
Case Prep: Encephalocele Repair
Case / Approach Snapshot
- Anatomy at risk: age-specific skull/soft tissue, developing brain and tracts, CSF pathways, brainstem/lower cranial nerves, tumor or congenital lesion relationships, and blood-volume constraints.
- Operative steps: adapt positioning/anesthesia to age, confirm imaging and goals with family, expose gently, preserve neurovascular/CSF pathways, reconstruct durably for growth, and plan ICU/endocrine/rehab surveillance; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: blood loss, hypothermia, swelling, hydrocephalus, airway/swallowing issues, endocrine/electrolyte shifts, infection, and staged therapy with oncology or rehab teams.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age — newborn/infant] [M/F] with a [occipital / frontoethmoidal (sincipital) / basal / parietal] encephalocele planned for microsurgical repair and multilayer closure [± skull base reconstruction].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Posterior Encephalocele — Society for Maternal-Fetal Medicine. American journal of obstetrics and gynecology 2020. PubMed
- Frontoethmoidal encephalocele. Report of a case — Horcajadas A. Neurocirugia 2019. PubMed
- Occipital Encephalocele: Cause, Incidence, Neuroimaging and Surgical Management — Markovic I. Current pediatric reviews 2020. PubMed
- Occipital encephalocele associated with Dandy-Walker malformation: a case-based review — Gutierrez F. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2022. PubMed
- Hydrocephalus in encephalocele — Akyol ME. European review for medical and pharmacological sciences 2022. PubMed
- Quadrigeminal arachnoid cyst with perinatal encephalocele — Akutagawa K. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2020. PubMed
- Anterior encephalocele — Rapport RL 2nd. Journal of neurosurgery 1981. PubMed
- Encephalocele — Jowi JO. East African medical journal 2009. PubMed
- ENCEPHALOCELE — ACERS TE. Archives of ophthalmology (Chicago, Ill. : 1960) 1965. PubMed
- [Frontoethmoidal encephalocele] — Parada Vásquez RH. Medicina clinica 2016. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
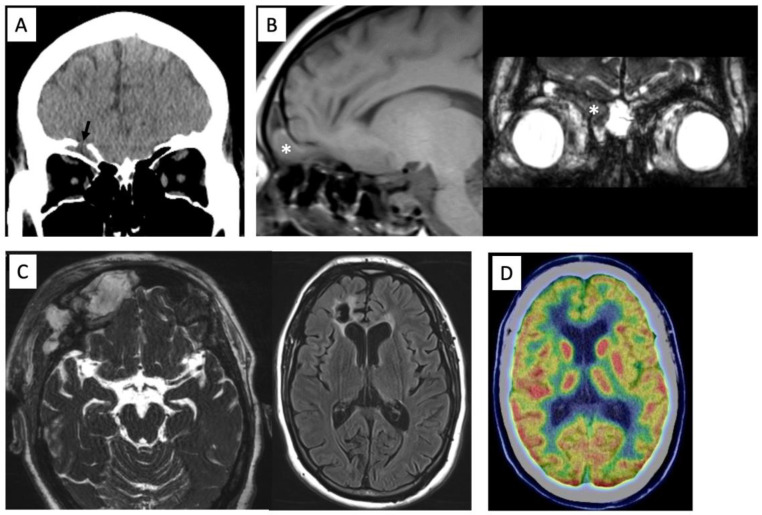 Figure 1. Preoperative computed tomography showing the anterior skull base defect (arrow) (A). MR images showing a prolapsed right rectal gyrus into the frontal sinus on T1-weighted image and… Source: Frontal Encephalocele Plus Epilepsy: A Case Report and Review of the Literature — Brain Sciences 2023; CC BY.
Figure 1. Preoperative computed tomography showing the anterior skull base defect (arrow) (A). MR images showing a prolapsed right rectal gyrus into the frontal sinus on T1-weighted image and… Source: Frontal Encephalocele Plus Epilepsy: A Case Report and Review of the Literature — Brain Sciences 2023; CC BY.
