationships, and blood-volume constraints.
- Operative steps: adapt positioning/anesthesia to age, confirm imaging and goals with family, expose gently, preserve neurovascular/CSF pathways, reconstruct durably for growth, and plan ICU/endocrine/rehab surveillance; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: blood loss, hypothermia, swelling, hydrocephalus, airway/swallowing issues, endocrine/electrolyte shifts, infection, and staged therapy with oncology or rehab teams.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo child with spastic [diplegic/quadriplegic] cerebral palsy (GMFCS [I-III]) and lower-extremity spasticity impairing function planned for selective dorsal rhizotomy via [single-level conus / L1 limited] laminoplasty.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- SELECTIVE DORSAL RHIZOTOMY IN CEREBRAL PALSY: SELECTION CRITERIA AND POSTOPERATIVE PHYSICAL THERAPY PROTOCOLS — Nicolini-Panisson RD. Revista paulista de pediatria : orgao oficial da Sociedade de Pediatria de Sao Paulo 2018. PubMed
- Selective dorsal rhizotomy for spasticity of genetic etiology — Lohkamp LN. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2020. PubMed
- Selective dorsal rhizotomy: an illustrated review of operative techniques — Warsi NM. Journal of neurosurgery. Pediatrics 2020. PubMed
- State of the Evidence Traffic Lights 2019: Systematic Review of Interventions for Preventing and Treating Children with Cerebral Palsy — Novak I. Current neurology and neuroscience reports 2020. PubMed
- Cerebral Palsy: An Overview — Vitrikas K. American family physician 2020. PubMed
- Cauda Equina-Level Selective Dorsal Rhizotomy — Enslin JMN. Advances and technical standards in neurosurgery 2025. PubMed
- Selective dorsal rhizotomy — Engsberg JR. Journal of neurosurgery. Pediatrics 2008. PubMed
- The selective dorsal rhizotomy technique for spasticity in 2020: a review — Abbott R. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2020. PubMed
