
Case Prep: Mechanical Thrombectomy for Acute Ischemic Stroke (Large Vessel Occlusion)
Case / Approach Snapshot
- Anatomy at risk: access vessels, arch/cervical anatomy, parent artery branches, perforators, collateral pathways, venous drainage when relevant, and device landing zones.
- Operative steps: confirm indication and imaging, obtain access safely, navigate with roadmap control, deploy the planned device or embolic strategy, document final angiography, and define antiplatelet/anticoagulation and postprocedure monitoring; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: access complication, dissection/perforation, thromboembolism, device malposition or migration, hemorrhage, vasospasm, antiplatelet failure, and conversion to open or staged management.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with acute ischemic stroke from a [left/right] [ICA / M1 / M2 / basilar] large vessel occlusion (NIHSS [__]) planned for emergent mechanical thrombectomy.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · neuroangio.org · Radiopaedia · PubMed Central — figures © linked; see media-sources.md
High-Yield Literature
- Contemporary Management of Acute Ischemic Stroke — Ho JP. Annual review of medicine 2025. PubMed
- Acute ischemic stroke: A guideline-based overview of evaluation and management — Bogenschutz KM. JAAPA : official journal of the American Academy of Physician Assistants 2025. PubMed
- A review of mechanical thrombectomy techniques for acute ischemic stroke — Munoz A. Interventional neuroradiology : journal of peritherapeutic neuroradiology, surgical procedures and related neurosciences 2023. PubMed
- Indications for Mechanical Thrombectomy for Acute Ischemic Stroke: Current Guidelines and Beyond — Jadhav AP. Neurology 2021. PubMed
- Management of acute ischemic stroke — Rigual R. Medicina clinica 2023. PubMed
- Diagnosis and Management of Transient Ischemic Attack and Acute Ischemic Stroke: A Review — Mendelson SJ. JAMA 2021. PubMed
- Mechanical Thrombectomy for Acute Ischemic Stroke — Sheth SA. Continuum (Minneapolis, Minn.) 2023. PubMed
- European Stroke Organisation (ESO) - European Society for Minimally Invasive Neurological Therapy (ESMINT) Guidelines on Mechanical Thrombectomy in Acute Ischemic Stroke — Turc G. Journal of neurointerventional surgery 2023. PubMed
- Thrombus Composition and Efficacy of Thrombolysis and Thrombectomy in Acute Ischemic Stroke — Jolugbo P. Stroke 2021. PubMed
- Advances in Acute Ischemic Stroke Therapy — Xiong Y. Circulation research 2022. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
