
Case Prep: Craniosynostosis Repair
Case / Approach Snapshot
- Anatomy at risk: age-specific skull/soft tissue, developing brain and tracts, CSF pathways, brainstem/lower cranial nerves, tumor or congenital lesion relationships, and blood-volume constraints.
- Operative steps: adapt positioning/anesthesia to age, confirm imaging and goals with family, expose gently, preserve neurovascular/CSF pathways, reconstruct durably for growth, and plan ICU/endocrine/rehab surveillance; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: blood loss, hypothermia, swelling, hydrocephalus, airway/swallowing issues, endocrine/electrolyte shifts, infection, and staged therapy with oncology or rehab teams.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age — months] [M/F] infant with [sagittal / metopic / unicoronal / bicoronal / lambdoid] craniosynostosis [± syndromic] planned for [endoscopic strip craniectomy + helmet / open cranial vault remodeling].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Craniosynostosis - Recognition, clinical characteristics, and treatment — Kajdic N. Bosnian journal of basic medical sciences 2018. PubMed
- The clinical manifestations, molecular mechanisms and treatment of craniosynostosis — Stanton E. Disease models & mechanisms 2022. PubMed
- Craniosynostosis — Governale LS. Pediatric neurology 2015. PubMed
- Syndromic Craniosynostosis — Sawh-Martinez R. Clinics in plastic surgery 2019. PubMed
- Nonsyndromic Craniosynostosis — Dempsey RF. Clinics in plastic surgery 2019. PubMed
- Craniosynostosis — Kabbani H. American family physician 2004. PubMed
- Craniosynostosis: A Pediatric Neurologist’s Perspective — Shruthi NM. Journal of pediatric neurosciences 2022. PubMed
- FGFR Craniosynostosis Syndromes Overview — Adam MP. 1993. PubMed
- Imaging in craniosynostosis: when and what? — Massimi L. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2019. PubMed
- Craniosynostosis and oculomotor disorders — Dalmas F. Neuro-Chirurgie 2020. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
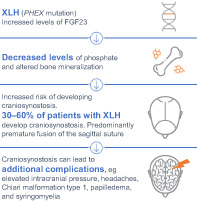 Figure 1. Source: Craniosynostosis in Patients With X‐Linked Hypophosphatemia: A Review — JBMR Plus. 2023 Mar 14;7(5):e10728. doi: 10.1002/jbm4.10728; CC BY.
Figure 1. Source: Craniosynostosis in Patients With X‐Linked Hypophosphatemia: A Review — JBMR Plus. 2023 Mar 14;7(5):e10728. doi: 10.1002/jbm4.10728; CC BY.
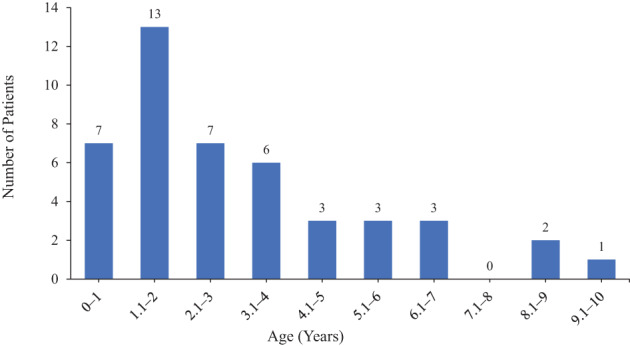 Fig. 2. Age distribution of craniosynostosis diagnosis in patients with XLH identified in this review. Note, the age of craniosynostosis diagnosis was not reported for all patients; this… Source: Craniosynostosis in Patients With X‐Linked Hypophosphatemia: A Review — JBMR Plus 2023; CC BY.
Fig. 2. Age distribution of craniosynostosis diagnosis in patients with XLH identified in this review. Note, the age of craniosynostosis diagnosis was not reported for all patients; this… Source: Craniosynostosis in Patients With X‐Linked Hypophosphatemia: A Review — JBMR Plus 2023; CC BY.