- The Evolution of Selective Dorsal Rhizotomy for the Management of Spasticity — Enslin JMN. Neurotherapeutics : the journal of the American Society for Experimental NeuroTherapeutics 2019. PubMed
- Selective dorsal rhizotomy: current state of practice and the role of imaging — Graham D. Quantitative imaging in medicine and surgery 2018. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
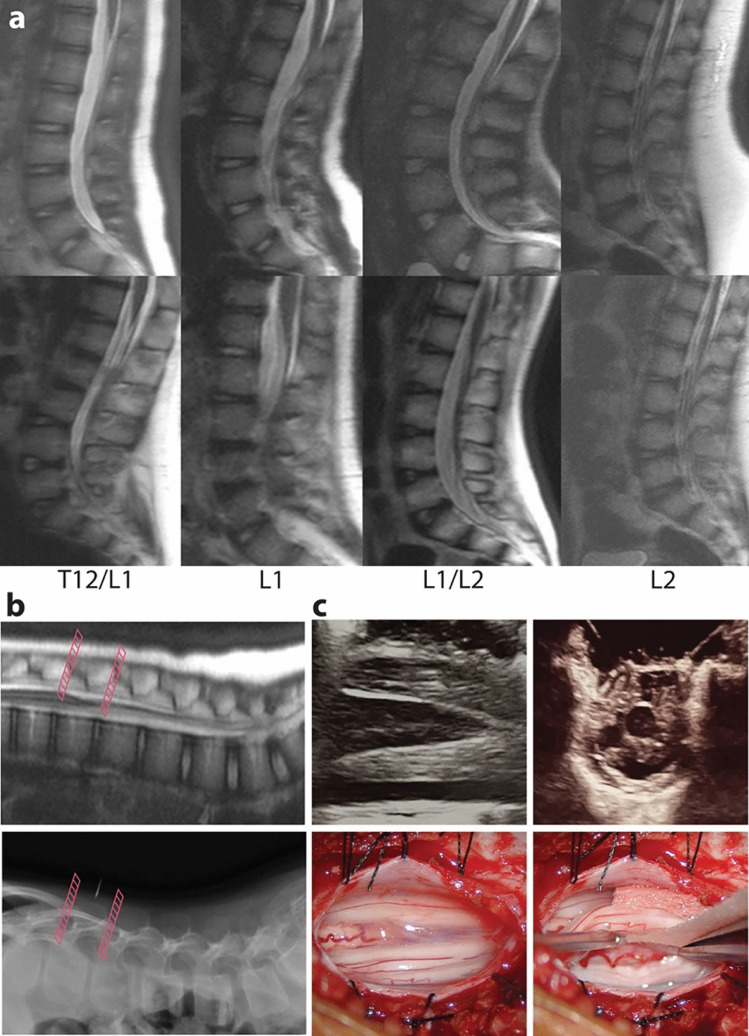 Fig. 1. Rapid MRI of the lumbar spine. a Representative examples of rapid MRI of the lumbar spine for conus localization. Sagittal SSH T2 images were chosen from 8 individual patients with conus… Source: Single-level laminoplasty approach to selective dorsal rhizotomy with conus localization by rapid spine MRI — Child’s Nervous System 2024; CC BY.
Fig. 1. Rapid MRI of the lumbar spine. a Representative examples of rapid MRI of the lumbar spine for conus localization. Sagittal SSH T2 images were chosen from 8 individual patients with conus… Source: Single-level laminoplasty approach to selective dorsal rhizotomy with conus localization by rapid spine MRI — Child’s Nervous System 2024; CC BY.
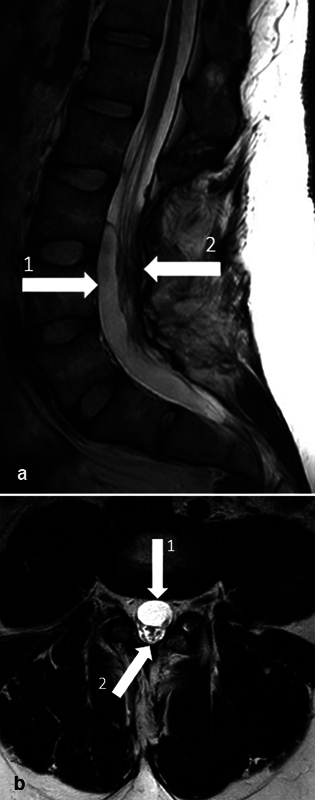 Fig. 1. Preoperative magnetic resonance imaging (MRI) of lumbosacral spine. ( a ) Sagittal view. 1, arachnoid cyst; 2, cauda equina. ( b ) Axial view. 1, arachnoid cyst; 2, cauda equina. Source: Arachnoid Cyst as a Late Complication of Selective Dorsal Rhizotomy: A Case Report — Journal of Neurological Surgery Reports 2024; CC BY.
Fig. 1. Preoperative magnetic resonance imaging (MRI) of lumbosacral spine. ( a ) Sagittal view. 1, arachnoid cyst; 2, cauda equina. ( b ) Axial view. 1, arachnoid cyst; 2, cauda equina. Source: Arachnoid Cyst as a Late Complication of Selective Dorsal Rhizotomy: A Case Report — Journal of Neurological Surgery Reports 2024; CC BY.