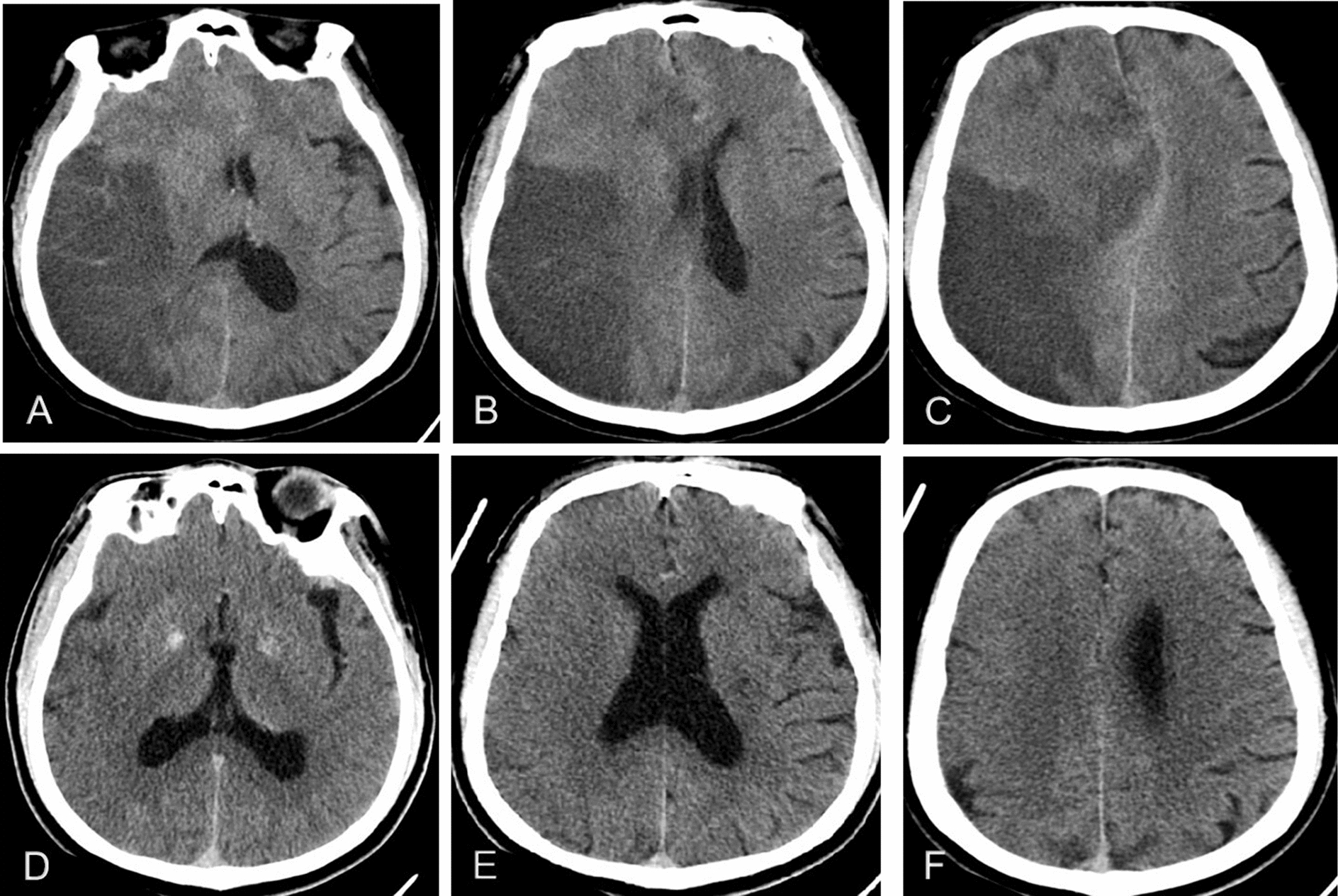 Fig. 2. Typical images of MBE after MT: 59-year-old man with mTICI score, 2b; and mRS score, 4; A–C post-treatment patient with cerebral edema on CT image; D–F pre-treatment patient without… Source: The risk and outcome of malignant brain edema in post-mechanical thrombectomy: acute ischemic stroke by anterior circulation occlusion — European Journal of Medical Research 2023; CC BY.
Fig. 2. Typical images of MBE after MT: 59-year-old man with mTICI score, 2b; and mRS score, 4; A–C post-treatment patient with cerebral edema on CT image; D–F pre-treatment patient without… Source: The risk and outcome of malignant brain edema in post-mechanical thrombectomy: acute ischemic stroke by anterior circulation occlusion — European Journal of Medical Research 2023; CC BY.
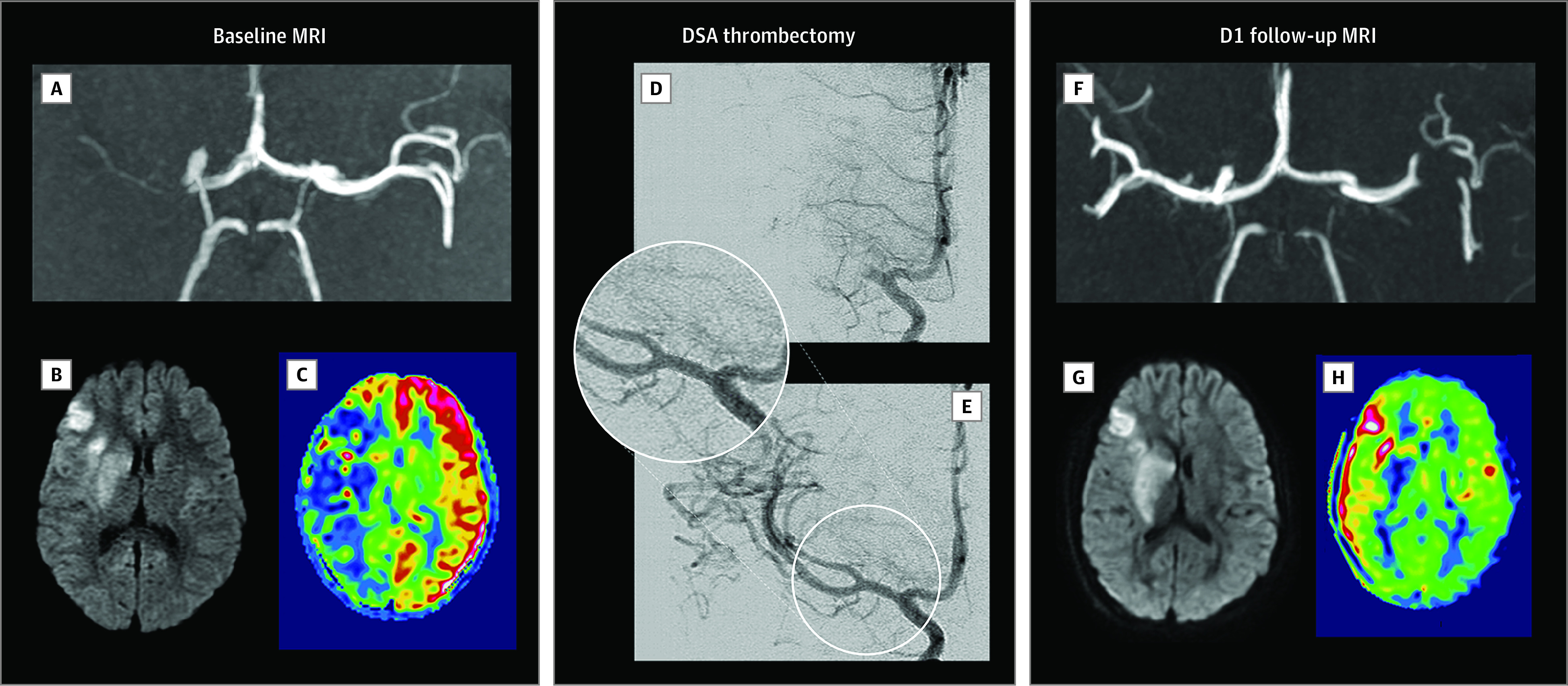 Figure 1.. Pediatric Acute Ischemic Stroke of Cardioembolic Origin Treated With Mechanical ThrombectomyAcute ischemic stroke in a child aged 8 years with a clinical history of embolic heart disease… Source: Recanalization Treatments for Pediatric Acute Ischemic Stroke in France — JAMA Network Open 2022; CC BY.
