
Case Prep: AVM / dAVF Endovascular Embolization
Case / Approach Snapshot
- Anatomy at risk: access vessels, arch/cervical anatomy, parent artery branches, perforators, collateral pathways, venous drainage when relevant, and device landing zones.
- Operative steps: confirm indication and imaging, obtain access safely, navigate with roadmap control, deploy the planned device or embolic strategy, document final angiography, and define antiplatelet/anticoagulation and postprocedure monitoring; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: access complication, dissection/perforation, thromboembolism, device malposition or migration, hemorrhage, vasospasm, antiplatelet failure, and conversion to open or staged management.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [brain AVM (Spetzler-Martin grade) / dural AV fistula] planned for endovascular embolization [as preoperative adjunct / pre-radiosurgery / curative / palliative].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · neuroangio.org · Radiopaedia · PubMed Central — figures © linked; see media-sources.md
High-Yield Literature
- Transvenous embolization of brain arteriovenous malformations: a review of techniques, indications, and outcomes — Chen CJ. Neurosurgical focus 2018. PubMed
- Role of endovascular embolization for trigeminal neuralgia related to cerebral vascular malformation — Ge H. Interventional neuroradiology : journal of peritherapeutic neuroradiology, surgical procedures and related neurosciences 2016. PubMed
- Cerebral abscess after neuro-vascular embolization: Own experience and review of the literature — Cossu G. Acta neurochirurgica 2017. PubMed
- Pediatric intracranial arteriovenous shunts: Advances in diagnosis and treatment — Lv X. European journal of paediatric neurology : EJPN : official journal of the European Paediatric Neurology Society 2020. PubMed
- Simulation of superselective catheterization for cerebrovascular lesions using a virtual injection software — Sundararajan SH. CVIR endovascular 2021. PubMed
- Clinical importance of the occipital artery in vascular lesions: A review of the literature — Guo Y. The neuroradiology journal 2019. PubMed
- Long-term angiographic results of endovascularly “cured” intracranial dural arteriovenous fistulas — Ambekar S. Journal of neurosurgery 2016. PubMed
- Radiation exposure in the endovascular therapy of cranial and spinal dural arteriovenous fistula in the last decade: a retrospective, single-center observational study — Opitz M. Neuroradiology 2022. PubMed
- The impact of software-based metal artifact reduction on the liquid embolic agent Onyx in cone-beam CT: a systematic in vitro and in vivo study — Schmitt N. Journal of neurointerventional surgery 2022. PubMed
- Treatment Strategy of a Patient With a Brain Arteriovenous Malformation and Cranial Dural Fistula: 2-Dimensional Operative Video — Sattur MG. Operative neurosurgery (Hagerstown, Md.) 2019. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