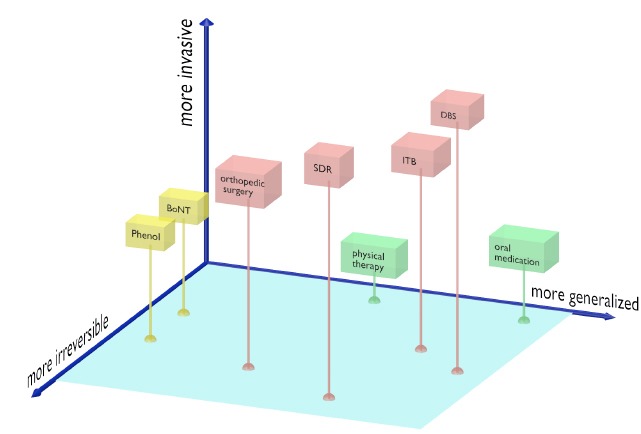 Fig. 1. Tone management options in cerebral palsy. Tone management is only one aspect of the musculoskeletal care needs of children with spastic cerebral palsy: lever arm dysfunction and joint… Source: Selective dorsal rhizotomy in ambulant children with cerebral palsy — Journal of Children’s Orthopaedics 2018; CC BY-NC.
Fig. 1. Tone management options in cerebral palsy. Tone management is only one aspect of the musculoskeletal care needs of children with spastic cerebral palsy: lever arm dysfunction and joint… Source: Selective dorsal rhizotomy in ambulant children with cerebral palsy — Journal of Children’s Orthopaedics 2018; CC BY-NC.
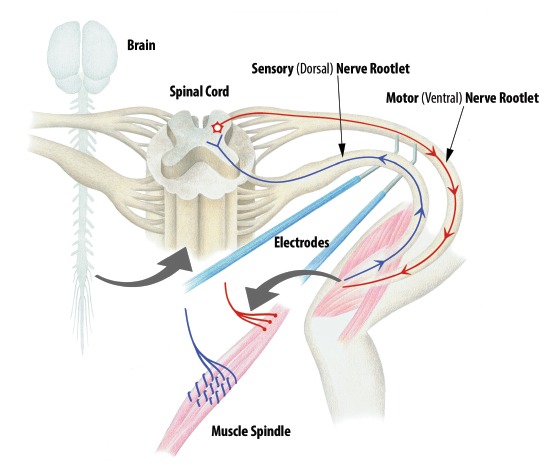 Fig. 2. Spasticity reflex arc schematic diagram. Muscle stretch stimulates dorsal (afferent) sensory nerve rootlets, which in turn has a net excitatory effect on alpha motor neurons within the… Source: Selective dorsal rhizotomy in ambulant children with cerebral palsy — Journal of Children’s Orthopaedics 2018; CC BY-NC.
Fig. 2. Spasticity reflex arc schematic diagram. Muscle stretch stimulates dorsal (afferent) sensory nerve rootlets, which in turn has a net excitatory effect on alpha motor neurons within the… Source: Selective dorsal rhizotomy in ambulant children with cerebral palsy — Journal of Children’s Orthopaedics 2018; CC BY-NC.
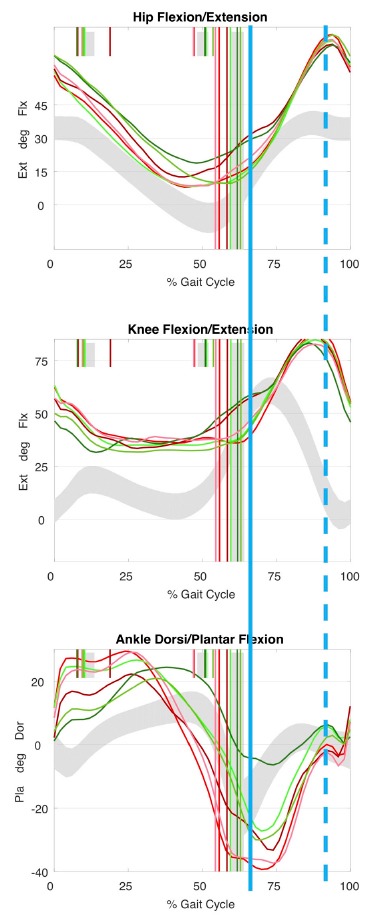 Fig. 3. Kinematic traces of ‘mass flexion (Flx)/extension (Ext)’. Mass flexion-extension is a primitive movement pattern suggesting reduced selective motor control. This can be seen typically… Source: Selective dorsal rhizotomy in ambulant children with cerebral palsy — Journal of Children’s Orthopaedics 2018; CC BY-NC.
