
Case Prep: Myelomeningocele Repair (Open Neural Tube Defect Closure)
Case / Approach Snapshot
- Anatomy at risk: age-specific skull/soft tissue, developing brain and tracts, CSF pathways, brainstem/lower cranial nerves, tumor or congenital lesion relationships, and blood-volume constraints.
- Operative steps: adapt positioning/anesthesia to age, confirm imaging and goals with family, expose gently, preserve neurovascular/CSF pathways, reconstruct durably for growth, and plan ICU/endocrine/rehab surveillance; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: blood loss, hypothermia, swelling, hydrocephalus, airway/swallowing issues, endocrine/electrolyte shifts, infection, and staged therapy with oncology or rehab teams.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Newborn / __ -day-old] [M/F] neonate with a [lumbar/lumbosacral/thoracic] myelomeningocele planned for [postnatal] microsurgical repair and multilayer closure [within 48-72 hours of birth] [or note prior fetal repair].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Myelomeningocele — Karsonovich T. 2026. PubMed
- Update on prenatal diagnosis and fetal surgery for myelomeningocele — Meller C. Archivos argentinos de pediatria 2021. PubMed
- The Management of Myelomeningocele Study: full cohort 30-month pediatric outcomes — Farmer DL. American journal of obstetrics and gynecology 2018. PubMed
- Fetal myelomeningocele repair — Yamashiro KJ. Seminars in pediatric surgery 2019. PubMed
- Open myelomeningocele — Hahn YS. Neurosurgery clinics of North America 1995. PubMed
- Myelomeningocele closure: A review and decision-making guidance — Ghadban E. JPRAS open 2025. PubMed
- Reflections upon the intrauterine repair of myelomeningocele — Talamonti G. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2024. PubMed
- Myelomeningocele with Associated Anomalies – Case Report and Literature Review — Kitov B. Folia medica 2019. PubMed
- Fetal myelomeningocele repair: a narrative review of the history, current controversies and future directions — Yamashiro KJ. Translational pediatrics 2021. PubMed
- Hydrocephalus in myelomeningocele — Cavalheiro S. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2021. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
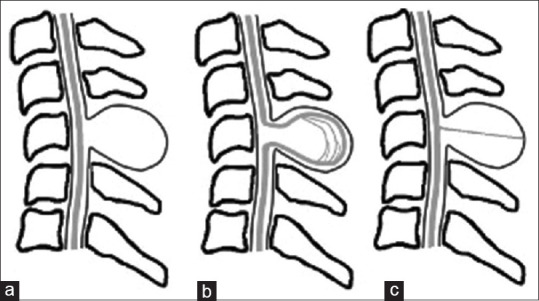 Figure 1. Classification of cervical myelomeningocele and meningocele. (a) Fibrovascular or neuroglial tissue protruding from the posterior surface of the spinal cord attached to the sac wall. (b)… Source: Prenatal Diagnosis and Outcomes of Cervical Meningocele and Myelomeningocele — Journal of Medical Ultrasound 2024; CC BY-NC-SA.
Figure 1. Classification of cervical myelomeningocele and meningocele. (a) Fibrovascular or neuroglial tissue protruding from the posterior surface of the spinal cord attached to the sac wall. (b)… Source: Prenatal Diagnosis and Outcomes of Cervical Meningocele and Myelomeningocele — Journal of Medical Ultrasound 2024; CC BY-NC-SA.