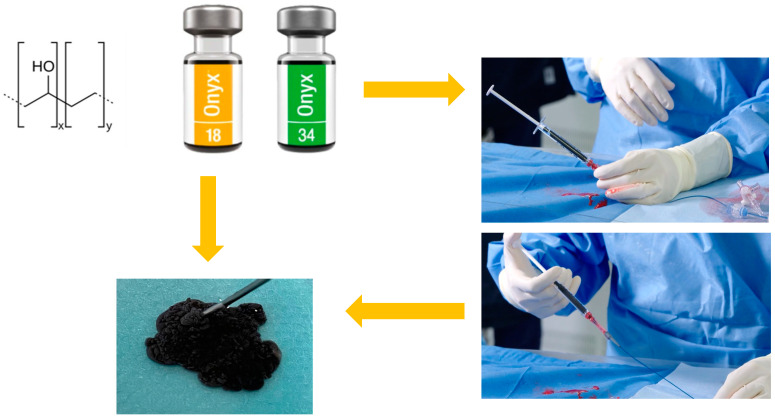 Figure 1. Graphical representation of the chemical formula, macroscopic appearance and material for the injection of OnyxTMgel. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
Figure 1. Graphical representation of the chemical formula, macroscopic appearance and material for the injection of OnyxTMgel. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
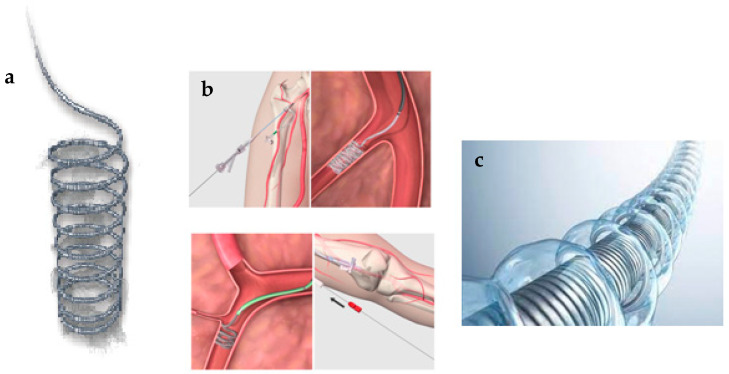 Figure 2. Coil bare (a), coil endovascular application (b), hydrogel-coated coil (c) for embolisation. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
Figure 2. Coil bare (a), coil endovascular application (b), hydrogel-coated coil (c) for embolisation. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
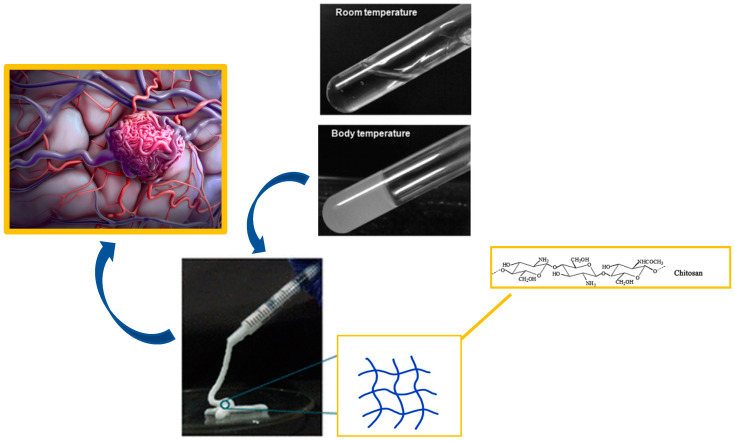 Figure 3. Chitosan hydrogel as embolic agent for embolisation process. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
Figure 3. Chitosan hydrogel as embolic agent for embolisation process. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
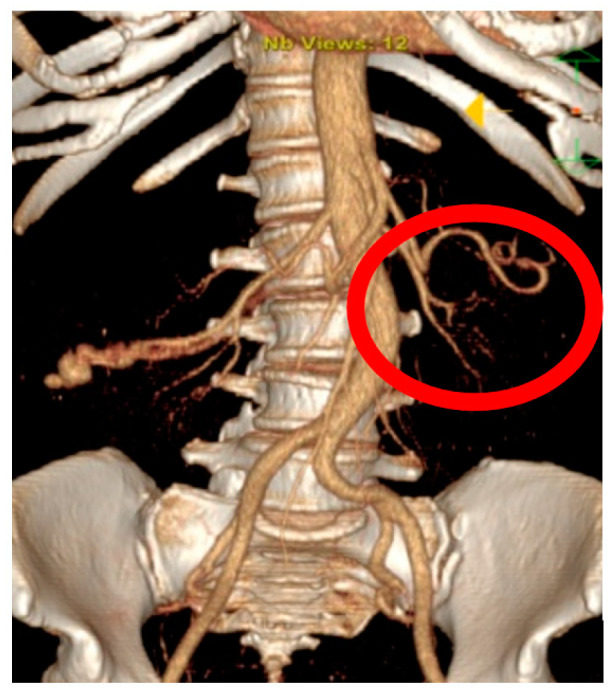 Figure A1. Pre-operative 3DMPR CT reconstruction. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
Figure A1. Pre-operative 3DMPR CT reconstruction. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
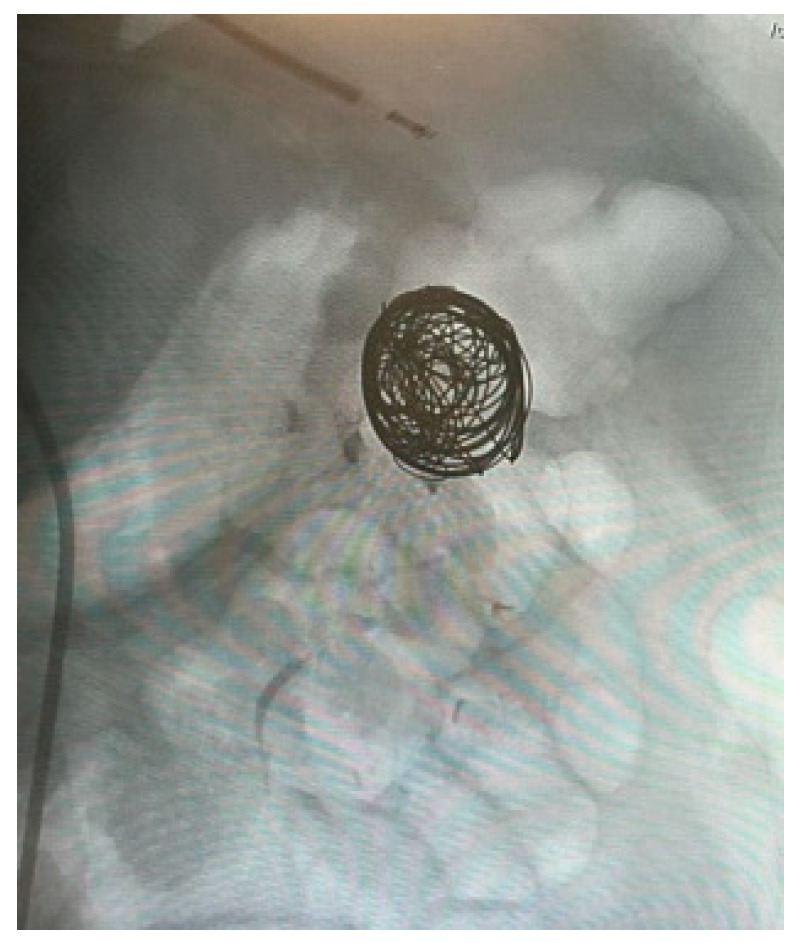 Figure A1. Pre-operative 3DMPR CT reconstruction. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
Figure A1. Pre-operative 3DMPR CT reconstruction. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