Fig. 3. Kinematic traces of ‘mass flexion (Flx)/extension (Ext)’. Mass flexion-extension is a primitive movement pattern suggesting reduced selective motor control. This can be seen typically… Source: Selective dorsal rhizotomy in ambulant children with cerebral palsy — Journal of Children’s Orthopaedics 2018; CC BY-NC.
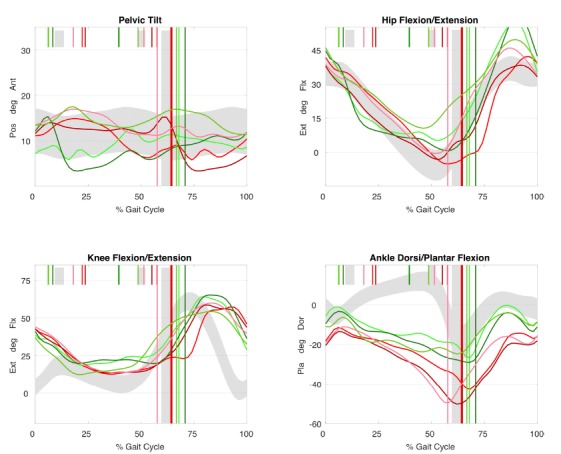 Fig. 4. Kinematic traces in dystonia. Uncontrollable movements in dystonia results in large cycle to cycle variations between individual cycles. This individual also walks with plantarflexed… Source: Selective dorsal rhizotomy in ambulant children with cerebral palsy — Journal of Children’s Orthopaedics 2018; CC BY-NC.
Fig. 4. Kinematic traces in dystonia. Uncontrollable movements in dystonia results in large cycle to cycle variations between individual cycles. This individual also walks with plantarflexed… Source: Selective dorsal rhizotomy in ambulant children with cerebral palsy — Journal of Children’s Orthopaedics 2018; CC BY-NC.
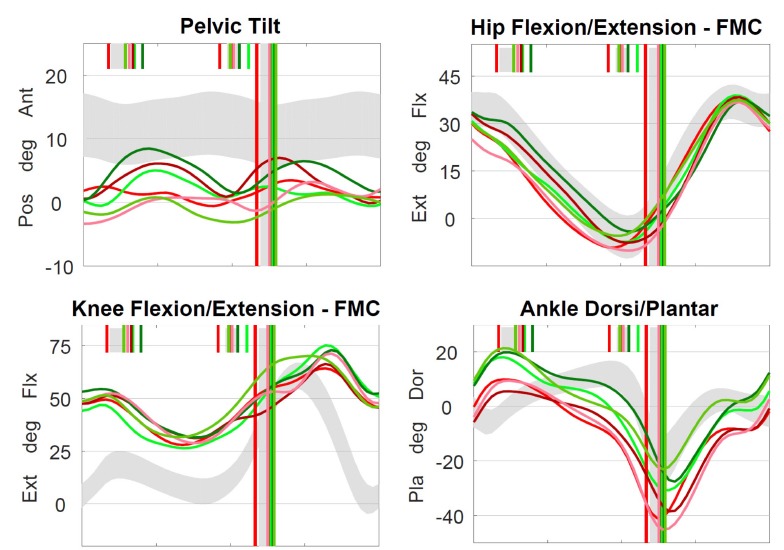 Fig. 5. Kinematic pattern of predominantly underlying spasticity affecting gait. ‘Double bump’ pelvis, slow and delayed knee flexion in early swing, reduced knee extension in late swing and… Source: Selective dorsal rhizotomy in ambulant children with cerebral palsy — Journal of Children’s Orthopaedics 2018; CC BY-NC.