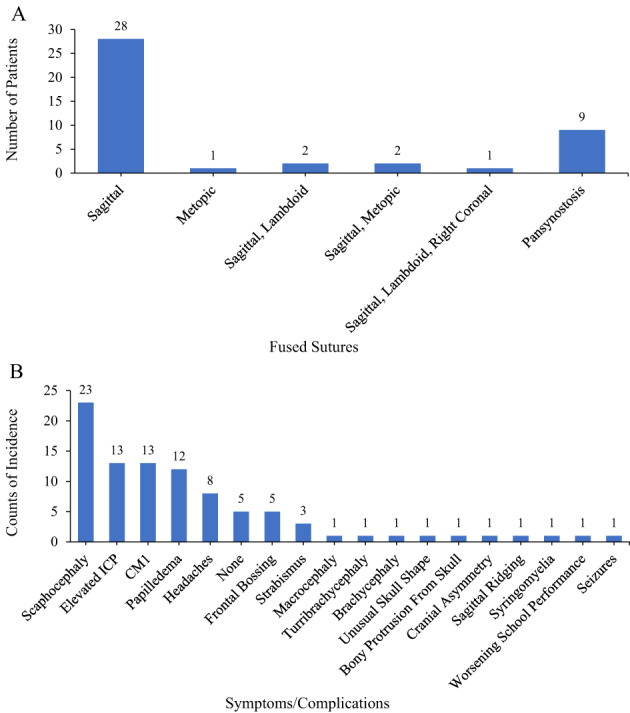 Fig. 3. (A) Distribution of fused sutures and (B) distribution of symptoms/complications in craniosynostosis in patients with XLH identified in this review. Note, the sutures fused were not… Source: Craniosynostosis in Patients With X‐Linked Hypophosphatemia: A Review — JBMR Plus 2023; CC BY.
Fig. 3. (A) Distribution of fused sutures and (B) distribution of symptoms/complications in craniosynostosis in patients with XLH identified in this review. Note, the sutures fused were not… Source: Craniosynostosis in Patients With X‐Linked Hypophosphatemia: A Review — JBMR Plus 2023; CC BY.
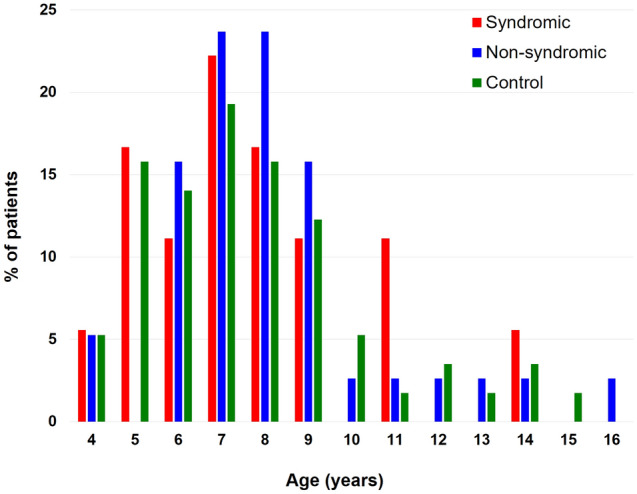 Figure 1. Age distribution of the syndromic craniosynostosis, non-syndromic craniosynostosis, and control groups. Source: Ocular biometric features of pediatric patients with fibroblast growth factor receptor-related syndromic craniosynostosis — Scientific Reports 2021; CC BY.
Figure 1. Age distribution of the syndromic craniosynostosis, non-syndromic craniosynostosis, and control groups. Source: Ocular biometric features of pediatric patients with fibroblast growth factor receptor-related syndromic craniosynostosis — Scientific Reports 2021; CC BY.