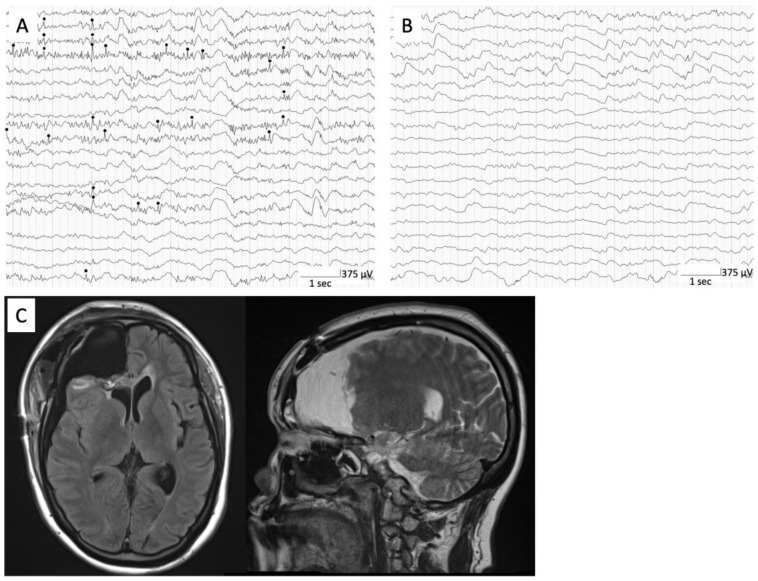 Figure 2. Intraoperative ECoG showing interictal epileptiform discharges (black circle) at right frontal lateral cortex (A). Postoperative intraoperative ECoG showing no obvious interictal… Source: Frontal Encephalocele Plus Epilepsy: A Case Report and Review of the Literature — Brain Sciences 2023; CC BY.
Figure 2. Intraoperative ECoG showing interictal epileptiform discharges (black circle) at right frontal lateral cortex (A). Postoperative intraoperative ECoG showing no obvious interictal… Source: Frontal Encephalocele Plus Epilepsy: A Case Report and Review of the Literature — Brain Sciences 2023; CC BY.
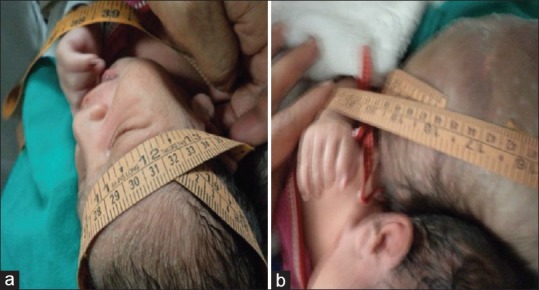 Figure 1. (a) The occipito-frontal circumference was 31 cm and (b) encephalocele circumference was 45 cm Source: A giant occipital encephalocele with spontaneous hemorrhage into the sac: A rare case report — Asian Journal of Neurosurgery 2014; CC BY-NC-SA.
Figure 1. (a) The occipito-frontal circumference was 31 cm and (b) encephalocele circumference was 45 cm Source: A giant occipital encephalocele with spontaneous hemorrhage into the sac: A rare case report — Asian Journal of Neurosurgery 2014; CC BY-NC-SA.