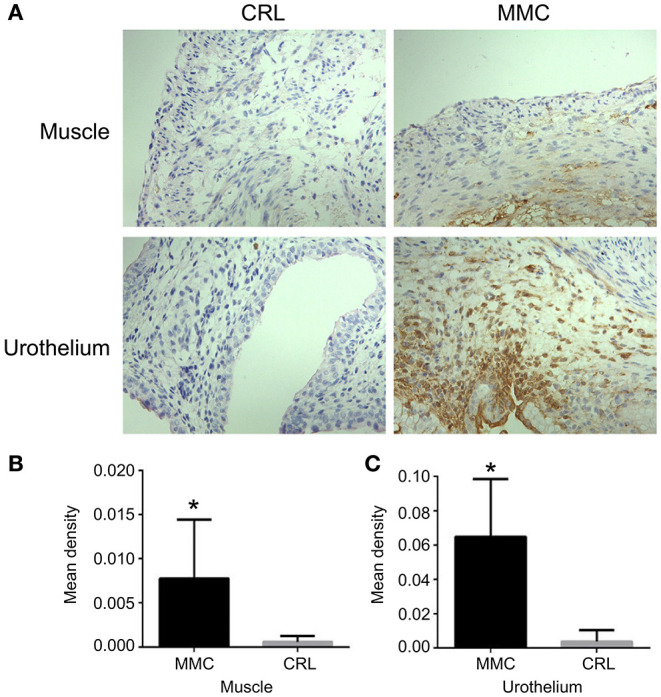 Figure 3. Expression and distribution of bladder cleaved caspase-3 at E22. (A) The distribution of cleaved caspase-3 at E22. (B) The expression of cleaved caspase-3 in the bladder muscle layer was… Source: The Mechanism of Bladder Injury in Fetal Rats With Myelomeningocele — Frontiers in Neurology 2022; CC BY.
Figure 3. Expression and distribution of bladder cleaved caspase-3 at E22. (A) The distribution of cleaved caspase-3 at E22. (B) The expression of cleaved caspase-3 in the bladder muscle layer was… Source: The Mechanism of Bladder Injury in Fetal Rats With Myelomeningocele — Frontiers in Neurology 2022; CC BY.
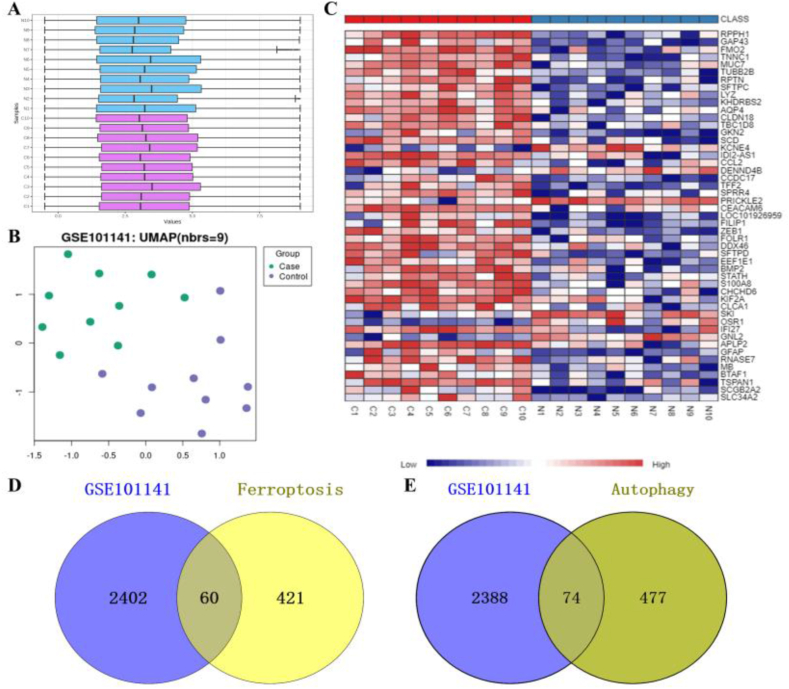 Fig. 1. Identification of DEGs in the GSE101141 GEO dataset. A Normalization of the GSE101141 dataset was performed using Log2 transformation: N, Control; C, myelomeningocele; B UMAP plot; C… Source: Identification of potential key ferroptosis- and autophagy-related genes in myelomeningocele through bioinformatics analysis — Heliyon 2024; CC BY-NC.
Fig. 1. Identification of DEGs in the GSE101141 GEO dataset. A Normalization of the GSE101141 dataset was performed using Log2 transformation: N, Control; C, myelomeningocele; B UMAP plot; C… Source: Identification of potential key ferroptosis- and autophagy-related genes in myelomeningocele through bioinformatics analysis — Heliyon 2024; CC BY-NC.
