
Case Prep: Pediatric Endoscopic Third Ventriculostomy (± Choroid Plexus Cauterization)
Case / Approach Snapshot
- Anatomy at risk: age-specific skull/soft tissue, developing brain and tracts, CSF pathways, brainstem/lower cranial nerves, tumor or congenital lesion relationships, and blood-volume constraints.
- Operative steps: adapt positioning/anesthesia to age, confirm imaging and goals with family, expose gently, preserve neurovascular/CSF pathways, reconstruct durably for growth, and plan ICU/endocrine/rehab surveillance; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: blood loss, hypothermia, swelling, hydrocephalus, airway/swallowing issues, endocrine/electrolyte shifts, infection, and staged therapy with oncology or rehab teams.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age — months/years] [M/F] child with obstructive hydrocephalus due to [aqueductal stenosis / posterior fossa tumor / other] planned for endoscopic third ventriculostomy [with choroid plexus cauterization (ETV/CPC)].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Paediatric hydrocephalus — Kahle KT. Nature reviews. Disease primers 2024. PubMed
- Endoscopic third ventriculostomy versus shunt for pediatric hydrocephalus: a systematic literature review and meta-analysis — Texakalidis P. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2019. PubMed
- Endoscopic third ventriculostomy for shunt malfunction in the pediatric population: a systematic review, meta-analysis, and meta-regression analysis — Lee KS. Journal of neurosurgery. Pediatrics 2023. PubMed
- Predicting endoscopic third ventriculostomy success in pediatric shunt dysfunction: a monocentric retrospective case series of 70 consecutive children, systematic review, and meta-analysis — Guida L. Journal of neurosurgery. Pediatrics 2023. PubMed
- Endoscopic third ventriculostomy versus ventriculoperitoneal shunt in pediatric and adult population: a systematic review and meta-analysis — Pande A. Neurosurgical review 2021. PubMed
- Endoscopic third ventriculostomy versus ventriculoperitoneal shunt for treating pediatric tuberculous meningitis hydrocephalus: a systematic review and meta-analysis — Fagundes W. Journal of neurosurgery. Pediatrics 2025. PubMed
- Endoscopic third ventriculostomy for pediatric tumor-associated hydrocephalus — Sherrod BA. Neurosurgical focus 2020. PubMed
- Infant Hydrocephalus — Lu VM. Pediatrics in review 2024. PubMed
- The Global Rise of Endoscopic Third Ventriculostomy with Choroid Plexus Cauterization in Pediatric Hydrocephalus — Dewan MC. Pediatric neurosurgery 2017. PubMed
- Endoscopic third ventriculostomy in the treatment of hydrocephalus in pediatric patients — Di Rocco C. Advances and technical standards in neurosurgery 2006. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
 Figure 2. Source: Re-endoscopic third ventriculostomy versus ventriculoperitoneal shunting in failed endoscopic third ventriculostomy in pediatric patients with hydrocephalus: A systematic review — Surg Neurol Int. 2025 May 30;16:205. doi: 10.25259/SNI_1111_2024; CC BY-NC-SA.
Figure 2. Source: Re-endoscopic third ventriculostomy versus ventriculoperitoneal shunting in failed endoscopic third ventriculostomy in pediatric patients with hydrocephalus: A systematic review — Surg Neurol Int. 2025 May 30;16:205. doi: 10.25259/SNI_1111_2024; CC BY-NC-SA.
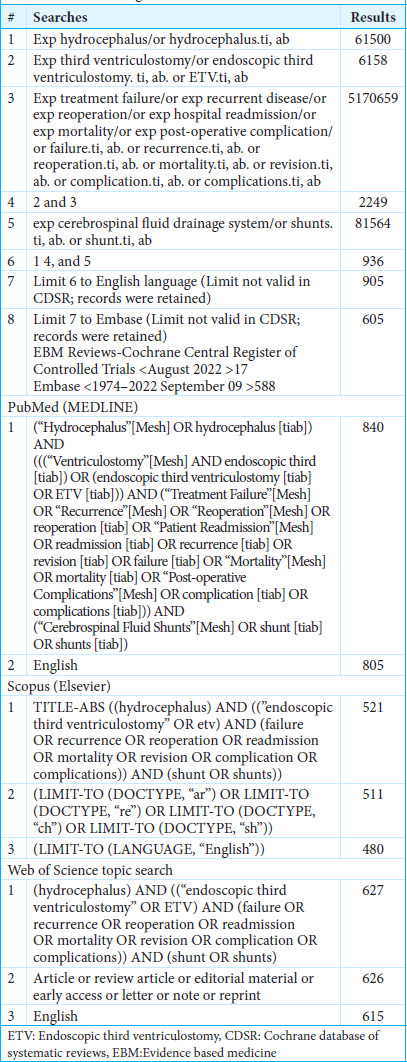 Figure 3. Source: Re-endoscopic third ventriculostomy versus ventriculoperitoneal shunting in failed endoscopic third ventriculostomy in pediatric patients with hydrocephalus: A systematic review — Surg Neurol Int. 2025 May 30;16:205. doi: 10.25259/SNI_1111_2024; CC BY-NC-SA.