Figure 1.. Pediatric Acute Ischemic Stroke of Cardioembolic Origin Treated With Mechanical ThrombectomyAcute ischemic stroke in a child aged 8 years with a clinical history of embolic heart disease… Source: Recanalization Treatments for Pediatric Acute Ischemic Stroke in France — JAMA Network Open 2022; CC BY.
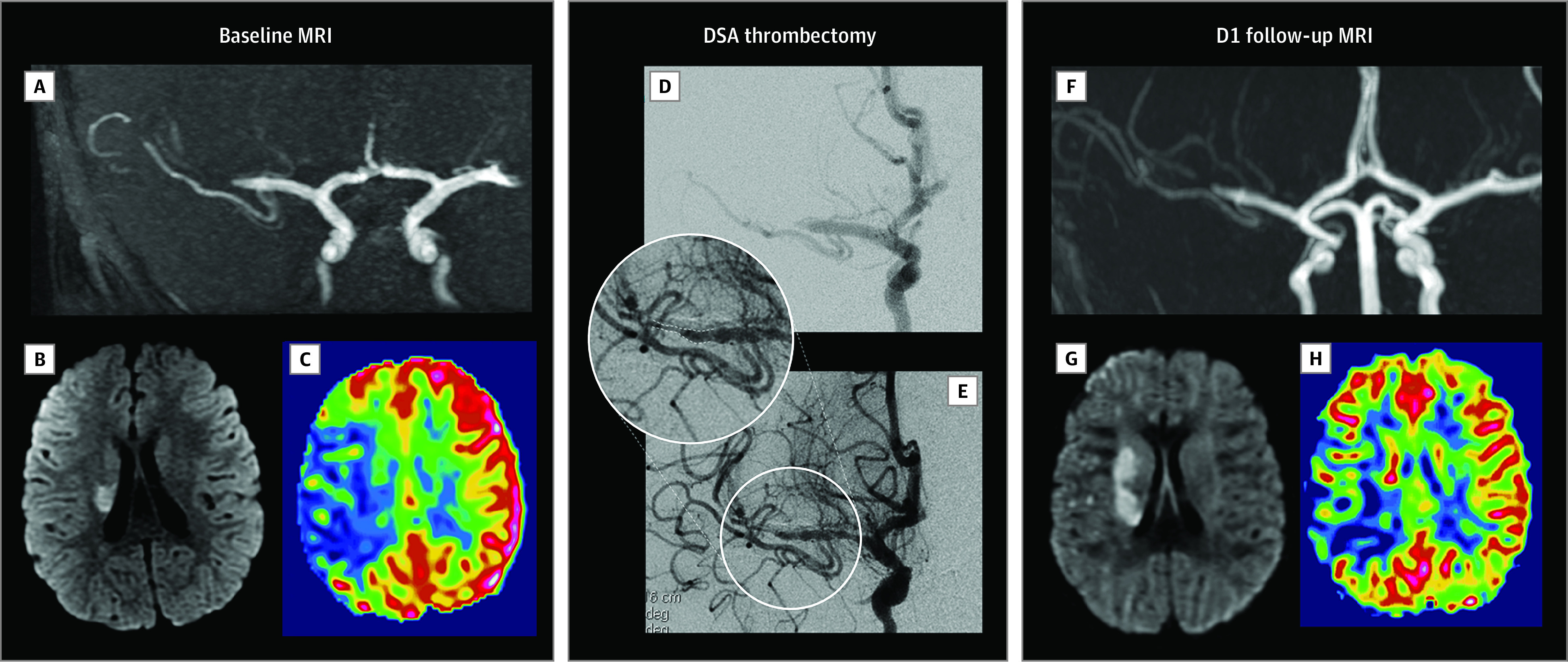 Figure 2.. Pediatric Acute Ischemic Stroke Caused by FCA Treated With Mechanical ThrombectomyAcute ischemic stroke in a child aged 4 years with no medical history, presenting as a sudden left… Source: Recanalization Treatments for Pediatric Acute Ischemic Stroke in France — JAMA Network Open 2022; CC BY.
Figure 2.. Pediatric Acute Ischemic Stroke Caused by FCA Treated With Mechanical ThrombectomyAcute ischemic stroke in a child aged 4 years with no medical history, presenting as a sudden left… Source: Recanalization Treatments for Pediatric Acute Ischemic Stroke in France — JAMA Network Open 2022; CC BY.
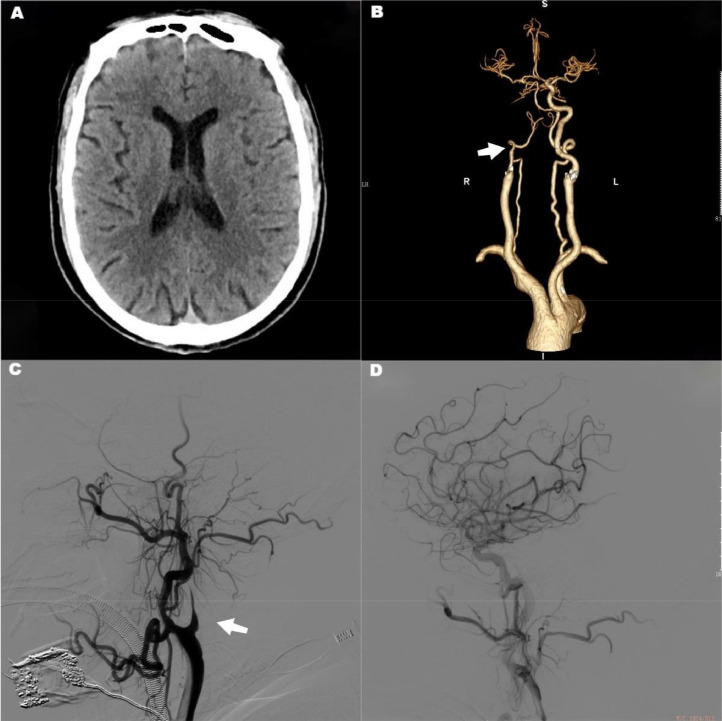 Fig. 1. The first mechanical thrombectomy, from A–D, showed no low-density lesions on preoperative head CT, occlusion of the right internal carotid artery (arrow), complete recanalization of the… Source: Two mechanical thrombectomies in acute ischemic stroke within 48 hours: A case report on a patient with atrial fibrillation — Radiology Case Reports 2023; CC BY-NC-ND.