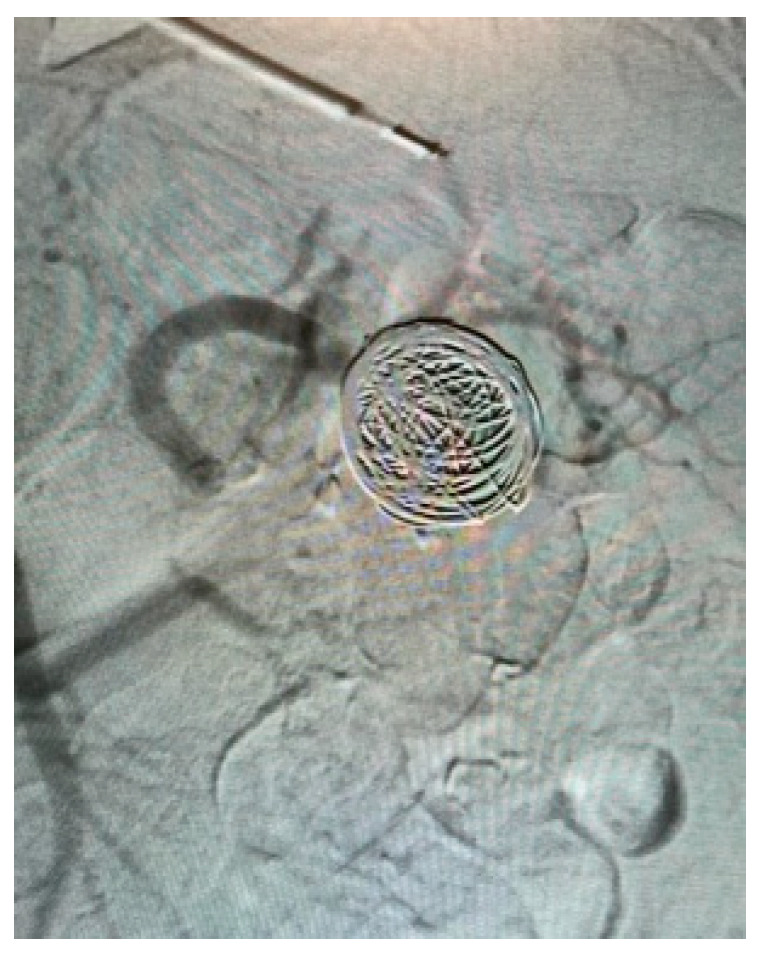 Figure A1. Pre-operative 3DMPR CT reconstruction. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
Figure A1. Pre-operative 3DMPR CT reconstruction. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
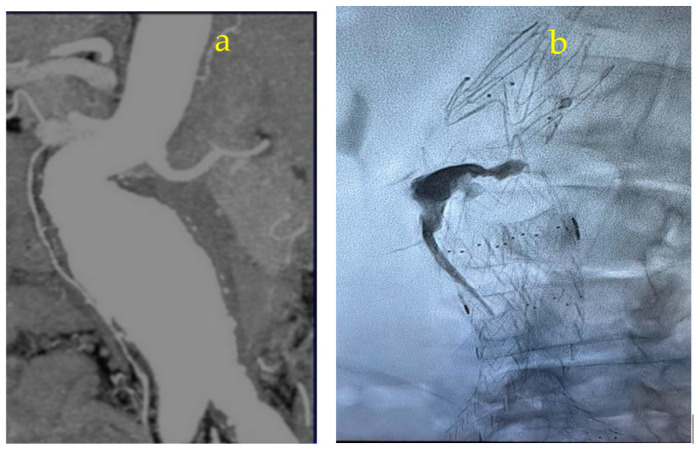 Figure A1. Pre-operative 3DMPR CT reconstruction. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
Figure A1. Pre-operative 3DMPR CT reconstruction. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
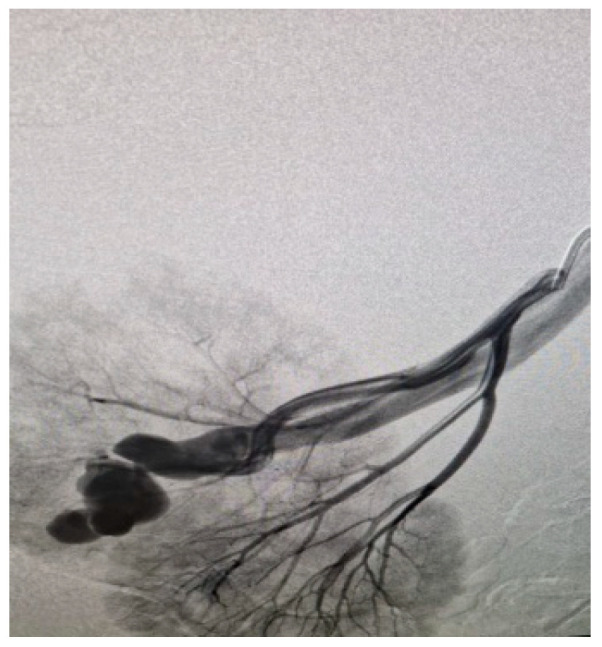 Figure A2. Intraoperative diagnostic angiography. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
Figure A2. Intraoperative diagnostic angiography. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
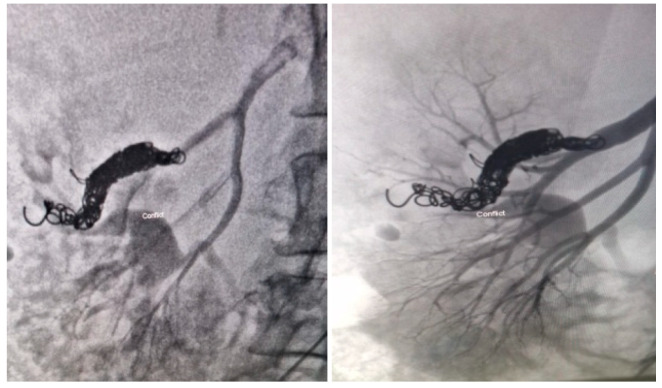 Figure A3. Angiographic control post-coil release. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
Figure A3. Angiographic control post-coil release. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
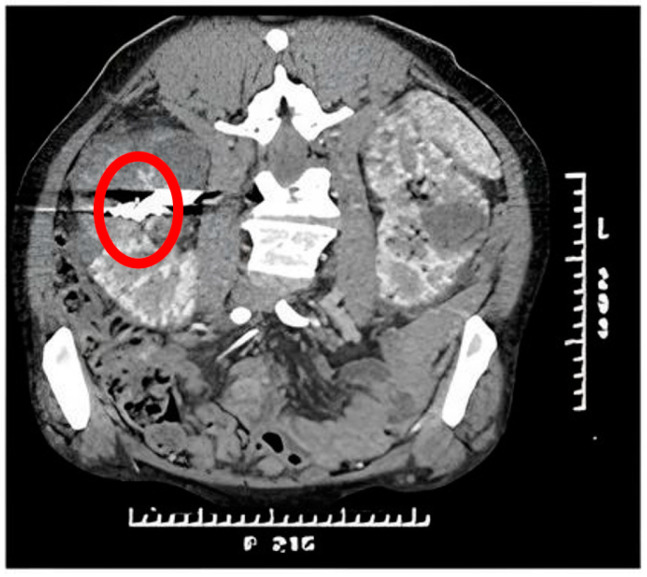 Figure A4. Control CT scan with contrast medium at 30 days with evidence of coils on release and absence of AVM. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
Figure A4. Control CT scan with contrast medium at 30 days with evidence of coils on release and absence of AVM. Source: OnyxTMGel or Coil versus Hydrogel as Embolic Agents in Endovascular Applications: Review of the Literature and Case Series — Gels 2024; CC BY.
History of Present Illness
- Chief complaint: Hemorrhage, seizures, headache, progressive deficit, or pulsatile tinnitus/bruit (dAVF)
