
Case Prep: Carotid Artery Angioplasty and Stenting (CAS)
Case / Approach Snapshot
- Anatomy at risk: access vessels, arch/cervical anatomy, parent artery branches, perforators, collateral pathways, venous drainage when relevant, and device landing zones.
- Operative steps: confirm indication and imaging, obtain access safely, navigate with roadmap control, deploy the planned device or embolic strategy, document final angiography, and define antiplatelet/anticoagulation and postprocedure monitoring; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: access complication, dissection/perforation, thromboembolism, device malposition or migration, hemorrhage, vasospasm, antiplatelet failure, and conversion to open or staged management.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [symptomatic/asymptomatic] [left/right] internal carotid stenosis ([__]%) and [high surgical risk / hostile neck / re-stenosis after CEA] planned for carotid artery angioplasty and stenting with embolic protection.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · neuroangio.org · Radiopaedia · PubMed Central — figures © linked; see media-sources.md
High-Yield Literature
- Casper vs. Closed-Cell Stent : Carotid Artery Stenting Randomized Trial — Vanzin JR. Clinical neuroradiology 2021. PubMed
- Early versus late carotid artery stenting for symptomatic carotid stenosis — de Castro-Afonso LH. Journal of neuroradiology = Journal de neuroradiologie 2015. PubMed
- Is carotid artery stenting equivalent or superior to carotid endarterectomy for treatment of carotid artery stenosis? — Shrivastava V. Interactive cardiovascular and thoracic surgery 2005. PubMed
- Flow reversal versus filter protection: a pilot carotid artery stenting randomized trial — Castro-Afonso LH. Circulation. Cardiovascular interventions 2013. PubMed
- Carotid artery revascularization using the Walrus balloon guide catheter: safety and feasibility from a US multicenter experience — Salem MM. Journal of neurointerventional surgery 2022. PubMed
- Why the United States Center for Medicare and Medicaid Services (CMS) should not extend reimbursement indications for carotid artery angioplasty/stenting — Brain and behavior 2012. PubMed
- Advances and innovations in revascularization of extracranial vertebral artery — Brasiliense LB. Neurosurgery 2014. PubMed
- Characteristics from the 100 most influential articles on carotid stenosis — Hwang JW. Annals of palliative medicine 2022. PubMed
- Why the United States Center for Medicare and Medicaid Services should not extend reimbursement indications for carotid artery angioplasty/stenting — Abbott AL. Vascular 2012. PubMed
- Periprocedural embolic events related to carotid artery stenting detected by diffusion-weighted MRI: comparison between proximal and distal embolus protection devices — El-Koussy M. Journal of endovascular therapy : an official journal of the International Society of Endovascular Specialists 2007. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
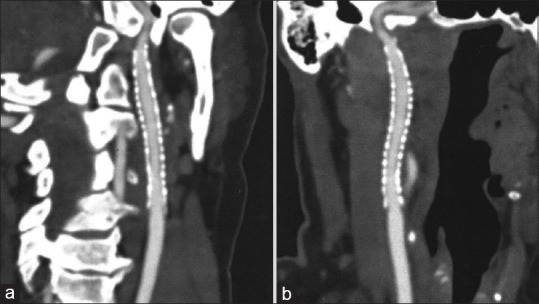 Figure 2. (a) Follow-up computed tomography angiogram, 12 months after stenting. The image showing the right cervical internal carotid artery in the sagittal plane. (b) Follow-up computed… Source: Casper stent in the treatment of pulsatile tinnitus in fibromuscular dysplasia: Therapeutic review and case report — Brain Circulation 2021; CC BY-NC-SA.
Figure 2. (a) Follow-up computed tomography angiogram, 12 months after stenting. The image showing the right cervical internal carotid artery in the sagittal plane. (b) Follow-up computed… Source: Casper stent in the treatment of pulsatile tinnitus in fibromuscular dysplasia: Therapeutic review and case report — Brain Circulation 2021; CC BY-NC-SA.