Fig. 1. The first mechanical thrombectomy, from A–D, showed no low-density lesions on preoperative head CT, occlusion of the right internal carotid artery (arrow), complete recanalization of the… Source: Two mechanical thrombectomies in acute ischemic stroke within 48 hours: A case report on a patient with atrial fibrillation — Radiology Case Reports 2023; CC BY-NC-ND.
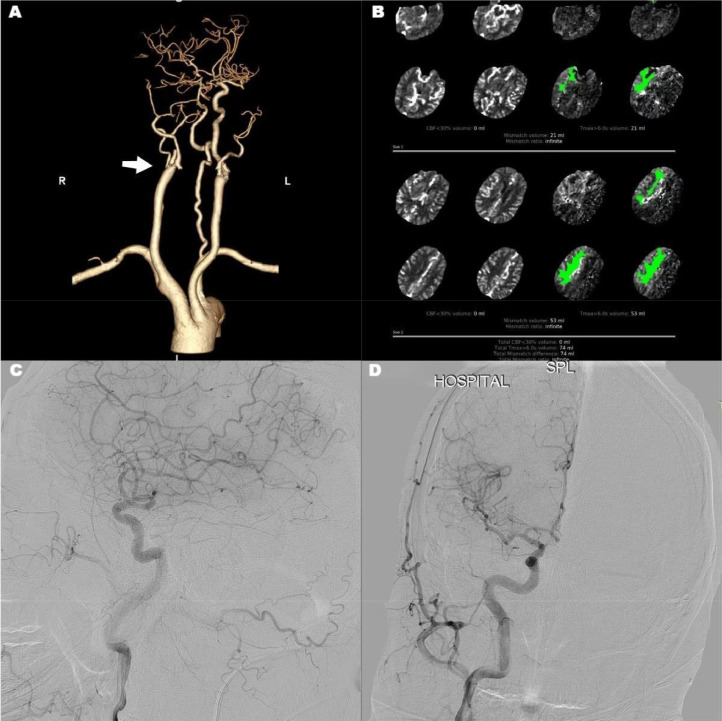 Fig. 2. The second mechanical thrombectomy, from A–D, suggested a recurrence of right-side internal carotid artery (arrow) occlusion, a mismatch between CT perfusion ischemia and core infarct… Source: Two mechanical thrombectomies in acute ischemic stroke within 48 hours: A case report on a patient with atrial fibrillation — Radiology Case Reports 2023; CC BY-NC-ND.
Fig. 2. The second mechanical thrombectomy, from A–D, suggested a recurrence of right-side internal carotid artery (arrow) occlusion, a mismatch between CT perfusion ischemia and core infarct… Source: Two mechanical thrombectomies in acute ischemic stroke within 48 hours: A case report on a patient with atrial fibrillation — Radiology Case Reports 2023; CC BY-NC-ND.
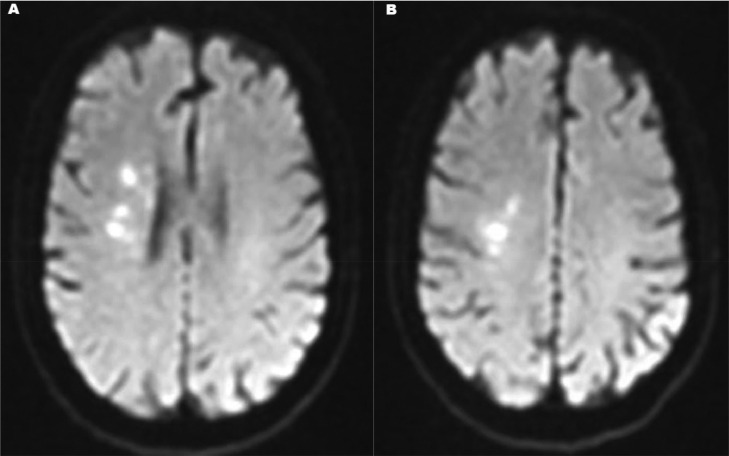 Fig. 3. After repeated mechanical thrombectomy, diffusion-weighted imaging (DWI) shows a small infarct area. Source: Two mechanical thrombectomies in acute ischemic stroke within 48 hours: A case report on a patient with atrial fibrillation — Radiology Case Reports 2023; CC BY-NC-ND.