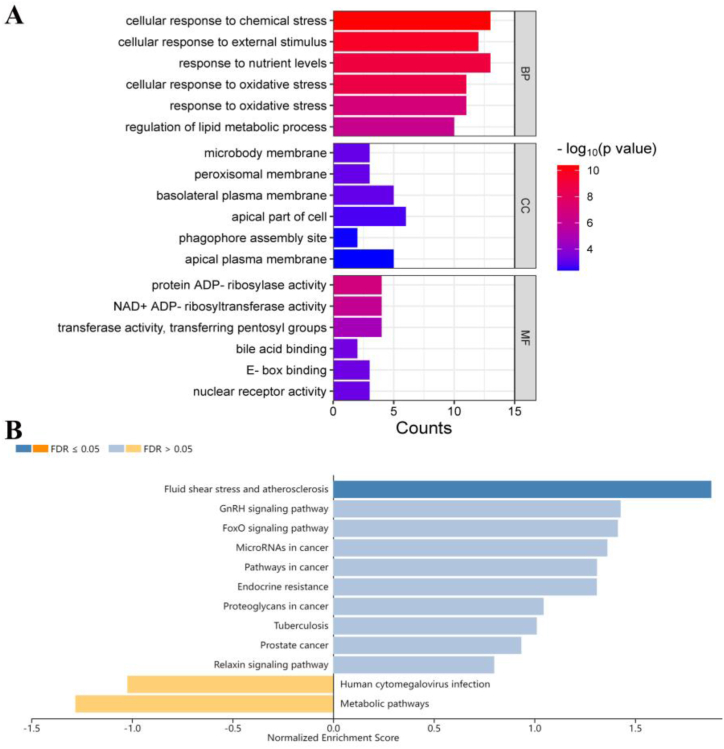 Fig. 2. Functional enrichment analysis of ferroptosis-related DEGs. A GO enrichment analysis of ferroptosis-related DEGs using SRplot: BP, biological process; CC, cellular component; MF,… Source: Identification of potential key ferroptosis- and autophagy-related genes in myelomeningocele through bioinformatics analysis — Heliyon 2024; CC BY-NC.
Fig. 2. Functional enrichment analysis of ferroptosis-related DEGs. A GO enrichment analysis of ferroptosis-related DEGs using SRplot: BP, biological process; CC, cellular component; MF,… Source: Identification of potential key ferroptosis- and autophagy-related genes in myelomeningocele through bioinformatics analysis — Heliyon 2024; CC BY-NC.
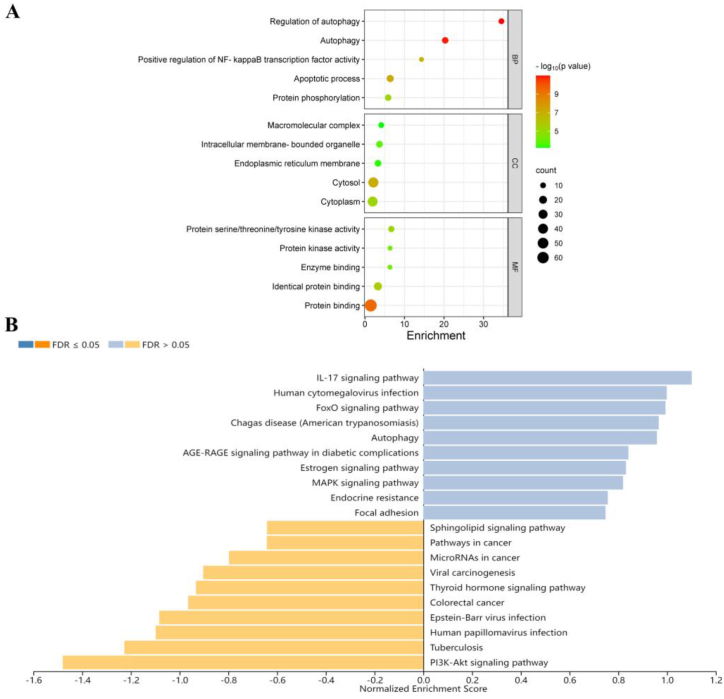 Fig. 3. Functional enrichment analysis of autophagy-related DEGs. A GO enrichment analysis of autophagy-related DEGs using DAVID and SRplot: BP, biological process; CC, cellular component; MF,… Source: Identification of potential key ferroptosis- and autophagy-related genes in myelomeningocele through bioinformatics analysis — Heliyon 2024; CC BY-NC.