History of Present Illness
- Chief complaint: Congenital midline skull defect with herniation of [meninges (meningocele) / brain + meninges (encephalocele/meningoencephalocele)]
- Location:
- Occipital (most common in Western populations) — posterior, may contain brain/venous sinuses
- Frontoethmoidal/sincipital (common in SE Asia) — nasofrontal/nasoethmoidal/naso-orbital, facial deformity
- Basal (transethmoidal/sphenoidal) — intranasal mass, CSF leak, may be occult
- Size, skin coverage (CSF leak/ulceration risk), neurological function, feeding/airway (basal/nasal)
- Associated: hydrocephalus, Chiari, other anomalies (Meckel-Gruber, amniotic band), syndromic
Past Medical History / Birth
- Prenatal diagnosis, mode of delivery, maternal folate, gestational age
- Associated anomalies/syndrome, hydrocephalus, airway/feeding (basal)
- Latex precautions
- Standard neonatal history
Imaging Review
MRI brain (+ MRV)
- Contents of the sac (brain — eloquent/functional? gliotic? — vs CSF only), venous sinuses within the sac (occipital — torcula/transverse may herniate; MRV critical), brain malformations, hydrocephalus, Chiari
CT (bone, 3D)
- Bony defect size/location, skull base anatomy (basal/frontoethmoidal — reconstruction planning), orbital/nasal anatomy
Labs
- CBC, BMP, type and crossmatch (neonatal blood volume, venous sinus bleeding risk), Coags
- Latex-free
Examination
- Sac (size, skin coverage, transillumination, leak), neuro exam, head circumference/fontanelle, associated anomalies, airway (basal)
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: pediatric anesthesia/equipment, warming, weight-based implants/antibiotics, navigation/endoscope/microscope as needed, blood availability for tumor/myelomeningocele cases, and family-centered postop handoff.
- Special needs: weight-based fluids/meds, latex allergy precautions for myelomeningocele, steroid/endocrine/DI plan when sellar/posterior fossa risk exists, EVD/CSF diversion plan, and age-appropriate neuro baseline.
- Immediate postop orders: PICU/step-down neuro checks, airway/swallow monitoring when relevant, CT/MRI timing, drain/EVD/shunt orders, antibiotics/steroid taper, pain control, wound/skin precautions, and PT/OT/rehab planning.
Diagnosis & Indication / Timing
- Indication: Repair to protect herniated tissue, prevent CSF leak/meningitis, correct deformity; urgent if ruptured/leaking/thin skin; elective otherwise once stable
- Assess sac contents — non-functional gliotic tissue can be excised; functional brain or critical venous sinuses must be preserved/reduced (not sacrificed)
- Hydrocephalus often coexists → may need CSF diversion (before/after — untreated hydrocephalus → repair breakdown/leak)
Position
- Per location (prone for occipital; supine for frontoethmoidal/basal — may need craniofacial/ENT/transnasal), neonatal padding/thermoregulation, latex-free
Key Surgical Steps
- Approach the defect (skin incision around the sac / bicoronal for frontoethmoidal / endoscopic endonasal for selected basal)
- Open the sac, inspect contents: reduce viable/functional neural tissue and venous structures back intracranially; excise only non-functional gliotic tissue
- Identify and preserve dural venous sinuses (occipital — torcula/transverse can be in the sac; injury → catastrophic hemorrhage)
- Watertight dural closure (primary or graft) over the reduced contents
- Bony/skull base reconstruction — repair the bony defect (autograft/graft/titanium per age; cartilage/bone for skull base); for frontoethmoidal correct the orbital/nasal deformity (craniofacial)
- Multilayer closure to prevent CSF leak (dura, pericranium/fascia, bone, soft tissue, skin); vascularized pericranial/nasoseptal flap for skull base
- Address hydrocephalus (EVD/shunt/ETV) per status
Critical Anatomy & Structures at Risk
- Dural venous sinuses (occipital — torcula/transverse/sagittal) — major hemorrhage
- Functional brain tissue within the sac (preserve/reduce)
- Skull base / CSF spaces (leak), orbit/optic apparatus/nasal structures (frontoethmoidal/basal)
- Neonatal blood volume
Equipment
- Microscope (± endoscope for basal), neonatal/micro instruments, fine bipolar
- Dural substitute, pericranial/vascularized flap, bone/skull base reconstruction materials, sealant
- Crossmatched blood, thermoregulation, latex-free; craniofacial/ENT team (frontoethmoidal/basal)