Fig. 3. After repeated mechanical thrombectomy, diffusion-weighted imaging (DWI) shows a small infarct area. Source: Two mechanical thrombectomies in acute ischemic stroke within 48 hours: A case report on a patient with atrial fibrillation — Radiology Case Reports 2023; CC BY-NC-ND.
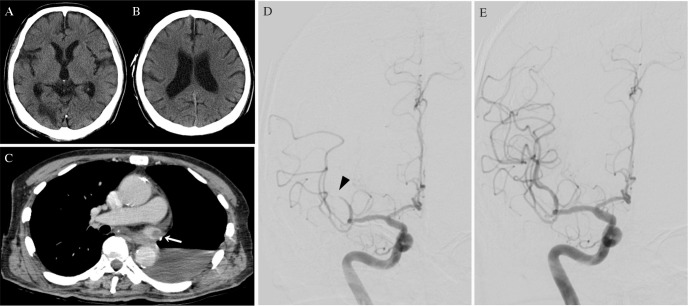 Fig. 1. (A and B) Axial plain computed tomography showing an old infarction in the right occipital lobe and early ischemic change in the right middle frontal gyrus. (C) Axial contrast-enhanced… Source: Mechanical Thrombectomy for Acute Ischemic Stroke Arising from Thrombus of the Left Superior Pulmonary Vein Stump after Left Pneumonectomy: A Case Report — NMC Case Report Journal 2019; CC BY-NC-ND.
Fig. 1. (A and B) Axial plain computed tomography showing an old infarction in the right occipital lobe and early ischemic change in the right middle frontal gyrus. (C) Axial contrast-enhanced… Source: Mechanical Thrombectomy for Acute Ischemic Stroke Arising from Thrombus of the Left Superior Pulmonary Vein Stump after Left Pneumonectomy: A Case Report — NMC Case Report Journal 2019; CC BY-NC-ND.
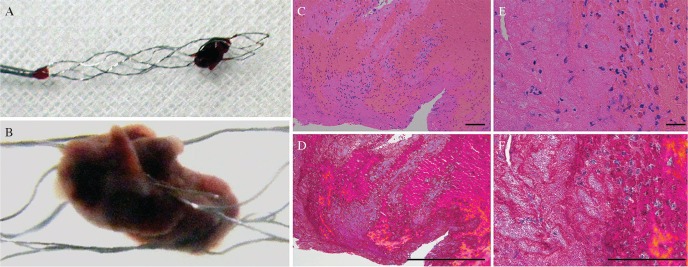 Fig. 2. Macroscopic photograph (A and B) and histological findings (C–F) of the retrieved embolus. The retrieved embolus appears as dark-red structure, and considers to be red thrombus (A,… Source: Mechanical Thrombectomy for Acute Ischemic Stroke Arising from Thrombus of the Left Superior Pulmonary Vein Stump after Left Pneumonectomy: A Case Report — NMC Case Report Journal 2019; CC BY-NC-ND.
Fig. 2. Macroscopic photograph (A and B) and histological findings (C–F) of the retrieved embolus. The retrieved embolus appears as dark-red structure, and considers to be red thrombus (A,… Source: Mechanical Thrombectomy for Acute Ischemic Stroke Arising from Thrombus of the Left Superior Pulmonary Vein Stump after Left Pneumonectomy: A Case Report — NMC Case Report Journal 2019; CC BY-NC-ND.
 Fig. 3. Post-operative findings of the imaging studies. Transesophageal echocardiography 6 days after thrombectomy (A) shows thrombus (arrow) in the left superior pulmonary vein stump…. Source: Mechanical Thrombectomy for Acute Ischemic Stroke Arising from Thrombus of the Left Superior Pulmonary Vein Stump after Left Pneumonectomy: A Case Report — NMC Case Report Journal 2019; CC BY-NC-ND.
Fig. 3. Post-operative findings of the imaging studies. Transesophageal echocardiography 6 days after thrombectomy (A) shows thrombus (arrow) in the left superior pulmonary vein stump…. Source: Mechanical Thrombectomy for Acute Ischemic Stroke Arising from Thrombus of the Left Superior Pulmonary Vein Stump after Left Pneumonectomy: A Case Report — NMC Case Report Journal 2019; CC BY-NC-ND.