Fig. 3. Functional enrichment analysis of autophagy-related DEGs. A GO enrichment analysis of autophagy-related DEGs using DAVID and SRplot: BP, biological process; CC, cellular component; MF,… Source: Identification of potential key ferroptosis- and autophagy-related genes in myelomeningocele through bioinformatics analysis — Heliyon 2024; CC BY-NC.
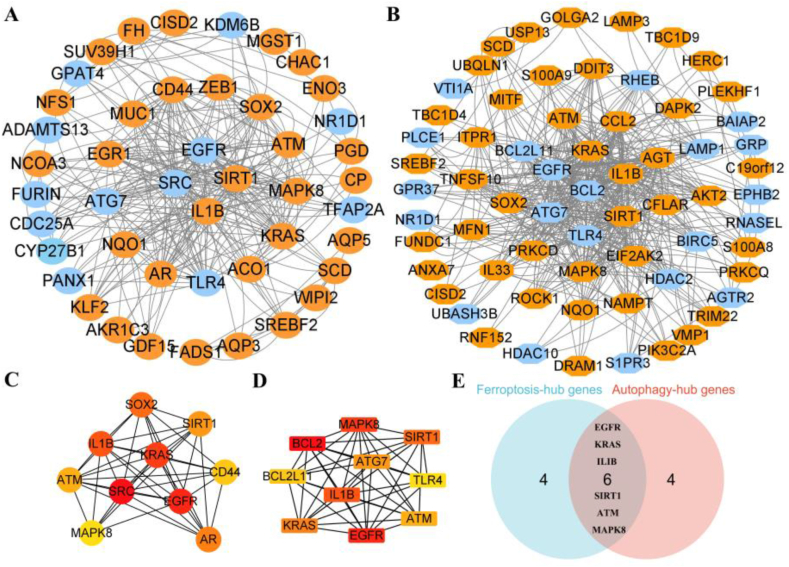 Fig. 4. PPI analysis of ferroptosis- and autophagy-related DEGs. A and B PPI analysis of ferroptosis- and autophagy-related DEGs: orange, upregulated genes; blue, downregulated genes; C and D… Source: Identification of potential key ferroptosis- and autophagy-related genes in myelomeningocele through bioinformatics analysis — Heliyon 2024; CC BY-NC.
Fig. 4. PPI analysis of ferroptosis- and autophagy-related DEGs. A and B PPI analysis of ferroptosis- and autophagy-related DEGs: orange, upregulated genes; blue, downregulated genes; C and D… Source: Identification of potential key ferroptosis- and autophagy-related genes in myelomeningocele through bioinformatics analysis — Heliyon 2024; CC BY-NC.
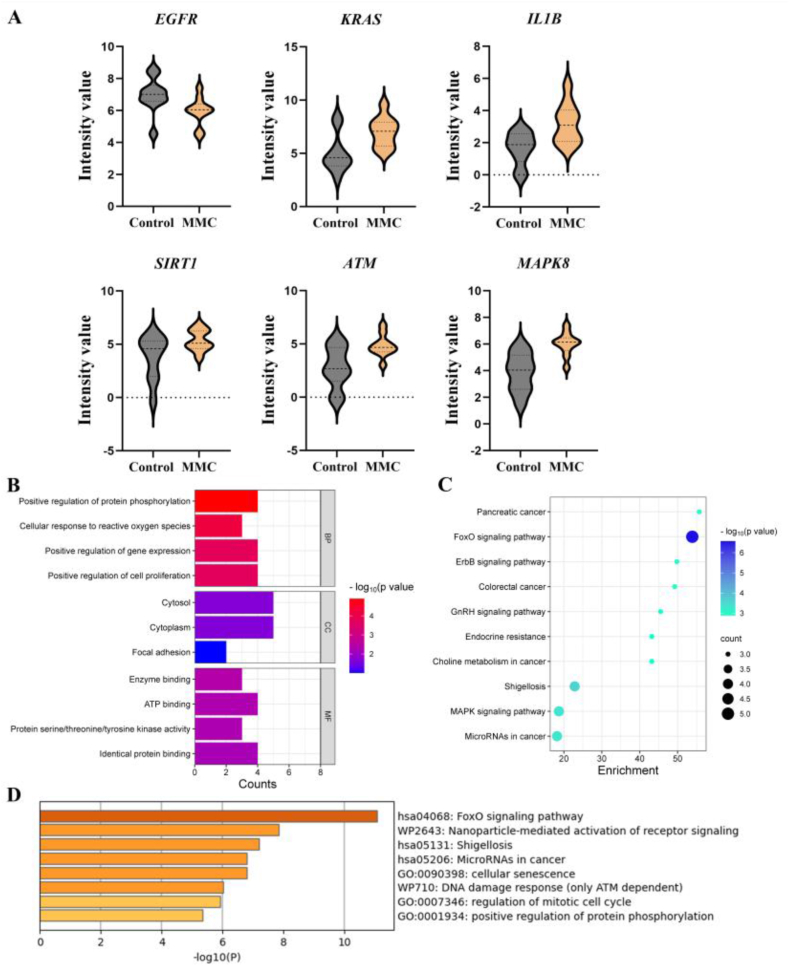 Fig. 5. Expression and function enrichment of candidate genes. A Expression of candidate genes from GSE101141; B and C GO and KEGG enrichment analyses of candidate genes using DAVID and SRplot:… Source: Identification of potential key ferroptosis- and autophagy-related genes in myelomeningocele through bioinformatics analysis — Heliyon 2024; CC BY-NC.