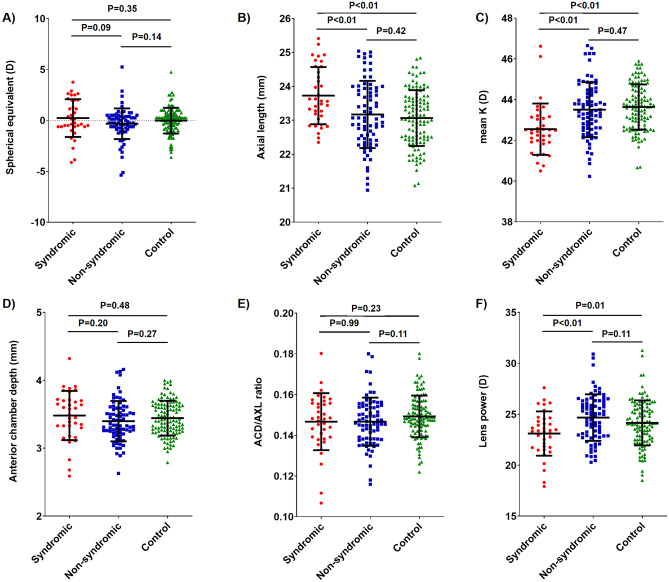 Figure 2. Comparison of biometric values between the syndromic craniosynostosis, non-syndromic craniosynostosis, and control groups. The distribution of (A) spherical equivalent, (B) axial length,… Source: Ocular biometric features of pediatric patients with fibroblast growth factor receptor-related syndromic craniosynostosis — Scientific Reports 2021; CC BY.
Figure 2. Comparison of biometric values between the syndromic craniosynostosis, non-syndromic craniosynostosis, and control groups. The distribution of (A) spherical equivalent, (B) axial length,… Source: Ocular biometric features of pediatric patients with fibroblast growth factor receptor-related syndromic craniosynostosis — Scientific Reports 2021; CC BY.
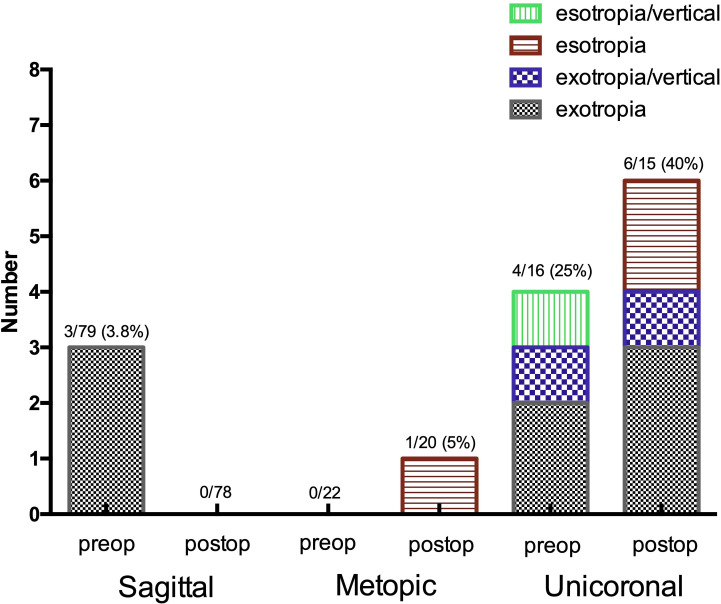 Figure 1. Prevalence of strabismus preoperatively and postoperatively in sagittal, unicoronal and metopic non-syndromic craniosynostosis. Source: Ophthalmological findings in children with non-syndromic craniosynostosis: preoperatively and postoperatively up to 12 months after surgery — BMJ Open Ophthalmology 2021; CC BY.
Figure 1. Prevalence of strabismus preoperatively and postoperatively in sagittal, unicoronal and metopic non-syndromic craniosynostosis. Source: Ophthalmological findings in children with non-syndromic craniosynostosis: preoperatively and postoperatively up to 12 months after surgery — BMJ Open Ophthalmology 2021; CC BY.