History of Present Illness
- Chief complaint: Acute focal neurological deficit (hemiparesis, aphasia, gaze deviation, neglect)
- Last known well (LKW) time — critical for eligibility; NIHSS
- IV thrombolysis (tPA/TNK) given? (bridging — thrombectomy still indicated for LVO)
- Time windows: early (<6h) by imaging; extended (6-24h) if favorable perfusion/clinical-core mismatch (DAWN/DEFUSE-3)
- Wake-up stroke, contraindications to tPA
Past Medical History
- Atrial fibrillation/cardioembolic source, prior stroke, anticoagulation, vascular risk factors, prior MI
- Renal function (contrast), access anatomy
- Standard PMH; goals of care / baseline function (mRS)
Imaging Review
Non-contrast CT + CTA + (CT perfusion / MRI)
- NCCT: exclude hemorrhage, ASPECTS score (early ischemic change — low ASPECTS = large established core, less benefit)
- CTA: confirm and localize the LVO (ICA, M1, M2, basilar, tandem cervical occlusion), collaterals, arch/access
- CT perfusion / MRI DWI-perfusion: core vs penumbra mismatch (extended window selection — salvageable tissue)
Labs
- POC glucose, Coags/INR (if on anticoagulation), CBC, BMP — do NOT delay thrombectomy for labs in eligible patients
- Type and screen
Neurological Examination
- NIHSS, gaze, language, motor, level of consciousness (basilar — coma); rapid, serial
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: biplane angio suite, thrombectomy catheters/stent retrievers/aspiration, radial/femoral access supplies, anesthesia airway plan, CT/CTA/perfusion images loaded, and bailout stents/balloons available.
- Special needs: BP target tied to reperfusion status, anticoagulation/antiplatelet decision, groin/radial closure plan, tPA/tenecteplase history, contrast/renal/allergy plan, and ICU-ready post-recanalization hemorrhage pathway.
- Immediate postop orders: NIHSS/neuro checks, puncture-site and distal-pulse checks, BP ceiling per TICI/hemorrhage risk, 24h CT/MRI before antithrombotics when lytic used, swallow screen, statin/secondary prevention, and stroke workup.
Indication / Time
- Emergent — “time is brain”; eligible LVO (ICA/M1, selected M2/basilar) within window with salvageable tissue
- Goal: reperfusion (TICI 2b-3) as fast as possible
Position / Setup
- Supine, angiography table, femoral (or radial/direct carotid) access, biplane DSA
- Anesthesia: conscious sedation vs general (institutional; avoid BP drops with GA — hypotension worsens penumbra)
Key Procedure Steps
- Rapid arterial access (femoral sheath), guide/balloon-guide catheter to the cervical ICA/vertebral
- Diagnostic run to confirm occlusion and define anatomy
- Navigate to the clot:
- Stent retriever: cross the clot with microcatheter/wire, deploy stentriever across the thrombus, allow integration, retrieve (often with balloon-guide flow arrest + aspiration)
- Aspiration (ADAPT): large-bore aspiration catheter to the clot face, aspirate
- Often combined (stentriever + aspiration)
- Reassess reperfusion after each pass (TICI grade); repeat passes as needed (balance with futility/complications)
- Treat tandem lesions (cervical ICA stenosis/occlusion — angioplasty/stent) as needed
- Final angiography (TICI 2b-3 goal), access closure
Critical Anatomy & Structures at Risk
- Occluded artery and distal territory — reperfusion vs reocclusion/distal embolization to new territory
- Vessel wall — perforation/dissection/SAH (wire/device)
- Already-ischemic brain — reperfusion hemorrhage (esp. large core, post-tPA)
- Access vessels
Equipment / Team
- Neuroangiography suite, balloon-guide/guide catheters, stent retrievers, aspiration catheters, microcatheters/wires
- Angioplasty/stent (tandem), heparin (judicious), contrast
- Stroke team + neurointervention + anesthesia (door-to-puncture/recanalization metrics)
Anesthesia
- Conscious sedation or GA; strict BP management — avoid hypotension (penumbra) pre-reperfusion; after reperfusion, lower BP target (reduce hemorrhage)
Potential Complications
- Symptomatic intracranial hemorrhage / reperfusion hemorrhage, vessel perforation/SAH, dissection
- Distal/new-territory embolization, reocclusion, failed reperfusion
- Access complications, contrast nephropathy, futile recanalization (large core)
Procedure Note Template
Preoperative Diagnosis: Acute ischemic stroke from [left/right] [ICA/M1/M2/basilar] large-vessel occlusion (NIHSS [__])
Postoperative Diagnosis: Same
Procedure: Mechanical thrombectomy of [vessel] occlusion — [stent retriever / aspiration / combined], [N] passes, final [TICI __]
Operator / Assistant: Anesthesia: [Conscious sedation / general] Access: [Right femoral/radial] sheath Contrast / Fluoro time: Devices: [Stent retriever / aspiration catheter / balloon-guide] Complications: None
Indications: [Age]yo [M/F] with an acute [vessel] LVO (NIHSS [], ASPECTS [], LKW [time], [tPA given]) and [favorable core/penumbra] — emergent thrombectomy indicated. Risks (reperfusion hemorrhage, perforation, distal embolization) discussed.