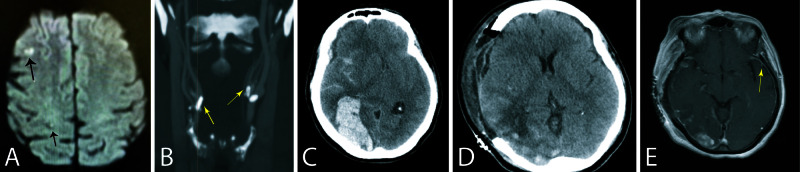 Figure 1. Pre- and post-operative brain images.A: Pre-operative diffusion weighted brain MRI showing previous punctate infarcts in the right middle cerebral artery territory (arrows). B: Cervical… Source: Concomitant Reversible Cerebral Vasoconstriction and Hyperperfusion Syndromes Following Carotid Endarterectomy — Cureus 2020; CC BY.
Figure 1. Pre- and post-operative brain images.A: Pre-operative diffusion weighted brain MRI showing previous punctate infarcts in the right middle cerebral artery territory (arrows). B: Cervical… Source: Concomitant Reversible Cerebral Vasoconstriction and Hyperperfusion Syndromes Following Carotid Endarterectomy — Cureus 2020; CC BY.
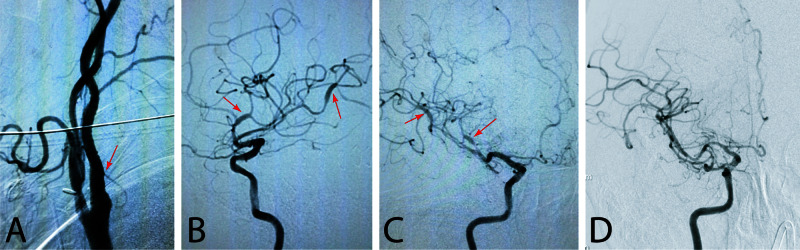 Figure 2. Cerebral angiogram.A: Catheter angiogram images showing resolution of right internal carotid artery stenosis after endarterectomy. Arrow points to the internal carotid artery…. Source: Concomitant Reversible Cerebral Vasoconstriction and Hyperperfusion Syndromes Following Carotid Endarterectomy — Cureus 2020; CC BY.
Figure 2. Cerebral angiogram.A: Catheter angiogram images showing resolution of right internal carotid artery stenosis after endarterectomy. Arrow points to the internal carotid artery…. Source: Concomitant Reversible Cerebral Vasoconstriction and Hyperperfusion Syndromes Following Carotid Endarterectomy — Cureus 2020; CC BY.
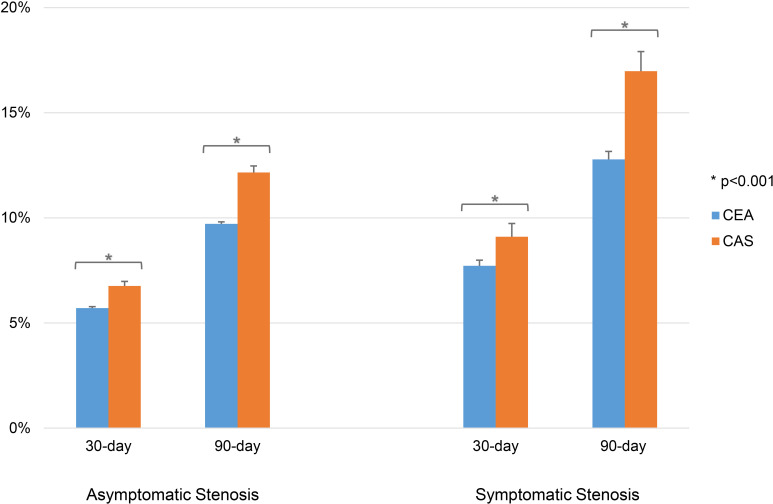 Figure 1. Readmission rates after CEA or CAS in asymptomatic and symptomatic patients. CAS=carotid artery stenting; CEA=carotid endarterectomy. Source: Unplanned readmission after carotid stenting versus endarterectomy: analysis of the United States Nationwide Readmissions Database — Journal of Neurointerventional Surgery 2023; CC BY-NC.