Fig. 5. Kinematic pattern of predominantly underlying spasticity affecting gait. ‘Double bump’ pelvis, slow and delayed knee flexion in early swing, reduced knee extension in late swing and… Source: Selective dorsal rhizotomy in ambulant children with cerebral palsy — Journal of Children’s Orthopaedics 2018; CC BY-NC.
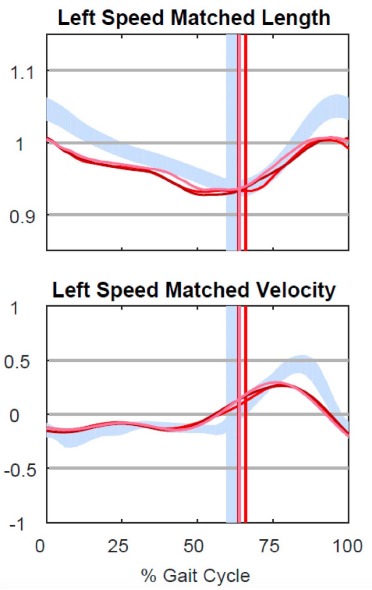 Fig. 6. Hamstring length. Musculotendinous length modelling can be performed given known muscle insertions and joint positions. Spasticity is associated with short hamstring length and slow… Source: Selective dorsal rhizotomy in ambulant children with cerebral palsy — Journal of Children’s Orthopaedics 2018; CC BY-NC.
Fig. 6. Hamstring length. Musculotendinous length modelling can be performed given known muscle insertions and joint positions. Spasticity is associated with short hamstring length and slow… Source: Selective dorsal rhizotomy in ambulant children with cerebral palsy — Journal of Children’s Orthopaedics 2018; CC BY-NC.
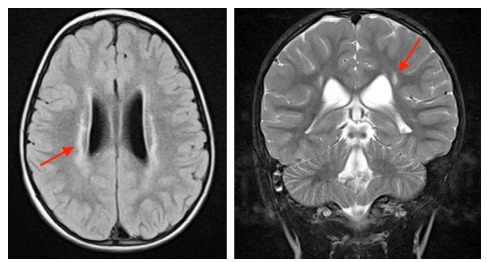 Fig. 7. Brain MRI in periventricular leukomalacia (PVL). The ‘ideal’ candidate for selective dorsal rhizotomy will have isolated PVL (red arrows). Source: Selective dorsal rhizotomy in ambulant children with cerebral palsy — Journal of Children’s Orthopaedics 2018; CC BY-NC.
Fig. 7. Brain MRI in periventricular leukomalacia (PVL). The ‘ideal’ candidate for selective dorsal rhizotomy will have isolated PVL (red arrows). Source: Selective dorsal rhizotomy in ambulant children with cerebral palsy — Journal of Children’s Orthopaedics 2018; CC BY-NC.
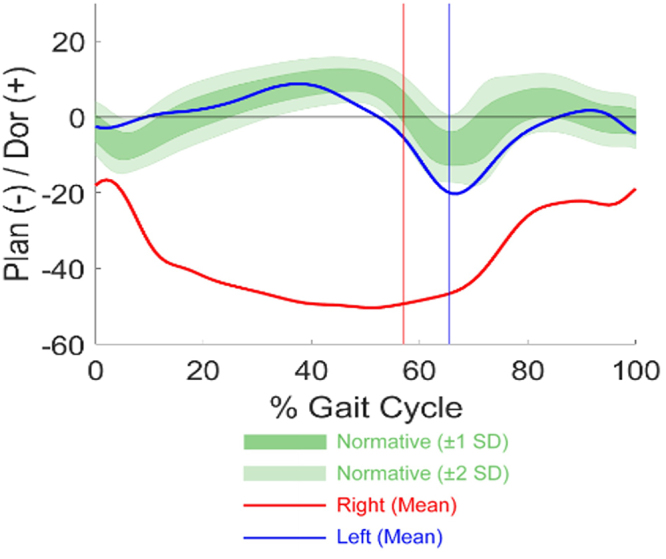 FIG. 1.. Preoperative ankle kinematics demonstrate excessive dynamic right plantar (Plan) flexion during stance and swing. Dor = dorsal. Source: Repeat selective dorsal rhizotomy for residual spasticity: illustrative case — Journal of Neurosurgery: Case Lessons 2025; CC BY-NC-ND.