Fig. 5. Expression and function enrichment of candidate genes. A Expression of candidate genes from GSE101141; B and C GO and KEGG enrichment analyses of candidate genes using DAVID and SRplot:… Source: Identification of potential key ferroptosis- and autophagy-related genes in myelomeningocele through bioinformatics analysis — Heliyon 2024; CC BY-NC.
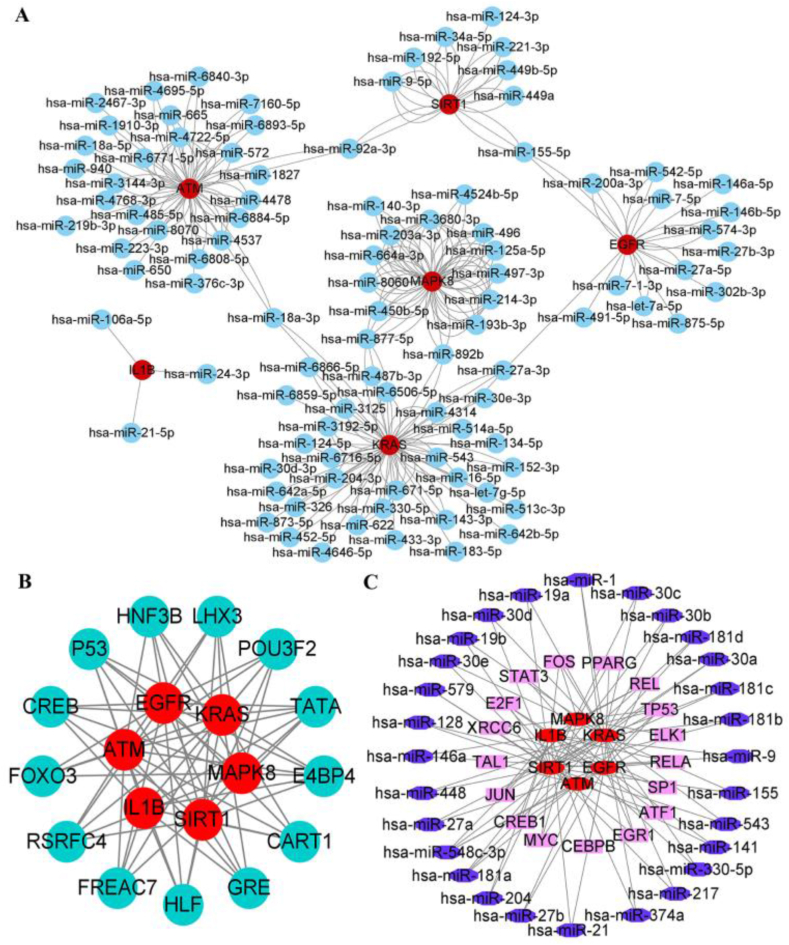 Fig. 6. Interaction network among miRNAs, TFs, and candidate genes. A Interaction network between candidate genes and targeted miRNAs: red, candidate genes; blue, miRNA; B Interaction network of… Source: Identification of potential key ferroptosis- and autophagy-related genes in myelomeningocele through bioinformatics analysis — Heliyon 2024; CC BY-NC.