Figure 3. Source: Re-endoscopic third ventriculostomy versus ventriculoperitoneal shunting in failed endoscopic third ventriculostomy in pediatric patients with hydrocephalus: A systematic review — Surg Neurol Int. 2025 May 30;16:205. doi: 10.25259/SNI_1111_2024; CC BY-NC-SA.
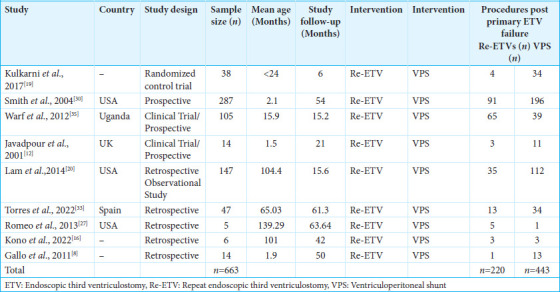 Figure 4. Source: Re-endoscopic third ventriculostomy versus ventriculoperitoneal shunting in failed endoscopic third ventriculostomy in pediatric patients with hydrocephalus: A systematic review — Surg Neurol Int. 2025 May 30;16:205. doi: 10.25259/SNI_1111_2024; CC BY-NC-SA.
Figure 4. Source: Re-endoscopic third ventriculostomy versus ventriculoperitoneal shunting in failed endoscopic third ventriculostomy in pediatric patients with hydrocephalus: A systematic review — Surg Neurol Int. 2025 May 30;16:205. doi: 10.25259/SNI_1111_2024; CC BY-NC-SA.
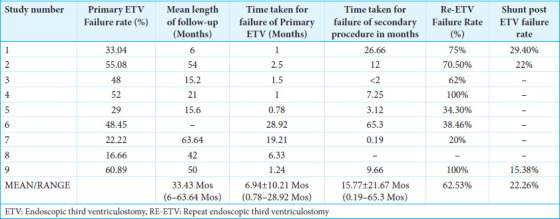 Figure 5. Source: Re-endoscopic third ventriculostomy versus ventriculoperitoneal shunting in failed endoscopic third ventriculostomy in pediatric patients with hydrocephalus: A systematic review — Surg Neurol Int. 2025 May 30;16:205. doi: 10.25259/SNI_1111_2024; CC BY-NC-SA.
Figure 5. Source: Re-endoscopic third ventriculostomy versus ventriculoperitoneal shunting in failed endoscopic third ventriculostomy in pediatric patients with hydrocephalus: A systematic review — Surg Neurol Int. 2025 May 30;16:205. doi: 10.25259/SNI_1111_2024; CC BY-NC-SA.
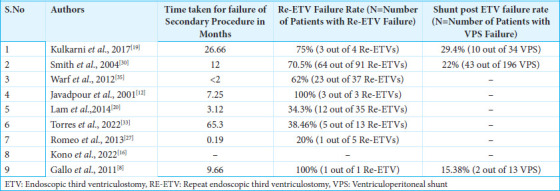 Figure 6. Source: Re-endoscopic third ventriculostomy versus ventriculoperitoneal shunting in failed endoscopic third ventriculostomy in pediatric patients with hydrocephalus: A systematic review — Surg Neurol Int. 2025 May 30;16:205. doi: 10.25259/SNI_1111_2024; CC BY-NC-SA.
Figure 6. Source: Re-endoscopic third ventriculostomy versus ventriculoperitoneal shunting in failed endoscopic third ventriculostomy in pediatric patients with hydrocephalus: A systematic review — Surg Neurol Int. 2025 May 30;16:205. doi: 10.25259/SNI_1111_2024; CC BY-NC-SA.