FIG. 1.. Preoperative ankle kinematics demonstrate excessive dynamic right plantar (Plan) flexion during stance and swing. Dor = dorsal. Source: Repeat selective dorsal rhizotomy for residual spasticity: illustrative case — Journal of Neurosurgery: Case Lessons 2025; CC BY-NC-ND.
History of Present Illness
- Chief complaint: Lower-extremity spasticity (scissoring, toe-walking, crouch) impairing gait/function/care
- Ideal candidate: spastic diplegia from prematurity, good underlying strength and selective motor control, spasticity (not dystonia) as the dominant problem, age ~3-10, GMFCS II-III, motivated for intensive postop rehab
- Prior treatments (botulinum toxin, baclofen, orthopedic), gait analysis
- Multidisciplinary selection (neurosurgery, PT, physiatry, ortho)
Past Medical History
- Prematurity/PVL, prior orthopedic surgery, baclofen pump, dystonia component (relative contraindication), fixed contractures (ortho first), scoliosis
- Hip status (subluxation — caution; spasticity may be “holding” hips)
- Standard pediatric history
Imaging Review
MRI brain + spine
- PVL (typical), exclude other cause; spinal anatomy, conus level, exclude tethered cord/syrinx
Gait analysis / functional assessment
- Formal gait lab, spasticity (Ashworth), ROM, strength, selective motor control — baseline
Labs
- CBC, BMP, Coags, type and screen; pediatric pre-op
Neurological Examination
- Spasticity (Modified Ashworth) each muscle group, strength, selective motor control, ROM/contractures, gait, document baseline; distinguish spasticity vs dystonia
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: pediatric anesthesia/equipment, warming, weight-based implants/antibiotics, navigation/endoscope/microscope as needed, blood availability for tumor/myelomeningocele cases, and family-centered postop handoff.
- Special needs: weight-based fluids/meds, latex allergy precautions for myelomeningocele, steroid/endocrine/DI plan when sellar/posterior fossa risk exists, EVD/CSF diversion plan, and age-appropriate neuro baseline.
- Immediate postop orders: PICU/step-down neuro checks, airway/swallow monitoring when relevant, CT/MRI timing, drain/EVD/shunt orders, antibiotics/steroid taper, pain control, wound/skin precautions, and PT/OT/rehab planning.
Diagnosis & Indication
- Indication: Spastic diplegia with functional impairment, good strength/selective control, suitable for permanent spasticity reduction (SDR is permanent — vs reversible baclofen pump)
- Goal: Reduce spasticity by selectively cutting abnormal dorsal (sensory) rootlets that drive the spastic reflex arc, preserving strength and sensation
Candidate Selection
- Best candidates usually have spastic diplegia, meaningful antigravity strength, selective motor control, family commitment to intensive rehabilitation, and gait potential limited by spasticity rather than fixed deformity alone.
- Less favorable candidates include predominant dystonia/athetosis, severe weakness masked by tone, major contractures requiring orthopedic correction first, uncontrolled epilepsy/medical fragility, or unclear rehabilitation support.
- Clarify goals preoperatively: improved gait efficiency, easier care/hygiene, pain/spasm reduction, brace tolerance, or prevention of secondary deformity are different endpoints.
- Compare SDR against intrathecal baclofen when tone is generalized, mixed dystonia-spasticity is prominent, goals are care/comfort, or reversibility/adjustability matters.