Fig. 6. Interaction network among miRNAs, TFs, and candidate genes. A Interaction network between candidate genes and targeted miRNAs: red, candidate genes; blue, miRNA; B Interaction network of… Source: Identification of potential key ferroptosis- and autophagy-related genes in myelomeningocele through bioinformatics analysis — Heliyon 2024; CC BY-NC.
History of Present Illness
- Open neural tube defect identified [prenatally on ultrasound/MRI and elevated maternal AFP / at birth]
- Fetal repair (MOMS trial — in utero closure reduces hydrocephalus/shunt rate and improves motor outcomes) vs postnatal repair
- Level of lesion (predicts motor/functional outcome), leaking CSF, neurological function of legs, anal tone
- Associated: Chiari II malformation, hydrocephalus, clubfoot, neurogenic bladder
Past Medical History / Birth
- Prenatal course, mode of delivery (C-section to protect placode)
- Maternal folate, gestational age, other anomalies
- Latex precautions from birth (high latex allergy risk in spina bifida)
Imaging Review
MRI brain and spine
- Chiari II (hindbrain herniation), hydrocephalus, ventricular size, the neural placode, level, associated cord anomalies (syrinx, diastematomyelia)
Head ultrasound
- Ventricular size (hydrocephalus — many need shunt/ETV, often staged after closure)
Labs
- CBC, BMP, type and screen (neonatal), coagulation
- Strict latex-free environment
Neurological Examination
- Spontaneous leg movement, response to stimulation (motor level), anal wink/tone, reflexes, head circumference, fontanelle, document baseline
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: pediatric anesthesia/equipment, warming, weight-based implants/antibiotics, navigation/endoscope/microscope as needed, blood availability for tumor/myelomeningocele cases, and family-centered postop handoff.
- Special needs: weight-based fluids/meds, latex allergy precautions for myelomeningocele, steroid/endocrine/DI plan when sellar/posterior fossa risk exists, EVD/CSF diversion plan, and age-appropriate neuro baseline.
- Immediate postop orders: PICU/step-down neuro checks, airway/swallow monitoring when relevant, CT/MRI timing, drain/EVD/shunt orders, antibiotics/steroid taper, pain control, wound/skin precautions, and PT/OT/rehab planning.
Goals & Timing
- Goals: Reconstitute the neural tube (untether/reposition placode into the canal), achieve watertight dural closure, multilayer soft tissue coverage to prevent CSF leak/infection/meningitis and preserve function
- Timing: within 48-72 hours of birth (reduces infection/ventriculitis) if not repaired in utero
Position
- Prone, neonatal padding/thermoregulation (warmer, careful), rolls, protect the exposed placode (keep moist, sterile, no pressure preop), latex-free
Key Surgical Steps
- Examine the defect: central neural placode, surrounding arachnoid/dura, then epithelialized skin junction
- Dissect the placode free circumferentially at the junction of neural tissue and the surrounding membrane/skin (the zona epitheliosa) — release tethering, excise non-neural epithelial tissue (prevents inclusion dermoid)
- Reconstitute the placode — “neurulate” by approximating the pia/placode edges into a tube (pial reapproximation) to reduce retethering
- Place the neural tube back into the spinal canal
- Dural closure — dissect dura from surrounding fascia, close in a watertight layer over the placode
- Fascial/myofascial layer — mobilize paraspinal fascia, close as additional watertight layer
- Skin closure — undermine skin, close (may need relaxing incisions or plastics flaps for large defects)
- Avoid tight closure/tension; ensure no CSF leak
Critical Anatomy & Structures at Risk
- Neural placode / functional neural tissue — preserve all functional tissue (handle gently, stimulate to identify)
- Nerve roots from the placode
- Watertight dura (CSF leak/meningitis), skin viability (large defects)
- Avoid leaving epithelial elements (dermoid/retethering)
Equipment
- Microscope, microsurgical/neonatal instruments, fine bipolar
- Nerve stimulator, dural substitute (if needed), fine suture
- Latex-free everything, neonatal warming, plastics backup (large defects)
Monitoring
- Neonatal anesthesia monitoring; optional EMG
Anesthesia
- Neonatal general anesthesia, thermoregulation, latex-free, careful fluid/glucose, prone neonatal precautions