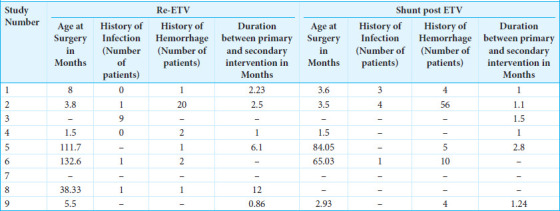 Figure 7. Source: Re-endoscopic third ventriculostomy versus ventriculoperitoneal shunting in failed endoscopic third ventriculostomy in pediatric patients with hydrocephalus: A systematic review — Surg Neurol Int. 2025 May 30;16:205. doi: 10.25259/SNI_1111_2024; CC BY-NC-SA.
Figure 7. Source: Re-endoscopic third ventriculostomy versus ventriculoperitoneal shunting in failed endoscopic third ventriculostomy in pediatric patients with hydrocephalus: A systematic review — Surg Neurol Int. 2025 May 30;16:205. doi: 10.25259/SNI_1111_2024; CC BY-NC-SA.
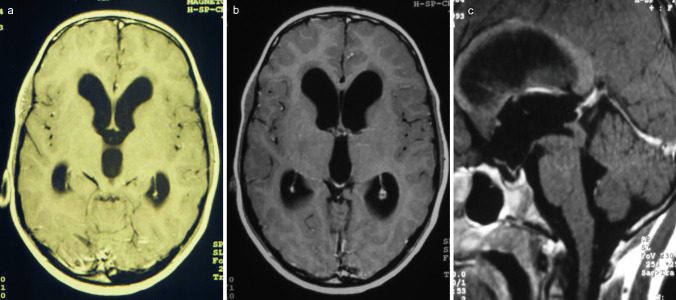 Fig. 1. Preoperative axial a, b, and sagittal c MR images showing tri-ventricular occlusive hydrocephalus due to compression of the aqueduct by a tectal lesion, suspected for low-grade tumor Source: Endoscopic transaqueductal stent placement for tumor-related aqueductal compression in pediatric patients: surgical consideration, technique, and results — Child’s Nervous System 2023; CC BY.
Fig. 1. Preoperative axial a, b, and sagittal c MR images showing tri-ventricular occlusive hydrocephalus due to compression of the aqueduct by a tectal lesion, suspected for low-grade tumor Source: Endoscopic transaqueductal stent placement for tumor-related aqueductal compression in pediatric patients: surgical consideration, technique, and results — Child’s Nervous System 2023; CC BY.
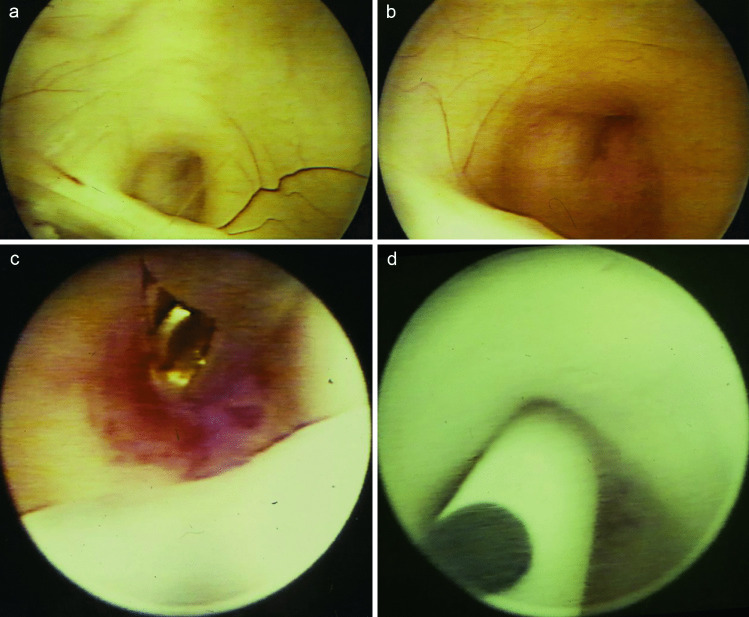 Fig. 2. Intraoperative endoscopic view on the occluded aqueduct above the posterior commissure a, b. After an endoscopic biopsy c, the transaqueductal stent is inserted via the aqueduct into the… Source: Endoscopic transaqueductal stent placement for tumor-related aqueductal compression in pediatric patients: surgical consideration, technique, and results — Child’s Nervous System 2023; CC BY.
Fig. 2. Intraoperative endoscopic view on the occluded aqueduct above the posterior commissure a, b. After an endoscopic biopsy c, the transaqueductal stent is inserted via the aqueduct into the… Source: Endoscopic transaqueductal stent placement for tumor-related aqueductal compression in pediatric patients: surgical consideration, technique, and results — Child’s Nervous System 2023; CC BY.