Rootlet-Selection Strategy
- Build a level-by-level plan with physiatry, PT, and IONM before incision; intraoperative EMG refines the plan but should not replace the preoperative functional hypothesis.
- Preserve motor roots absolutely and treat sacral rootlets conservatively; bladder, bowel, and sexual function are not acceptable tradeoffs for marginal tone reduction.
- Avoid overcutting in a child who uses spasticity for stance; early postoperative weakness is expected, but excessive denervation can erase functional reserve.
- Document percent cut by level and side so later tone, weakness, sensory symptoms, or orthopedic planning can be interpreted correctly.
Position
- Prone, careful pediatric padding, IONM setup (EMG of multiple lower-extremity myotomes bilaterally, anal sphincter)
Key Surgical Steps (Single-Level / Conus technique)
- Localize the conus (fluoroscopy/ultrasound); limited laminoplasty (often single level over the conus, e.g., L1) — laminoplasty (replace lamina) preserves stability in children
- Midline durotomy, identify the conus and cauda equina
- Separate dorsal (sensory) from ventral (motor) roots — dorsal roots dorsolateral; confirm with stimulation (ventral roots = low-threshold motor; dorsal = sensory)
- Identify each dorsal root level (L1/L2-S1/S2) — use anatomic and stimulation mapping
- Divide each dorsal root into rootlets; stimulate each rootlet (EMG) and grade the response — abnormal/sustained/spreading (diffuse multisegmental) EMG responses = “abnormal” rootlets → transect; normal responses preserved
- Selectively cut ~25-50% of dorsal rootlets at targeted levels based on EMG abnormality (preserve sensory and all motor; preserve S2 and below carefully — bladder/sexual function)
- Confirm sphincter/sacral function preservation (monitor)
- Watertight dural closure, laminoplasty reconstruction, closure
Critical Anatomy & Structures at Risk
- Ventral (motor) roots — must preserve (only cut dorsal/sensory)
- S2-S4 (bladder/bowel/sexual function) — limit/avoid sacral sensory cutting; sphincter EMG
- Conus/cauda, dorsal columns (sensory — selective cutting preserves protective sensation)
- Dura (CSF leak), spinal stability (laminoplasty mitigates)
Equipment
- Microscope, intraoperative EMG (multichannel lower extremity + anal sphincter), nerve stimulator
- Micro-instruments, fine bipolar, ultrasound/fluoroscopy, dural substitute, laminoplasty fixation
Monitoring
- EMG-guided rootlet selection (the core of the procedure), sphincter EMG, SSEP — IONM is essential
Anesthesia
- No paralytic (EMG-dependent), TIVA (anesthesia that preserves EMG responses), pediatric, prone precautions
Potential Complications
- Transient sensory changes / dysesthesia (usually resolve), bladder dysfunction (sacral — avoid over-cutting)
- Weakness (if too aggressive / motor roots) — spasticity may have been providing functional support; transient post-op weakness common
- CSF leak, spinal deformity (long-term — scoliosis/lordosis surveillance), back pain
- Inadequate spasticity reduction / recurrence
Rescue and Postoperative Problem Solving
- Ventral/motor-root uncertainty: stop cutting until stimulation confirms anatomy; if separation is ambiguous, preserve the questionable rootlet.
- Sphincter EMG change or sacral concern: stop sacral sectioning, reassess stimulation thresholds, and accept a higher residual tone burden rather than risking bladder/bowel dysfunction.
- CSF leak/pseudomeningocele: flat protocol, wound pressure precautions, imaging if symptomatic, and early repair for persistent leak or wound compromise.
- Unexpected weakness: distinguish expected tone-unmasking from motor injury; protect joints, intensify rehab, check sensory/bladder status, and image if a compressive collection is possible.
- Residual spasticity: correlate with percent cut, untreated levels, dystonia, contracture, pain, and therapy adherence before labeling the rhizotomy a failure.