Potential Complications
- CSF leak / wound breakdown / meningitis (closure integrity)
- Hydrocephalus (progressive — many need shunt/ETV after closure; monitor head circumference/ventricles)
- Symptomatic Chiari II (stridor, apnea, swallowing — may need decompression)
- Retethering (later), skin necrosis, infection
- Neurological function fixed by lesion level (closure preserves, rarely improves)
Operative Note Template
Preoperative Diagnosis: [Lumbosacral] myelomeningocele (open neural tube defect)
Postoperative Diagnosis: Same
Procedure: Microsurgical repair of [lumbosacral] myelomeningocele with neurulation and multilayer (dural, fascial, skin) closure
Surgeon / Assistant: Anesthesia: Neonatal general endotracheal, latex-free, thermoregulation EBL / Fluids: Adjuncts: Microscope, nerve stimulator, [plastics for large defects] Implants: [Dural substitute if needed] Complications: None
Indications: Newborn with a [lumbosacral] myelomeningocele [not repaired in utero], repaired within 48–72h to prevent infection/ventriculitis and preserve function. Latex precautions from birth. Risks (CSF leak, hydrocephalus, Chiari II) discussed with family.
Description of Procedure: After consent and time-out, neonatal general anesthesia was induced (latex-free, warming) and the infant positioned prone with the placode protected. Under the microscope, the neural placode was dissected circumferentially free at the junction with the surrounding membrane/skin (zona epitheliosa), and non-neural epithelial tissue excised (to prevent inclusion dermoid). The placode was reconstituted by pial reapproximation (neurulation) and returned into the spinal canal.
The dura was dissected and closed in a watertight layer, followed by a myofascial layer, and the skin closed [with relaxing incisions/flaps for the large defect], avoiding tension. No CSF leak was evident.
The infant was transferred to the NICU prone/side-lying with serial head-circumference/US monitoring (hydrocephalus) and a multidisciplinary spina bifida plan.
Postoperative Plan
- NICU, prone/side-lying positioning (protect closure, off the back)
- Monitor wound for CSF leak/breakdown, serial head circumference and head US (hydrocephalus)
- Watch for Chiari II symptoms (stridor, apnea, feeding) — may need urgent intervention
- Latex-free, neurogenic bladder management (urology — CIC), orthopedics (feet/hips), multidisciplinary spina bifida team
- Plan for CSF diversion (VP shunt/ETV) if hydrocephalus progresses (often ~1-2 weeks)
- Long-term: tethered cord surveillance, developmental follow-up
Chief-Level Case Review
Use these as the senior-level mental model for Myelomeningocele Repair (Open Neural Tube Defect Closure):
- Decision point: The setup is age-specific: blood volume, warming, positioning pressure, airway, latex risk, family counseling, and ICU/PICU handoff differ from adults.
- Technical lever: Preserve future options: growth, shunt dependence, cranioplasty/bone healing, endocrine/neurocognitive trajectory, and adjuvant therapy influence today’s choices.
- Bailout: Have a complication script: blood loss, CSF leak, hydrocephalus, wound breakdown, posterior fossa mutism, infection, and airway/swallow risk should be anticipated.
- Postop watch: Postop communication matters: family expectations, neurologic baseline, therapy needs, school/developmental supports, and surveillance imaging/labs should be clear.
Common Pimp Questions
Use these to pressure-test preparation for Myelomeningocele Repair (Open Neural Tube Defect Closure):
- What age-specific anatomy, blood volume, temperature, and positioning issue changes the plan?
- What is the neurologic, developmental, or syndromic baseline?
- What skin, wound, CSF, or infection risk is highest in this child?
- What family-facing expectation should be clarified before surgery?
- What postop bed, feeding, pain, imaging, and activity plan is safest?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Blood availability threshold, warming strategy, antibiotic dosing, and Foley/drain use: [attending-specific]
- Positioning aids, pinning versus horseshoe, and skin-prep preference: [attending-specific]
- Family update cadence and expected ICU/floor disposition: [attending-specific]
- Postop feeding, pain regimen, wound care, and activity restrictions: [attending-specific]