Figure 1. Readmission rates after CEA or CAS in asymptomatic and symptomatic patients. CAS=carotid artery stenting; CEA=carotid endarterectomy. Source: Unplanned readmission after carotid stenting versus endarterectomy: analysis of the United States Nationwide Readmissions Database — Journal of Neurointerventional Surgery 2023; CC BY-NC.
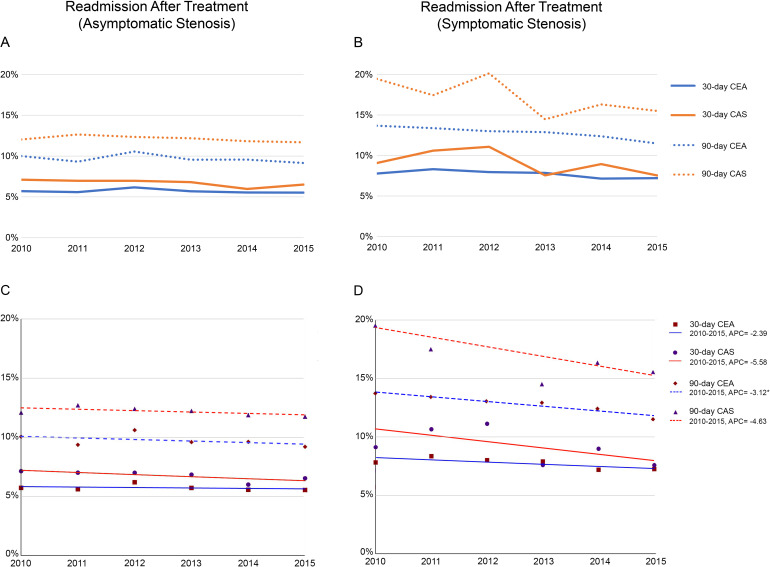 Figure 2. Trends in readmission rates (A, B) and APC (C, D) from 2010 to 2015 in asymptomatic and symptomatic patients. APC=annual percent change; CAS=carotid artery stenting; CEA=carotid… Source: Unplanned readmission after carotid stenting versus endarterectomy: analysis of the United States Nationwide Readmissions Database — Journal of Neurointerventional Surgery 2023; CC BY-NC.
Figure 2. Trends in readmission rates (A, B) and APC (C, D) from 2010 to 2015 in asymptomatic and symptomatic patients. APC=annual percent change; CAS=carotid artery stenting; CEA=carotid… Source: Unplanned readmission after carotid stenting versus endarterectomy: analysis of the United States Nationwide Readmissions Database — Journal of Neurointerventional Surgery 2023; CC BY-NC.
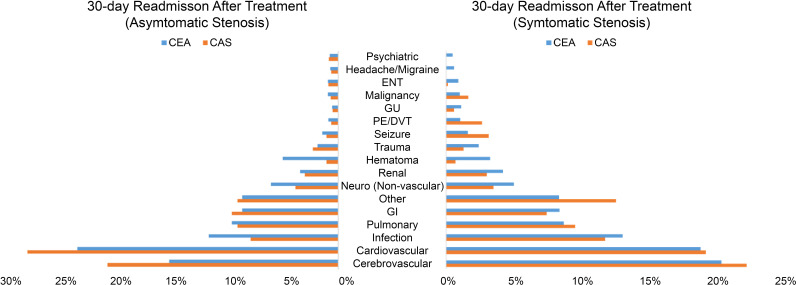 Figure 3. Grouped categories tabulating proportion of causes of readmission for asymptomatic stenosis (left) and symptomatic stenosis (right). CAS=carotid artery stenting; CEA=carotid… Source: Unplanned readmission after carotid stenting versus endarterectomy: analysis of the United States Nationwide Readmissions Database — Journal of Neurointerventional Surgery 2023; CC BY-NC.