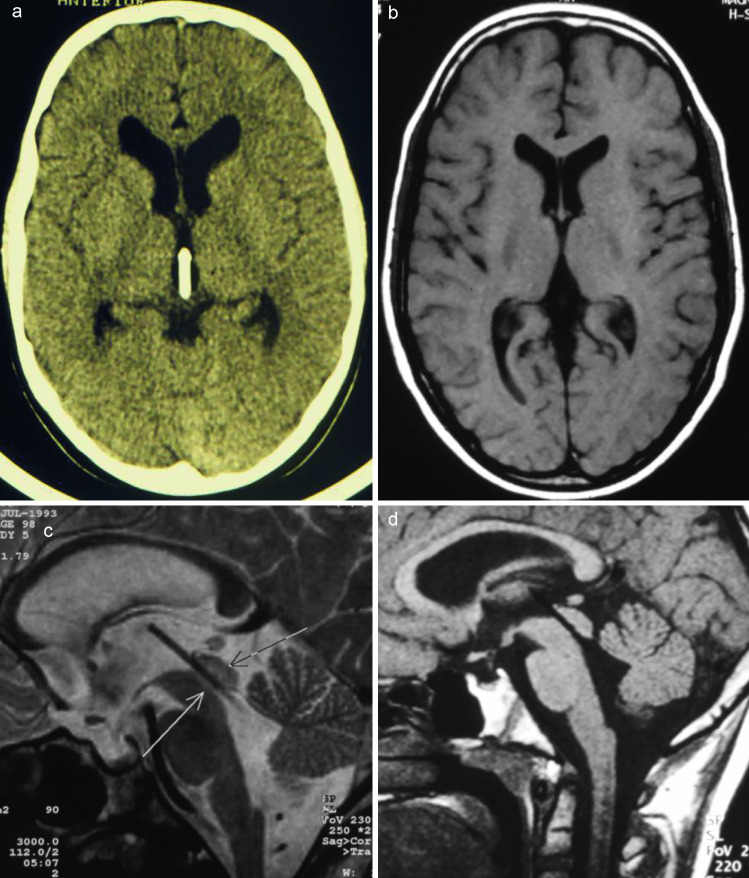 Fig. 3. Postoperative obtained axial computed tomogram a axial and sagittal MR images b, c, d showing the optimal positioning of the transaqueductal stents. Additionally, the obvious reduction… Source: Endoscopic transaqueductal stent placement for tumor-related aqueductal compression in pediatric patients: surgical consideration, technique, and results — Child’s Nervous System 2023; CC BY.
Fig. 3. Postoperative obtained axial computed tomogram a axial and sagittal MR images b, c, d showing the optimal positioning of the transaqueductal stents. Additionally, the obvious reduction… Source: Endoscopic transaqueductal stent placement for tumor-related aqueductal compression in pediatric patients: surgical consideration, technique, and results — Child’s Nervous System 2023; CC BY.
History of Present Illness
- Chief complaint: Macrocephaly, bulging fontanelle, sunsetting eyes, irritability, vomiting, developmental delay (infants); headache/vomiting (older)
- Etiology: aqueductal stenosis, tumor (tectal/pineal/posterior fossa), post-hemorrhagic, post-infectious
- ETV Success Score (age, etiology, prior shunt) — younger infants and post-infectious have lower success; ETV+CPC improves success in infants (Warf technique, esp. < 1-2 years)
Past Medical History
- Prematurity, IVH (post-hemorrhagic hydrocephalus), prior infection (post-infectious), prior shunt
- Birth/developmental history
Imaging Review
MRI (sagittal, T2, CISS, cine flow)
- Triventricular hydrocephalus (obstructive pattern), aqueduct (stenosis/tumor)
- Third ventricle floor — thinned, bowed; prepontine cistern space (adequate between floor and basilar/clivus)
- Basilar artery position, anatomy (massa intermedia, infundibular recess, mammillary bodies)
- Etiology (tumor, septations)
Labs
- CBC, BMP, Coags, pediatric pre-op
Examination
- Head circumference (plot), fontanelle, eye movements (sunsetting, CN VI), developmental status
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: pediatric anesthesia/equipment, warming, weight-based implants/antibiotics, navigation/endoscope/microscope as needed, blood availability for tumor/myelomeningocele cases, and family-centered postop handoff.