 Figure 8. Source: Ophthalmological findings in children with non-syndromic craniosynostosis: preoperatively and postoperatively up to 12 months after surgery — BMJ Open Ophthalmol. 2021 Apr 25;6(1):e000677. doi: 10.1136/bmjophth-2020-000677; CC BY.
Figure 8. Source: Ophthalmological findings in children with non-syndromic craniosynostosis: preoperatively and postoperatively up to 12 months after surgery — BMJ Open Ophthalmol. 2021 Apr 25;6(1):e000677. doi: 10.1136/bmjophth-2020-000677; CC BY.
 Figure 9. Source: Ophthalmological findings in children with non-syndromic craniosynostosis: preoperatively and postoperatively up to 12 months after surgery — BMJ Open Ophthalmol. 2021 Apr 25;6(1):e000677. doi: 10.1136/bmjophth-2020-000677; CC BY.
Figure 9. Source: Ophthalmological findings in children with non-syndromic craniosynostosis: preoperatively and postoperatively up to 12 months after surgery — BMJ Open Ophthalmol. 2021 Apr 25;6(1):e000677. doi: 10.1136/bmjophth-2020-000677; CC BY.
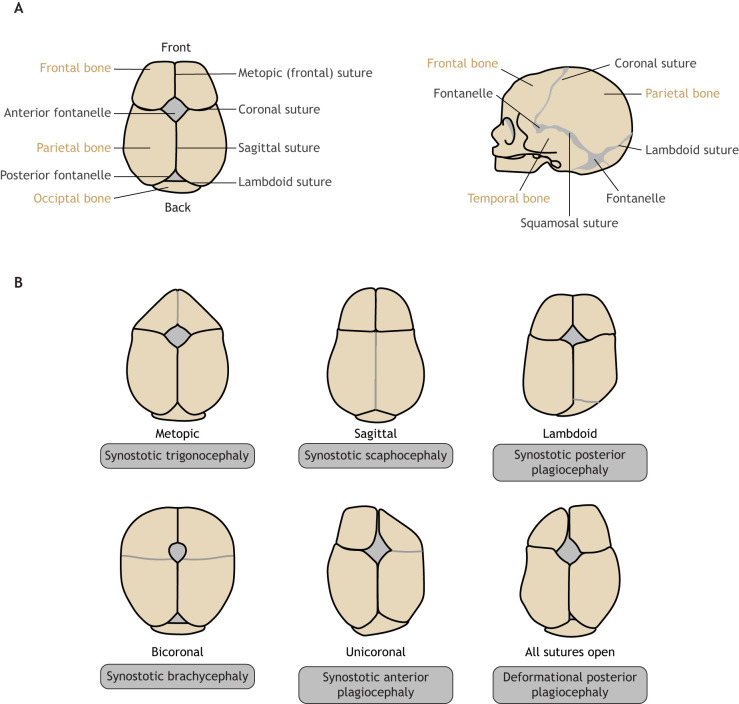 Fig. 1.. Cranial sutures and craniosynostosis in humans. (A) A normal human infant skull shown from above (left) and human infant skull shown from the side (right). (B) Skull deformities caused… Source: The clinical manifestations, molecular mechanisms and treatment of craniosynostosis — Disease Models & Mechanisms 2022; CC BY.
Fig. 1.. Cranial sutures and craniosynostosis in humans. (A) A normal human infant skull shown from above (left) and human infant skull shown from the side (right). (B) Skull deformities caused… Source: The clinical manifestations, molecular mechanisms and treatment of craniosynostosis — Disease Models & Mechanisms 2022; CC BY.