Figure 3. Grouped categories tabulating proportion of causes of readmission for asymptomatic stenosis (left) and symptomatic stenosis (right). CAS=carotid artery stenting; CEA=carotid… Source: Unplanned readmission after carotid stenting versus endarterectomy: analysis of the United States Nationwide Readmissions Database — Journal of Neurointerventional Surgery 2023; CC BY-NC.
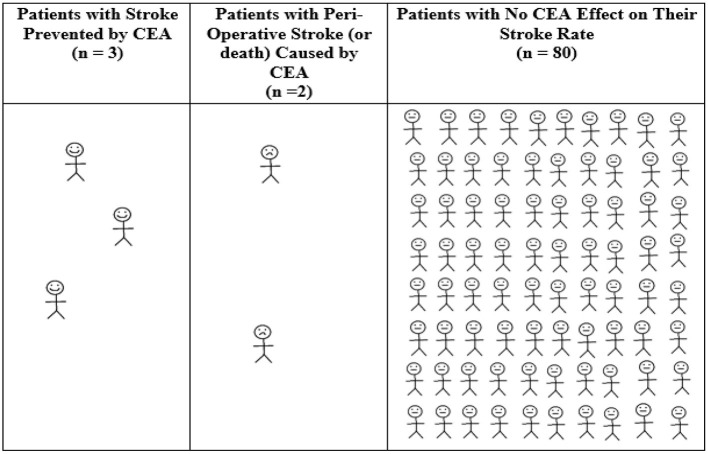 Figure 1. Average 12-month outcomes for every 85 patients with asymptomatic carotid stenosis randomized to CEA in ACAS (35). Calculated from ACAS data regarding patients with 60–99% asymptomatic… Source: Extra-Cranial Carotid Artery Stenosis: An Objective Analysis of the Available Evidence — Frontiers in Neurology 2022; CC BY.
Figure 1. Average 12-month outcomes for every 85 patients with asymptomatic carotid stenosis randomized to CEA in ACAS (35). Calculated from ACAS data regarding patients with 60–99% asymptomatic… Source: Extra-Cranial Carotid Artery Stenosis: An Objective Analysis of the Available Evidence — Frontiers in Neurology 2022; CC BY.
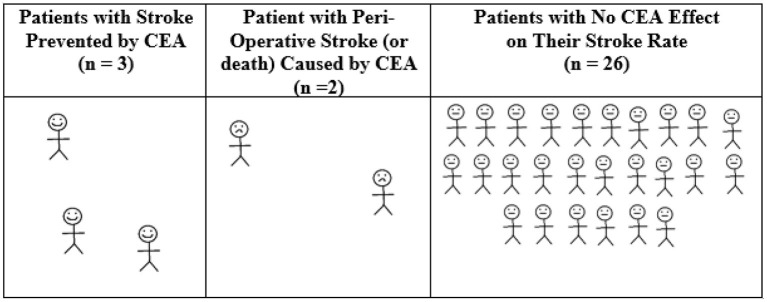 Figure 2. Average 12-month outcomes for every 31 symptomatic patients randomized to CEA in NASCET, ECST, and VACS. Calculated from pooled randomized trial data regarding symptomatic patients with… Source: Extra-Cranial Carotid Artery Stenosis: An Objective Analysis of the Available Evidence — Frontiers in Neurology 2022; CC BY.
Figure 2. Average 12-month outcomes for every 31 symptomatic patients randomized to CEA in NASCET, ECST, and VACS. Calculated from pooled randomized trial data regarding symptomatic patients with… Source: Extra-Cranial Carotid Artery Stenosis: An Objective Analysis of the Available Evidence — Frontiers in Neurology 2022; CC BY.