- Long-term deformity risk: continue spine/hip surveillance because reduced tone does not eliminate orthopedic progression in cerebral palsy.
Operative Note Template
Preoperative Diagnosis: Spastic [diplegic] cerebral palsy (GMFCS [__]) with disabling lower-extremity spasticity
Postoperative Diagnosis: Same
Procedure: Selective dorsal rhizotomy via [L1] limited laminoplasty with intraoperative EMG-guided rootlet selection
Surgeon / Assistant: Anesthesia: Total IV anesthesia (EMG-preserving), no paralytic EBL / Fluids: Adjuncts: Microscope, ultrasound/fluoroscopy, multichannel lower-extremity + anal sphincter EMG, nerve stimulator Implants: Dural substitute, laminoplasty fixation Complications: None
Indications: [Age] child with spastic diplegia, good underlying strength/selective control, suitable for permanent spasticity reduction; selected by the multidisciplinary team. Risks (sensory change, bladder dysfunction, weakness) discussed.
Description of Procedure: After consent and time-out, TIVA was induced (no paralytic) and multichannel EMG including anal sphincter established. The conus was localized and a limited laminoplasty (single-level over the conus) performed; the dura was opened. Dorsal (sensory) rootlets were separated from ventral (motor) roots (confirmed by stimulation), and each dorsal root divided into rootlets. Each rootlet was stimulated and graded by its EMG response, and abnormal (sustained/spreading) rootlets selectively transected (~25–50% per level), preserving sacral (S2–4) sensory and all motor function (sphincter EMG monitored).
A watertight dural closure and laminoplasty reconstruction were performed. The child was kept flat per protocol and transferred with neuro/bladder monitoring and a planned intensive rehabilitation course.
Postoperative Plan
- Floor/PICU, flat bed rest per protocol (CSF leak/dural healing), neuro checks (motor/sensory/bladder)
- Pain/spasm management, bladder function monitoring, wound/CSF leak watch
- Intensive PT/rehab is essential (months — strengthening, gait retraining; outcomes depend heavily on rehab)
- MRI if concern; long-term: monitor for spinal deformity, functional gains
- Multidisciplinary follow-up (neurosurgery, PT, physiatry, ortho); counsel re: permanent spasticity reduction and rehab commitment
Chief-Level Case Review
Use these as the senior-level mental model for Selective Dorsal Rhizotomy (SDR):
- Decision point: The setup is age-specific: blood volume, warming, positioning pressure, airway, latex risk, family counseling, and ICU/PICU handoff differ from adults.
- Technical lever: Preserve future options: growth, shunt dependence, cranioplasty/bone healing, endocrine/neurocognitive trajectory, and adjuvant therapy influence today’s choices.
- Bailout: Have a complication script: blood loss, CSF leak, hydrocephalus, wound breakdown, posterior fossa mutism, infection, and airway/swallow risk should be anticipated.
- Postop watch: Postop communication matters: family expectations, neurologic baseline, therapy needs, school/developmental supports, and surveillance imaging/labs should be clear.
Common Pimp Questions
Use these to pressure-test preparation for Selective Dorsal Rhizotomy (SDR):
- What age-specific anatomy, blood volume, temperature, and positioning issue changes the plan?
- What is the neurologic, developmental, or syndromic baseline?
- What skin, wound, CSF, or infection risk is highest in this child?
- What family-facing expectation should be clarified before surgery?
- What postop bed, feeding, pain, imaging, and activity plan is safest?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Blood availability threshold, warming strategy, antibiotic dosing, and Foley/drain use: [attending-specific]
- Positioning aids, pinning versus horseshoe, and skin-prep preference: [attending-specific]
- Family update cadence and expected ICU/floor disposition: [attending-specific]
- Postop feeding, pain regimen, wound care, and activity restrictions: [attending-specific]