- Embolization role: preoperative (reduce flow/deep feeders before resection), pre-SRS (volume reduction — debated), curative (selected small AVMs, many dAVFs), palliative (high-grade, symptom-targeted)
- Prior hemorrhage, prior treatment, planned multimodal strategy
Past Medical History
- Contrast allergy, renal function, bleeding/clotting, vascular access
- Standard PMH
Imaging Review
DSA (gold standard) + MRI/CTA
- Angioarchitecture: feeding arteries, nidus, draining veins, flow, associated aneurysms (flow-related/intranidal — bleeding risk), venous outflow stenosis
- Spetzler-Martin grade (AVM); dAVF: Borden/Cognard classification (cortical venous reflux = high risk), fistula site
- Identify en passage vessels and dangerous anastomoses (e.g., ECA-ICA/vertebral collaterals, supply to cranial nerves) — avoid non-target embolization
Labs
- CBC, BMP (renal), Coags, type and screen
Neurological Examination
- Focal exam per AVM location, cranial nerves (dAVF/skull base), document baseline
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: biplane angio suite, radial/femoral access, full heparinization/reversal plan, stents/coils/liquid embolic or flow-diverter inventory, closure device, and bailout balloon/stent/aspiration tools.
- Special needs: antiplatelet status verified for stents/flow diverters, BP targets for rupture/ischemia/hyperperfusion risk, contrast/renal/allergy plan, ACT monitoring, and external ventricular drain/SAH pathway if ruptured.