Monitoring
- Neonatal anesthesia monitoring; VAE precautions (venous sinus exposure)
Anesthesia
- Neonatal general, crossmatched blood (sinus bleeding), thermoregulation/fluid/glucose, latex-free, VAE precautions
Potential Complications
- Hemorrhage (venous sinus), CSF leak / meningitis (closure integrity)
- Hydrocephalus (progressive — many need shunt/ETV; monitor), neurological deficit (functional tissue)
- Wound breakdown, cosmetic/deformity issues, recurrence; visual/nasal issues (anterior)
Operative Note Template
Preoperative Diagnosis: [Occipital/frontoethmoidal/basal/parietal] encephalocele
Postoperative Diagnosis: Same
Procedure: Repair of [location] encephalocele with multilayer dural and skull base reconstruction [± deformity correction / CSF diversion]
Surgeon / Assistant: [± craniofacial/ENT for frontoethmoidal/basal] Anesthesia: Neonatal general endotracheal, latex-free, thermoregulation EBL / Fluids / Blood products: [crossmatched — venous sinus risk] Adjuncts: Microscope [± endoscope], pericranial/vascularized flap, skull base reconstruction materials; VAE precautions Complications: None
Indications: [Age] infant with a [location] encephalocele; repair to protect herniated tissue, prevent CSF leak/meningitis, and correct deformity. Risks (venous sinus hemorrhage, CSF leak, hydrocephalus) discussed with family.
Description of Procedure: After consent and time-out, neonatal anesthesia was induced (latex-free, warming, crossmatched blood) with VAE precautions. The defect was approached [per location], the sac opened, and the contents inspected — viable/functional neural tissue and venous structures were reduced intracranially while non-functional gliotic tissue was excised; the dural venous sinuses were identified and preserved. A watertight dural closure was performed over the reduced contents, the bony/skull base defect reconstructed [graft/titanium per age; vascularized flap for skull base], and a multilayer soft-tissue/skin closure completed. [Hydrocephalus was addressed with EVD/shunt/ETV per status.]
The infant was transferred to the NICU with head-circumference/US monitoring and CSF-leak precautions.
Postoperative Plan
- NICU/PICU, positioning to protect the repair, neuro checks, head circumference/fontanelle and head US (hydrocephalus)
- CSF leak/wound monitoring, latex-free
- CSF diversion (shunt/ETV) if hydrocephalus progresses (common — can precipitate repair breakdown if untreated)
- MRI postop, craniofacial/ENT follow-up (frontoethmoidal/basal), genetics if syndromic
- Developmental follow-up, multidisciplinary care
Chief-Level Case Review
Use these as the senior-level mental model for Encephalocele Repair:
- Decision point: The setup is age-specific: blood volume, warming, positioning pressure, airway, latex risk, family counseling, and ICU/PICU handoff differ from adults.
- Technical lever: Preserve future options: growth, shunt dependence, cranioplasty/bone healing, endocrine/neurocognitive trajectory, and adjuvant therapy influence today’s choices.
- Bailout: Have a complication script: blood loss, CSF leak, hydrocephalus, wound breakdown, posterior fossa mutism, infection, and airway/swallow risk should be anticipated.
- Postop watch: Postop communication matters: family expectations, neurologic baseline, therapy needs, school/developmental supports, and surveillance imaging/labs should be clear.
Common Pimp Questions
Use these to pressure-test preparation for Encephalocele Repair:
- What age-specific anatomy, blood volume, temperature, and positioning issue changes the plan?
- What is the neurologic, developmental, or syndromic baseline?
- What skin, wound, CSF, or infection risk is highest in this child?
- What family-facing expectation should be clarified before surgery?
- What postop bed, feeding, pain, imaging, and activity plan is safest?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Blood availability threshold, warming strategy, antibiotic dosing, and Foley/drain use: [attending-specific]
- Positioning aids, pinning versus horseshoe, and skin-prep preference: [attending-specific]
- Family update cadence and expected ICU/floor disposition: [attending-specific]
- Postop feeding, pain regimen, wound care, and activity restrictions: [attending-specific]