History of Present Illness
- Chief complaint: Symptomatic (TIA/amaurosis/minor stroke) or asymptomatic significant stenosis
- CAS indications (vs CEA): high cardiac/surgical risk, hostile neck (prior radiation, neck dissection, tracheostomy), restenosis after prior CEA, high carotid bifurcation, contralateral laryngeal nerve palsy
- Symptom timing, anatomy considerations
Past Medical History
- Cardiac disease (CAS may be favored if very high cardiac risk), antiplatelet response (dual antiplatelet required), contrast allergy, renal function
- Arch/access anatomy (tortuous/type III arch, heavy calcification → higher CAS risk), prior CEA/radiation
- Standard PMH
Imaging Review
CTA (arch to vertex) + Duplex (± DSA)
- Stenosis degree/morphology (heavy calcification, fresh thrombus/ulceration — higher embolic risk), aortic arch type and tortuosity (access feasibility/risk), bifurcation, intracranial circulation/collaterals
- Lesion length, distal landing zone for protection device
Labs
- CBC, BMP (renal), Coags, platelet function (dual antiplatelet efficacy), type and screen
Neurological Examination
- Focal exam, document baseline, NIHSS
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: biplane angio suite, radial/femoral access, full heparinization/reversal plan, stents/coils/liquid embolic or flow-diverter inventory, closure device, and bailout balloon/stent/aspiration tools.
- Special needs: antiplatelet status verified for stents/flow diverters, BP targets for rupture/ischemia/hyperperfusion risk, contrast/renal/allergy plan, ACT monitoring, and external ventricular drain/SAH pathway if ruptured.
- Immediate postop orders: neuro checks, access-site/pulse checks, BP parameters, antiplatelet/anticoagulation continuation, postop CT if neurologic change or rupture, flat time per closure, and follow-up vascular imaging plan.
Pre-procedure
- Dual antiplatelet therapy (aspirin + clopidogrel) started before the procedure (confirm responsiveness)
Revascularization Choice: CAS vs CEA vs TCAR
| Factor | CAS favored | CEA favored | TCAR / flow-reversal favored |
|---|---|---|---|
| Neck history | Prior radiation, radical neck dissection, restenosis after CEA, high bifurcation | Clean surgical neck, low cranial nerve risk | Hostile neck but anatomy suitable for direct carotid access |
| Arch/access | Simple arch, good femoral/radial access | Type III arch, bovine arch with tortuosity, severe arch atheroma | Poor transfemoral arch but accessible common carotid |
| Lesion | Smooth stenosis, adequate landing zones | Heavy circumferential calcification, fresh thrombus, very tortuous ICA | High embolic-risk lesion where flow reversal is feasible |
| Patient risk | High cardiac/pulmonary surgical risk | Older patient with high CAS stroke risk but acceptable surgical risk | High surgical-risk patient with anatomy favorable for TCAR |
| Antiplatelets | Can tolerate DAPT | Cannot tolerate DAPT | Can tolerate DAPT |
Pre-Procedure Readiness
- Confirm stenosis measurement method (NASCET-style distal ICA reference is standard for symptomatic carotid trials).
- Confirm symptom timing and infarct burden; large recent infarct, hemorrhagic conversion, or unstable neurologic status may change timing and BP goals.
- Review arch type, CCA/ICA tortuosity, plaque calcification, ulceration, thrombus, distal landing zone, and intracranial collaterals.
- Verify aspirin/P2Y12 loading and response if your practice uses platelet-function testing; document plan for clopidogrel nonresponse.
- Establish bailout medications and devices before crossing: atropine/glycopyrrolate, vasopressors, temporary pacing access if high risk, aspiration catheter, thrombectomy tools, covered stent, and reversal strategy.