- Immediate postop orders: neuro checks, access-site/pulse checks, BP parameters, antiplatelet/anticoagulation continuation, postop CT if neurologic change or rupture, flat time per closure, and follow-up vascular imaging plan.
Strategy & Agents
- Liquid embolics: Onyx (EVOH) (controlled, cohesive — workhorse), n-BCA glue (cyanoacrylate); coils (high-flow fistulas, venous side of dAVF); particles (palliative/preop, temporary)
- Approach: transarterial (most) or transvenous (selected dAVF — occlude the recipient venous pouch)
- Staged embolization for large AVMs (avoid normal perfusion pressure breakthrough)
Endpoint Selection
- Preoperative AVM embolization: target deep feeders, flow-related aneurysms, high-flow shunts, and surgically inaccessible pedicles; do not embolize superficial feeders that the surgeon needs for intraoperative orientation unless planned.
- Curative AVM embolization: only for selected small compact nidi with safe pedicles and venous anatomy; final cure requires complete nidus obliteration without premature venous occlusion.
- dAVF embolization: the endpoint is occlusion of the fistulous point and proximal pathologic venous recipient, especially cortical venous reflux; feeder reduction alone is not cure.
- Palliative embolization: treat a specific risk/symptom such as venous hypertension, flow aneurysm, steal, or high-output shunt; document what remains.
- Staged embolization: limit flow/pressure shifts per session and define the next treatment before leaving the angio suite.
Position / Setup
- Supine, angiography table, femoral/radial access, biplane DSA, heparinization
Key Procedure Steps
- Arterial access, guide catheter to feeding pedicle territory
- Microcatheter navigated into the feeding artery/nidus (or transvenous to the fistula/draining vein for dAVF)
- Provocative testing (selected — e.g., amytal/lidocaine to test for eloquent supply before embolizing) in awake or with monitoring
- Inject liquid embolic (Onyx/glue) under continuous fluoroscopy with controlled reflux, penetrating the nidus/fistula; avoid premature venous occlusion (AVM) or non-target/dangerous-anastomosis embolization
- dAVF: occlude the fistulous point / proximal draining vein (transvenous coiling/Onyx) — eliminate cortical venous reflux
- Sequential pedicles/stages; final angiography (degree of nidus/fistula obliteration, preserved normal vessels)
- Access closure
Critical Anatomy & Structures at Risk
- Normal brain arteries / en passage vessels — non-target embolization → stroke
- Draining vein (AVM) — premature venous occlusion → nidus rupture/hemorrhage
- Dangerous anastomoses (ECA-to-ICA/vertebral, cranial nerve supply) — non-target embolization → stroke/cranial neuropathy
- Catheter retention (glued/retained microcatheter)
Equipment / Team
- Neuroangiography suite, guide/microcatheters (DMSO-compatible for Onyx), microwires
- Onyx / n-BCA glue / coils / particles, DMSO, heparin
- Neurointerventional team, anesthesia
Anesthesia
- General (or awake for provocative testing in eloquent territory), heparinization, BP control
Potential Complications
- Hemorrhage (vessel/nidus perforation, premature venous occlusion, post-embolization NPPB) — BP control, reversal
- Ischemic stroke / cranial neuropathy (non-target/reflux embolization, dangerous anastomoses)
- Retained/glued microcatheter, incomplete obliteration (multimodal plan), access complications, contrast nephropathy
Rescue Plans
- Reflux toward normal branch/en-passage vessel: stop injection, wait for plug control, reposition or abandon that pedicle; do not “push through” reflux.
- Microcatheter stuck in Onyx/glue cast: follow device-specific detachment/traction limits, consider leaving a retained catheter segment rather than avulsing a feeder or nidus.
- Perforation/rupture: stop embolic, reverse anticoagulation as appropriate, lower BP, tamponade with balloon/embolization if possible, obtain CT, and coordinate emergent surgery/EVD.
- Premature venous occlusion: stop; assess nidus drainage and hemorrhage risk, maintain strict BP control, and do not continue arterial filling into a trapped nidus.