Description of Procedure: After time-out (expedited for stroke), [conscious sedation] with strict BP management (avoiding hypotension pre-reperfusion) was provided and rapid arterial access obtained. A [balloon-]guide catheter was advanced to the cervical [ICA/vertebral] and a diagnostic run confirmed the [vessel] occlusion. The clot was crossed and [a stent retriever deployed and retrieved with flow arrest/aspiration / direct aspiration performed]; reperfusion was reassessed after each pass ([N] passes). [A tandem cervical lesion was treated with angioplasty/stent.]
Final angiography demonstrated [TICI __] reperfusion without distal embolization. Catheters were removed and the access closed.
The patient was transferred to the NSICU/stroke unit with a lowered BP target post-reperfusion; a 24h NCCT was planned before antithrombotics.
Post-Procedure Plan
- NSICU/stroke unit, neuro checks q15min→hourly, NIHSS
- BP management (post-reperfusion target lower, e.g., < 160-180 or per recanalization status; avoid extremes), access/pulse checks
- NCCT at ~24h (and for any deterioration) — hemorrhage before starting/restarting antithrombotics; tPA patients delay antithrombotics 24h
- Stroke workup (etiology — echo, telemetry/AF, vessel imaging, labs), start secondary prevention (antiplatelet/anticoagulation per cause and bleed status)
- DVT prophylaxis (after hemorrhage excluded), dysphagia screen, early rehab, goals of care
Chief-Level Case Review
Use these as the senior-level mental model for Mechanical Thrombectomy for Acute Ischemic Stroke (Large Vessel Occlusion):
- Decision point: The operation is won or lost on control: identify inflow, outflow, perforators, collateral options, and the fastest route to temporary control before exposing the lesion itself.
- Technical lever: Do not accept a cosmetic result over physiology: ICG/Doppler/DSA, branch patency, perforator preservation, and parent-vessel caliber matter more than how the clip or resection bed looks.
- Bailout: Have a rupture or ischemia script ready: lower pressure, suction strategy, temporary occlusion time, heparin/reversal plan, bypass/reconstruction threshold, and postop BP targets.
- Postop watch: Postop danger is delayed: vasospasm, thromboembolism, hyperperfusion, hemorrhage, edema, hydrocephalus, and seizure plans need explicit orders.
Common Pimp Questions
Use these to pressure-test preparation for Mechanical Thrombectomy for Acute Ischemic Stroke (Large Vessel Occlusion):
- What is the proximal-control plan before the lesion is manipulated?
- Which branch, perforator, or venous structure is most likely to be injured in this exposure?
- What are the intraoperative rupture steps, including temporary clip, suction, BP, and backup clip strategy?
- What confirms treatment success: ICG, Doppler, puncture/deflation, DSA, or postoperative CTA?
- What postoperative BP, vasospasm, antiplatelet, or anticoagulation issue changes the orders tonight?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Preferred approach side, sylvian split style, and cisternal-opening sequence: [attending-specific]
- Temporary clip threshold, burst-suppression preference, and BP during occlusion: [attending-specific]
- Clip manufacturer/shape sequence and whether Doppler, ICG, puncture, or intraop DSA is routine: [attending-specific]
- Antiplatelet/anticoagulation reversal and restart timing: [attending-specific]