Position / Setup
- Supine, angiography table, femoral (or radial/direct carotid) access, biplane DSA, heparinization
Key Procedure Steps
- Arterial access, heparinization; guide/sheath to the common carotid (navigate the arch carefully — embolic/stroke risk)
- Cross the stenosis with a wire (atraumatic)
- Deploy embolic protection device (distal filter beyond the lesion, or proximal/flow-reversal protection) — reduce distal embolization
- Pre-dilation angioplasty (if tight/calcified) — watch for bradycardia/hypotension (carotid baroreceptor — have atropine/glycopyrrolate, pacing ready)
- Deploy self-expanding carotid stent across the lesion
- Post-dilation angioplasty to appropriate diameter (avoid over-dilation — embolization)
- Retrieve embolic protection device, final angiography (residual stenosis, intracranial runs to exclude distal emboli)
- Access closure
Critical Anatomy & Structures at Risk
- Distal cerebral circulation — embolic stroke (arch navigation, lesion crossing, dilation) — protection device mitigates
- Carotid baroreceptor — bradycardia/hypotension/asystole (pre-medicate)
- Carotid wall (dissection, perforation), access vessels, hyperperfusion post-revascularization
Embolic Protection Choices
- Distal filter: familiar and preserves antegrade flow, but the lesion must be crossed before protection and filters can be difficult in tortuous distal ICA.
- Proximal balloon occlusion: protects before lesion crossing but requires flow arrest tolerance and careful aspiration before restoring flow.
- Flow reversal / TCAR-style protection: avoids arch manipulation and can protect before crossing, but needs suitable common carotid access and venous return setup.
- Choose protection based on arch risk, lesion morphology, distal ICA landing zone, circle of Willis/collaterals, and operator/device availability.
Intra-Procedure Rescue Plans
- Bradycardia/hypotension: stop balloon inflation, atropine/glycopyrrolate, vasopressor support, fluids, temporary pacing if refractory.
- Distal embolus or acute occlusion: intracranial angiographic run, aspiration/thrombectomy strategy, GP IIb/IIIa or antithrombotic rescue per protocol, and neurologic/anesthesia coordination.
- Dissection: maintain wire access, cover with additional stent if flow-limiting, avoid aggressive overdilation.
- No-reflow / spasm: distinguish embolus, spasm, dissection, and hyperperfusion physiology; treat with vasodilator only when appropriate.
- Hyperperfusion risk: aggressive post-stent BP control, especially severe pre-op stenosis with impaired autoregulation, contralateral occlusion, or chronic hypertension.
Equipment / Team
- Guide sheath/catheters, wires, embolic protection device, balloons, self-expanding carotid stent
- Atropine/glycopyrrolate, vasopressors, pacing (bradycardia), heparin, contrast
- Neurointervention/vascular team, anesthesia
Anesthesia
- Usually conscious sedation (awake neuro monitoring), arterial line, manage bradycardia/hypotension during dilation, BP control (hyperperfusion)
Potential Complications
- Embolic stroke (procedural — higher periprocedural stroke than CEA in some trials, esp. elderly/tortuous arch), distal embolization
- Bradycardia/hypotension/asystole (baroreceptor), access complications
- Hyperperfusion syndrome / hemorrhage, stent thrombosis (antiplatelet-dependent), restenosis, dissection, contrast nephropathy
Procedure Note Template
Preoperative Diagnosis: [Symptomatic/asymptomatic] [left/right] ICA stenosis ([__]%) with [high surgical risk / hostile neck / restenosis after CEA]
Postoperative Diagnosis: Same
Procedure: [Left/Right] carotid artery angioplasty and stenting with embolic protection
Operator / Assistant: Anesthesia: Conscious sedation (awake neuro monitoring) Access: [Right femoral/radial] sheath Contrast / Fluoro time: Devices: Embolic protection device, [balloon], self-expanding carotid stent; dual antiplatelet Complications: None
Indications: [Age]yo [M/F] with [symptomatic/asymptomatic] [__]% ICA stenosis and [high cardiac/surgical risk / hostile neck / post-CEA restenosis], favoring CAS over CEA. Dual antiplatelet confirmed. Risks (embolic stroke, bradycardia/hypotension, hyperperfusion) discussed.