- Cranial neuropathy risk through ECA supply: stop if dangerous anastomoses or vasa nervorum supply is seen; facial/ophthalmic/petrous collaterals are not optional details.
Procedure Note Template
Preoperative Diagnosis: [Brain AVM (Spetzler-Martin __) / dural AV fistula (Borden/Cognard __)]
Postoperative Diagnosis: Same
Procedure: Endovascular embolization of [brain AVM / dAVF] — [transarterial/transvenous], [Onyx/glue/coils], [N] pedicles
Operator / Assistant: Anesthesia: General [or awake for provocative testing] Access: [Right femoral/radial] arterial sheath Contrast / Fluoro time / EBL: Devices: [Onyx/n-BCA/coils — volumes], heparin Complications: None
Indications: [Age]yo [M/F] with a [brain AVM/dAVF] presenting with [hemorrhage/seizures/tinnitus]; embolization performed as [preoperative adjunct / pre-SRS / curative / palliative]. Risks (hemorrhage, non-target embolization/stroke, cranial neuropathy) discussed.
Description of Procedure: After consent and time-out, [general anesthesia] and arterial access with heparinization were established. A guide catheter was positioned and a microcatheter navigated into the [feeding pedicle / fistulous point]. [Provocative testing was performed before embolization in eloquent territory.] Liquid embolic [Onyx/glue] was injected under continuous fluoroscopy with controlled reflux, penetrating the [nidus/fistula], avoiding premature venous occlusion and dangerous anastomoses; [the dAVF draining vein/fistulous point was occluded transvenously with coils/Onyx]. [N] pedicles were treated over [N] stages.
Final angiography showed [__]% obliteration with preserved normal vessels and draining vein [until the appropriate endpoint]. Catheters were removed and the access closed.
The patient was transferred to the NSICU with strict BP control; [the next stage of the multimodal plan was scheduled].
Post-Procedure Plan
- NSICU, neuro checks q1h, strict BP control (post-embolization hemorrhage/NPPB risk), access checks
- Coordinate next stage of multimodal plan (surgery — often within days; SRS; further embolization stages)
- Hydration (contrast), CT if neuro change
- Follow-up DSA (obliteration; for definitive embolization confirm cure), surveillance
Chief-Level Case Review
Use these as the senior-level mental model for AVM / dAVF Endovascular Embolization:
- Decision point: The operation is won or lost on control: identify inflow, outflow, perforators, collateral options, and the fastest route to temporary control before exposing the lesion itself.
- Technical lever: Do not accept a cosmetic result over physiology: ICG/Doppler/DSA, branch patency, perforator preservation, and parent-vessel caliber matter more than how the clip or resection bed looks.
- Bailout: Have a rupture or ischemia script ready: lower pressure, suction strategy, temporary occlusion time, heparin/reversal plan, bypass/reconstruction threshold, and postop BP targets.
- Postop watch: Postop danger is delayed: vasospasm, thromboembolism, hyperperfusion, hemorrhage, edema, hydrocephalus, and seizure plans need explicit orders.
Common Pimp Questions
Use these to pressure-test preparation for AVM / dAVF Endovascular Embolization:
- What is the proximal-control plan before the lesion is manipulated?
- Which branch, perforator, or venous structure is most likely to be injured in this exposure?
- What are the intraoperative rupture steps, including temporary clip, suction, BP, and backup clip strategy?
- What confirms treatment success: ICG, Doppler, puncture/deflation, DSA, or postoperative CTA?
- What postoperative BP, vasospasm, antiplatelet, or anticoagulation issue changes the orders tonight?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Preferred approach side, sylvian split style, and cisternal-opening sequence: [attending-specific]
- Temporary clip threshold, burst-suppression preference, and BP during occlusion: [attending-specific]
- Clip manufacturer/shape sequence and whether Doppler, ICG, puncture, or intraop DSA is routine: [attending-specific]
- Antiplatelet/anticoagulation reversal and restart timing: [attending-specific]