History of Present Illness
- Chief complaint: Abnormal head shape since birth, ridging over suture, ± raised ICP (multisuture/syndromic)
- Suture and head shape:
- Sagittal → scaphocephaly (long, narrow) — most common
- Metopic → trigonocephaly (triangular forehead, hypotelorism)
- Unicoronal → anterior plagiocephaly (forehead flattening, harlequin orbit)
- Bicoronal → brachycephaly (often syndromic)
- Lambdoid → posterior plagiocephaly (rare; distinguish from positional)
- Syndromic (Apert, Crouzon, Pfeiffer, Saethre-Chotzen, Muenke) — multisuture, raised ICP, midface
- Developmental milestones, signs of raised ICP
Past Medical History
- Syndromic features (limbs, midface, airway — Apert/Crouzon), genetics
- Airway issues (syndromic), feeding, OSA
- Birth/developmental history
Imaging Review
CT head with 3D reconstruction
- Confirm fused suture(s), head shape, exclude other sutures, ventricles, Chiari (lambdoid/syndromic), raised ICP signs (copper-beaten skull)
MRI (selective)
- Chiari, hydrocephalus, brain anomalies (syndromic)
Ophthalmology
- Papilledema (raised ICP)
Labs
- CBC, type and CROSSMATCH (blood loss can be significant in infants), coagulation
- Pre-op anesthesia/age-appropriate
Examination
- Head shape/circumference, suture ridging, fontanelle, neurological/developmental, eyes, syndromic features
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: pediatric anesthesia, blood conservation/cell saver per protocol, craniofacial/plastics trays, positioning pads, temperature management, tranexamic acid/blood products, and helmet pathway for endoscopic cases.
- Special needs: weight-based antibiotics/fluids/transfusion thresholds, arterial line for open vault cases, eye protection, hypothermia prevention, and family counseling about swelling and helmet therapy.
- Immediate postop orders: PICU neuro and airway checks, CBC/coags, drain care if used, pain/nausea regimen, head elevation, transfusion parameters, wound checks, and helmet/craniofacial follow-up.
Procedure Selection
- Endoscopic strip craniectomy: age < 3-6 months (younger = better — relies on rapid brain growth + postoperative molding helmet); minimal blood loss, short stay; for single-suture (esp. sagittal)
- Open cranial vault remodeling (CVR) / fronto-orbital advancement (FOA): older infants (typically 6-12 months), syndromic, multisuture, significant deformity; FOA for coronal/metopic (forehead/orbit); more blood loss, longer surgery
- Spring-assisted / distraction (select centers)
Position
- Endoscopic sagittal: prone or modified prone/sphinx; Open: supine (FOA) or prone (posterior); careful infant positioning/padding/thermoregulation
Key Surgical Steps
- Endoscopic strip craniectomy (sagittal): small incision(s), subgaleal/subperiosteal dissection, endoscopic dissection of the epidural plane, remove the fused suture strip (± lateral barrel-stave osteotomies/wedges), control sagittal sinus/bleeding, closure; helmet therapy starts ~1-2 weeks post-op for months
- Open CVR/FOA: bicoronal incision, scalp flap, craniotomies to remove and remodel bone, fronto-orbital bar advancement (FOA), reshape and refix vault with resorbable plates/sutures, expand the constricted dimension; meticulous hemostasis (blood loss)
Critical Anatomy & Structures at Risk
- Superior sagittal sinus (sagittal/under the strip) — major bleeding risk in a small infant
- Dura (tears, especially syndromic/older), bridging veins
- Orbit/globe, supraorbital nerves (FOA), frontal lobes
- Blood volume — infants have small total blood volume; significant relative blood loss
Equipment
- Endoscope + endoscopic craniectomy set OR open craniotomy/remodeling set
- Resorbable fixation plates/sutures, high-speed drill/craniotome
- Crossmatched blood (have in room), cell saver, tranexamic acid, hemostatic agents
- Molding helmet plan (endoscopic), thermoregulation
Monitoring
- Arterial line (open/blood loss), invasive monitoring; precordial Doppler (VAE — sinus exposure)
Anesthesia
- Arterial line, large-bore IV/central access, crossmatched blood ready, TXA, careful infant fluid/thermoregulation, VAE precautions (sagittal sinus), blood loss vigilance