Description of Procedure: After consent and time-out, conscious sedation with arterial access and heparinization was established. A guide sheath was navigated to the common carotid (careful arch navigation) and the stenosis crossed atraumatically. An embolic protection device was deployed distally. Pre-dilation angioplasty was performed (with atropine ready for bradycardia/hypotension), a self-expanding carotid stent deployed across the lesion, and post-dilation performed to an appropriate diameter. The protection device was retrieved.
Final angiography (including intracranial runs) showed satisfactory stent result without distal emboli. The access was closed.
The patient was transferred with strict BP control (hyperperfusion), telemetry (bradycardia), and continued dual antiplatelet (no interruption).
Post-Procedure Plan
- Step-down/ICU, neuro checks q1h, NIHSS, strict BP control (hyperperfusion/hemorrhage; also avoid hypotension)
- Continue dual antiplatelet (do not interrupt — stent thrombosis), access/pulse checks
- Telemetry (bradycardia), hydration (contrast)
- Watch hyperperfusion syndrome (headache/seizure/deficit), carotid duplex follow-up (restenosis), risk factor modification
Follow-Up and Surveillance
- First 24 hours: NIHSS/neuro checks, access-site exam, telemetry, BP ceiling/floor orders, renal/contrast monitoring, and explicit DAPT continuation.
- Early danger signs: ipsilateral headache, seizure, focal deficit, confusion, or severe hypertension after revascularization should trigger hyperperfusion/ICH evaluation.
- Duplex surveillance: establish a post-stent baseline, then repeat per local protocol; in-stent velocities can differ from native ICA thresholds.
- Secondary prevention: statin intensity, smoking cessation, diabetes/BP control, sleep apnea management, and antiplatelet duration documented before discharge.
- If DAPT must be interrupted for another procedure, discuss with the stenting team first; early interruption risks acute stent thrombosis.
Chief-Level Case Review
Use these as the senior-level mental model for Carotid Artery Angioplasty and Stenting (CAS):
- Decision point: The operation is won or lost on control: identify inflow, outflow, perforators, collateral options, and the fastest route to temporary control before exposing the lesion itself.
- Technical lever: Do not accept a cosmetic result over physiology: ICG/Doppler/DSA, branch patency, perforator preservation, and parent-vessel caliber matter more than how the clip or resection bed looks.
- Bailout: Have a rupture or ischemia script ready: lower pressure, suction strategy, temporary occlusion time, heparin/reversal plan, bypass/reconstruction threshold, and postop BP targets.
- Postop watch: Postop danger is delayed: vasospasm, thromboembolism, hyperperfusion, hemorrhage, edema, hydrocephalus, and seizure plans need explicit orders.
Common Pimp Questions
Use these to pressure-test preparation for Carotid Artery Angioplasty and Stenting (CAS):
- What is the proximal-control plan before the lesion is manipulated?
- Which branch, perforator, or venous structure is most likely to be injured in this exposure?
- What are the intraoperative rupture steps, including temporary clip, suction, BP, and backup clip strategy?
- What confirms treatment success: ICG, Doppler, puncture/deflation, DSA, or postoperative CTA?
- What postoperative BP, vasospasm, antiplatelet, or anticoagulation issue changes the orders tonight?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Preferred approach side, sylvian split style, and cisternal-opening sequence: [attending-specific]
- Temporary clip threshold, burst-suppression preference, and BP during occlusion: [attending-specific]
- Clip manufacturer/shape sequence and whether Doppler, ICG, puncture, or intraop DSA is routine: [attending-specific]
- Antiplatelet/anticoagulation reversal and restart timing: [attending-specific]