- Special needs: weight-based fluids/meds, latex allergy precautions for myelomeningocele, steroid/endocrine/DI plan when sellar/posterior fossa risk exists, EVD/CSF diversion plan, and age-appropriate neuro baseline.
- Immediate postop orders: PICU/step-down neuro checks, airway/swallow monitoring when relevant, CT/MRI timing, drain/EVD/shunt orders, antibiotics/steroid taper, pain control, wound/skin precautions, and PT/OT/rehab planning.
Diagnosis & Indication
- Indication: Obstructive hydrocephalus; ETV avoids shunt dependence; ETV+CPC for infants to improve success (cauterize choroid plexus to reduce CSF production)
- Cautions: very young infants (lower ETV success alone → add CPC), prepontine scarring (post-infectious), narrow cistern, distorted anatomy
ETV Success Read
- Favor ETV when hydrocephalus is obstructive with a defined block (aqueductal stenosis, tectal/pineal/posterior fossa obstruction) and a navigable third-ventricle floor/prepontine cistern.
- Lower success is expected in very young infants, postinfectious/posthemorrhagic hydrocephalus, thick opaque floor, scarred prepontine cistern, small ventricles, or prior failed ETV with closed/scarred stoma.
- ETV+CPC is most relevant in infants and selected shunt-avoidance scenarios; the added value depends on age, etiology, anatomy, and ability to safely reach/cauterize the plexus.
- A shunt is still the safer answer when the anatomy is hostile, the floor landmarks are not trustworthy, or the child cannot tolerate an uncertain ETV failure risk.
Imaging Checklist
- MRI sagittal CISS/FIESTA or equivalent: third-ventricle floor thickness, basilar position, clival/dorsum relationship, prepontine cistern size, Liliequist membrane, and any interpeduncular scarring.
- Coronal/axial planning: foramen of Monro size, venous anatomy, septations, mass trajectory constraints, and whether a flexible scope is needed for CPC.
- Review prior shunt history, infection/hemorrhage, and whether ventricles are large enough for safe endoscopic working room.
Position
- Supine, head neutral/slightly flexed, age-appropriate fixation/padding
- Right frontal entry (modified Kocher trajectory to foramen of Monro)
Key Surgical Steps
- Right frontal burr hole (or fontanelle-based in infants), trajectory to foramen of Monro
- Introduce rigid (or flexible) neuroendoscope via peel-away sheath into the lateral ventricle
- Identify foramen of Monro landmarks (choroid plexus, septal/thalamostriate veins, fornix)
- Enter third ventricle; identify floor landmarks — mammillary bodies (posterior), infundibular recess (anterior), tuber cinereum (between)
- Fenestrate the floor in the midline anterior to the mammillary bodies, behind the dorsum sellae (through tuber cinereum) — blunt perforation (not cautery near basilar), dilate with Fogarty balloon
- Open the membrane of Liliequist; confirm patency into the prepontine cistern; visualize and avoid the basilar artery and perforators
- ETV+CPC (if performed): with flexible scope, cauterize the choroid plexus bilaterally in the lateral ventricles (and septostomy as needed)
- Confirm flow (floor pulsation), hemostasis, withdraw scope, closure
Critical Anatomy & Structures at Risk
- Basilar artery and perforators — directly below the floor; injury catastrophic
- Fornix (foramen of Monro) — memory
- Hypothalamus (floor) — endocrine/autonomic
- Choroid plexus vessels (CPC — bleeding), septal/thalamostriate veins
Equipment
- Rigid neuroendoscope (ETV) ± flexible scope (for CPC), working channel
- Fogarty/ETV balloon, blunt fenestration probe, bipolar/cautery (CPC)
- Warm irrigation (LR), EVD kit (backup), pediatric setup
Monitoring
- Standard; watch bradycardia (floor manipulation)
Anesthesia
- Pediatric general; warm irrigation (thermoregulation), watch bradycardia/asystole during floor manipulation (stop, irrigate), careful fluid balance
Potential Complications
- Basilar artery injury (rare, catastrophic), bradycardia/arrest (floor)
- Fornix/hypothalamic injury, CN III palsy
- ETV failure (esp. infants/post-infectious) → may need repeat or shunt; delayed closure possible (counsel re: warning signs)
- CSF leak, intraventricular hemorrhage (CPC), infection
Rescue and Failure Logic
- Bradycardia/asystole during floor work: stop manipulation, irrigate warm fluid, let anesthesia restore hemodynamics, and resume only if landmarks remain clear and the child is stable.