Potential Complications
- Hemorrhage / blood loss (transfusion usually needed in open; lower in endoscopic)
- Venous air embolism (sinus exposure)
- Dural tear/CSF leak, sagittal sinus injury
- Under/over-correction, need for revision, raised ICP persistence (syndromic)
- Infection, hardware issues, helmet compliance (endoscopic)
Operative Note Template
Preoperative Diagnosis: [Sagittal/metopic/unicoronal/bicoronal] craniosynostosis [± syndromic]
Postoperative Diagnosis: Same
Procedure: [Endoscopic-assisted strip craniectomy for sagittal synostosis / Open cranial vault remodeling with fronto-orbital advancement]
Surgeon / Assistant: Neurosurgery + craniofacial/plastics Anesthesia: General endotracheal EBL / Fluids / Blood products: [crossmatched in room; TXA; cell saver] Adjuncts: [Endoscope] / craniotome, resorbable fixation; arterial line; VAE precautions (precordial Doppler) Implants: Resorbable plates/sutures Complications: None
Indications: [Age — months] infant with [suture] synostosis ([head-shape]); [endoscopic strip chosen given age < 3–6 months with planned helmet / open CVR-FOA given older age/deformity]. Risks (blood loss/transfusion, VAE, dural tear) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced with arterial access, crossmatched blood in the room, and TXA; VAE precautions were observed. [Endoscopic: a small incision, subgaleal/epidural endoscopic dissection, and removal of the fused sagittal suture strip (± barrel-stave wedges) with sagittal-sinus/bleeding control.] [Open: a bicoronal incision and scalp flap, craniotomies to remove and remodel the vault with fronto-orbital bar advancement, reshaping and refixing with resorbable plates.] Meticulous hemostasis was maintained given the infant blood volume.
Closure was performed. The patient was transferred to the [PICU/floor] with Hgb/transfusion monitoring; [helmet therapy was planned ~1–2 weeks post-op for the endoscopic case].
Postoperative Plan
- PICU (open/blood loss) or floor (endoscopic), neuro checks, monitor Hgb/transfusion needs
- Facial/periorbital swelling (FOA — eyes may swell shut, reassure), head dressing
- Helmet therapy ~1-2 weeks post-op (endoscopic) for several months; helmet/orthotist referral
- Pain control, feeding, thermoregulation
- Craniofacial team follow-up, genetics (syndromic), ophthalmology, head shape/circumference surveillance
- Long-term: monitor for raised ICP, reossification, need for revision (syndromic)
Chief-Level Case Review
Use these as the senior-level mental model for Craniosynostosis Repair:
- Decision point: The setup is age-specific: blood volume, warming, positioning pressure, airway, latex risk, family counseling, and ICU/PICU handoff differ from adults.
- Technical lever: Preserve future options: growth, shunt dependence, cranioplasty/bone healing, endocrine/neurocognitive trajectory, and adjuvant therapy influence today’s choices.
- Bailout: Have a complication script: blood loss, CSF leak, hydrocephalus, wound breakdown, posterior fossa mutism, infection, and airway/swallow risk should be anticipated.
- Postop watch: Postop communication matters: family expectations, neurologic baseline, therapy needs, school/developmental supports, and surveillance imaging/labs should be clear.
Common Pimp Questions
Use these to pressure-test preparation for Craniosynostosis Repair:
- What age-specific anatomy, blood volume, temperature, and positioning issue changes the plan?
- What is the neurologic, developmental, or syndromic baseline?
- What skin, wound, CSF, or infection risk is highest in this child?
- What family-facing expectation should be clarified before surgery?
- What postop bed, feeding, pain, imaging, and activity plan is safest?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Blood availability threshold, warming strategy, antibiotic dosing, and Foley/drain use: [attending-specific]
- Positioning aids, pinning versus horseshoe, and skin-prep preference: [attending-specific]
- Family update cadence and expected ICU/floor disposition: [attending-specific]
- Postop feeding, pain regimen, wound care, and activity restrictions: [attending-specific]