- Basilar/perforator seen too close or floor opaque: do not force the stoma; adjust trajectory only if safe, otherwise abort to shunt/alternate diversion.
- Bleeding during CPC: irrigate patiently, lower irrigation pressure once visibility returns, use focal bipolar only on plexus, and avoid chasing blood into the foramen/veins.
- No visible prepontine flow after fenestration: open Liliequist membrane, inspect for a second membrane, confirm the basilar/perforator corridor, and consider leaving an EVD or converting if patency remains doubtful.
- Early clinical failure: do not rely on ventricular size alone; evaluate symptoms, fontanelle/OFC, wound, infection, cine flow when useful, and have a low threshold for shunt in an unstable infant.
- Late failure: treat recurrent headache/vomiting/lethargy/sunsetting as urgent hydrocephalus until proven otherwise, even years after a successful ETV.
Operative Note Template
Preoperative Diagnosis: Obstructive hydrocephalus ([aqueductal stenosis / tumor / post-hemorrhagic])
Postoperative Diagnosis: Same
Procedure: Endoscopic third ventriculostomy [with choroid plexus cauterization (ETV/CPC)]
Surgeon / Assistant: Anesthesia: Pediatric general endotracheal EBL / Fluids: Minimal Adjuncts: Rigid [± flexible] neuroendoscope, Fogarty/ETV balloon, [bipolar for CPC], warm irrigation Complications: None Note: Watch for bradycardia during floor manipulation
Indications: [Age — months/years] child with obstructive hydrocephalus and favorable floor anatomy; [ETV+CPC chosen to improve success in the infant]. Risks (basilar injury, bradycardia, ETV failure) discussed with family.
Description of Procedure: After consent and time-out, pediatric general anesthesia was induced (warm irrigation). A right frontal entry was made along a trajectory to the foramen of Monro and the endoscope introduced. The foramen of Monro landmarks were identified and the third ventricle entered; the floor landmarks (mammillary bodies, infundibular recess, tuber cinereum) were defined. The floor was bluntly fenestrated in the midline anterior to the mammillary bodies and dilated with a Fogarty balloon, the membrane of Liliequist opened, and patency confirmed with the basilar artery visualized and avoided. [With a flexible scope, the choroid plexus was cauterized bilaterally (CPC).] Floor pulsation confirmed flow.
The endoscope was withdrawn and closure performed. The infant/child was transferred with head-circumference/fontanelle monitoring and family education on ETV-failure signs.
Postoperative Plan
- Floor/PICU per age, neuro checks, head circumference/fontanelle
- CT/MRI postop (ventricles may not shrink immediately; cine flow shows stoma patency)
- Monitor for ETV failure (recurrent hydrocephalus — bulging fontanelle, increasing OFC, vomiting, sunsetting — can be early or delayed → shunt)
- Educate family on warning signs of failure
- Follow-up MRI, developmental surveillance, neurosurgery follow-up
Chief-Level Case Review
Use these as the senior-level mental model for Pediatric Endoscopic Third Ventriculostomy (± Choroid Plexus Cauterization):
- Decision point: The setup is age-specific: blood volume, warming, positioning pressure, airway, latex risk, family counseling, and ICU/PICU handoff differ from adults.
- Technical lever: Preserve future options: growth, shunt dependence, cranioplasty/bone healing, endocrine/neurocognitive trajectory, and adjuvant therapy influence today’s choices.
- Bailout: Have a complication script: blood loss, CSF leak, hydrocephalus, wound breakdown, posterior fossa mutism, infection, and airway/swallow risk should be anticipated.
- Postop watch: Postop communication matters: family expectations, neurologic baseline, therapy needs, school/developmental supports, and surveillance imaging/labs should be clear.
Common Pimp Questions
Use these to pressure-test preparation for Pediatric Endoscopic Third Ventriculostomy (± Choroid Plexus Cauterization):
- What age-specific anatomy, blood volume, temperature, and positioning issue changes the plan?
- What is the neurologic, developmental, or syndromic baseline?
- What skin, wound, CSF, or infection risk is highest in this child?
- What family-facing expectation should be clarified before surgery?
- What postop bed, feeding, pain, imaging, and activity plan is safest?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Blood availability threshold, warming strategy, antibiotic dosing, and Foley/drain use: [attending-specific]
- Positioning aids, pinning versus horseshoe, and skin-prep preference: [attending-specific]
- Family update cadence and expected ICU/floor disposition: [attending-specific]
- Postop feeding, pain regimen, wound care, and activity restrictions: [attending-specific]