
Case Prep: Decompressive Hemicraniectomy for Malignant MCA Infarction
Case / Approach Snapshot
- Anatomy at risk: parent vessels, perforators, branch ostia, collateral circulation, venous drainage, cranial nerves, cisterns, and eloquent territories threatened by temporary occlusion or retraction.
- Operative steps: plan proximal and distal control, expose the corridor, obtain cerebrospinal fluid/brain relaxation, identify parent vessels before the lesion, treat the lesion/device target, and confirm flow and hemostasis before closure; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: intraoperative rupture, thromboembolism, branch or perforator compromise, vasospasm, inadequate proximal control, bypass or reconstructive options, anticoagulation/reversal, and postoperative surveillance.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with malignant [left/right] MCA territory infarction with [progressive edema / midline shift / declining consciousness] planned for decompressive hemicraniectomy.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
External sources — operative figures/atlases are copyrighted (linked, not copied). See media-sources.md.
Operative technique & approach
- The Neurosurgical Atlas — search “decompressive hemicraniectomy” (technique + flap size)
Imaging
Open-access figures
High-Yield Literature
- Decompressive Hemicraniectomy in the Treatment of Malignant Middle Cerebral Artery Infarction: A Meta-Analysis — Das S. World neurosurgery 2019. PubMed
- Decompressive Surgery for the Treatment of Malignant Infarction of the Middle Cerebral Artery (DESTINY): a randomized, controlled trial — Jüttler E. Stroke 2007. PubMed
- It is all about timing: decompressive hemicraniectomy for malignant middle-cerebral-artery infarction — Macha K. Arquivos de neuro-psiquiatria 2023. PubMed
- Decompressive hemicraniectomy after malignant middle cerebral artery infarction: does hospital of origin matter? — Smyth D. Internal medicine journal 2018. PubMed
- Decompressive hemicraniectomy versus medical treatment of malignant middle cerebral artery infarction: a systematic review and meta-analysis — Wei H. Bioscience reports 2020. PubMed
- Decompressive hemicraniectomy in patients with malignant middle cerebral artery infarction: A real-world study — Pilato F. Journal of the neurological sciences 2022. PubMed
- Surgical decompression for space-occupying cerebral infarction (the Hemicraniectomy After Middle Cerebral Artery infarction with Life-threatening Edema Trial [HAMLET]): a multicentre, open, randomised trial — Hofmeijer J. The Lancet. Neurology 2009. PubMed
- Decompressive hemicraniectomy in patients with malignant middle cerebral artery infarction: A systematic review and meta-analysis — Yang MH. The surgeon : journal of the Royal Colleges of Surgeons of Edinburgh and Ireland 2015. PubMed
- Decompressive hemicraniectomy for malignant middle cerebral artery infarction: an update — Subramaniam S. The neurologist 2009. PubMed
- Long-term outcome after decompressive hemicraniectomy for malignant middle cerebral artery infarction — Berger N. Journal of neurology 2023. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
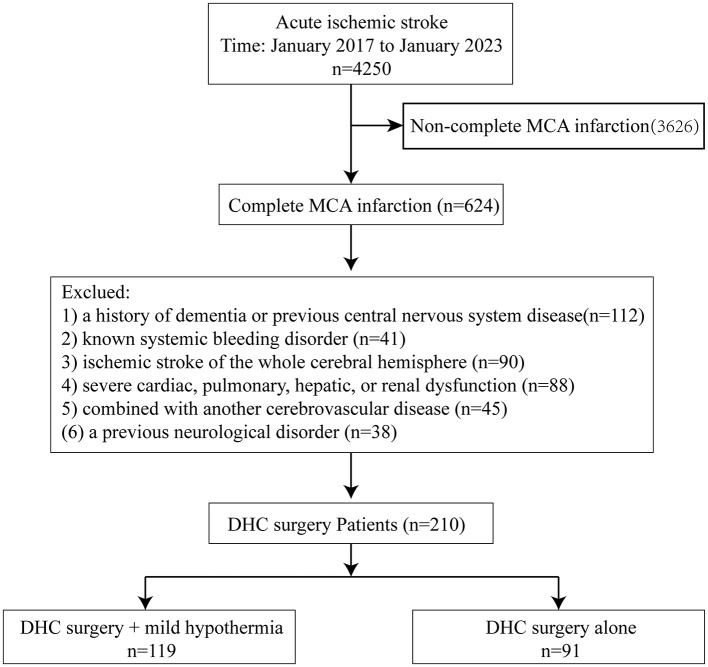 Figure 1. Trial profile. Source: Early decompressive hemicraniectomy combined with mild hypothermia treatment for malignant middle cerebral artery infarction — Frontiers in Neurology 2026; CC BY.
Figure 1. Trial profile. Source: Early decompressive hemicraniectomy combined with mild hypothermia treatment for malignant middle cerebral artery infarction — Frontiers in Neurology 2026; CC BY.
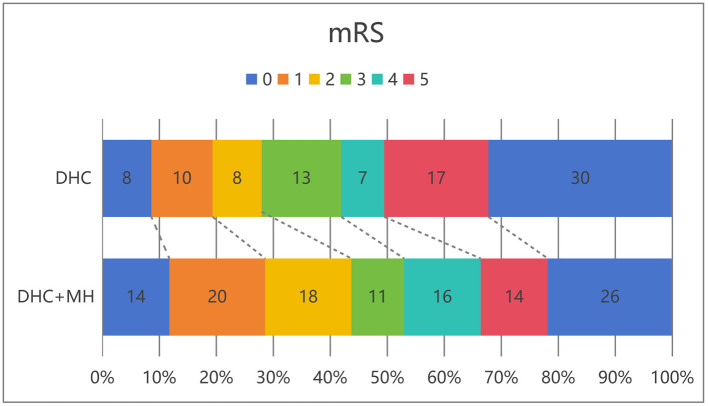 Figure 2. Distribution of 6-month modified Rankin scale scores in patients receiving DHC alone vs. those receiving DHC combined with mild hypothermia. Source: Early decompressive hemicraniectomy combined with mild hypothermia treatment for malignant middle cerebral artery infarction — Frontiers in Neurology 2026; CC BY.
Figure 2. Distribution of 6-month modified Rankin scale scores in patients receiving DHC alone vs. those receiving DHC combined with mild hypothermia. Source: Early decompressive hemicraniectomy combined with mild hypothermia treatment for malignant middle cerebral artery infarction — Frontiers in Neurology 2026; CC BY.
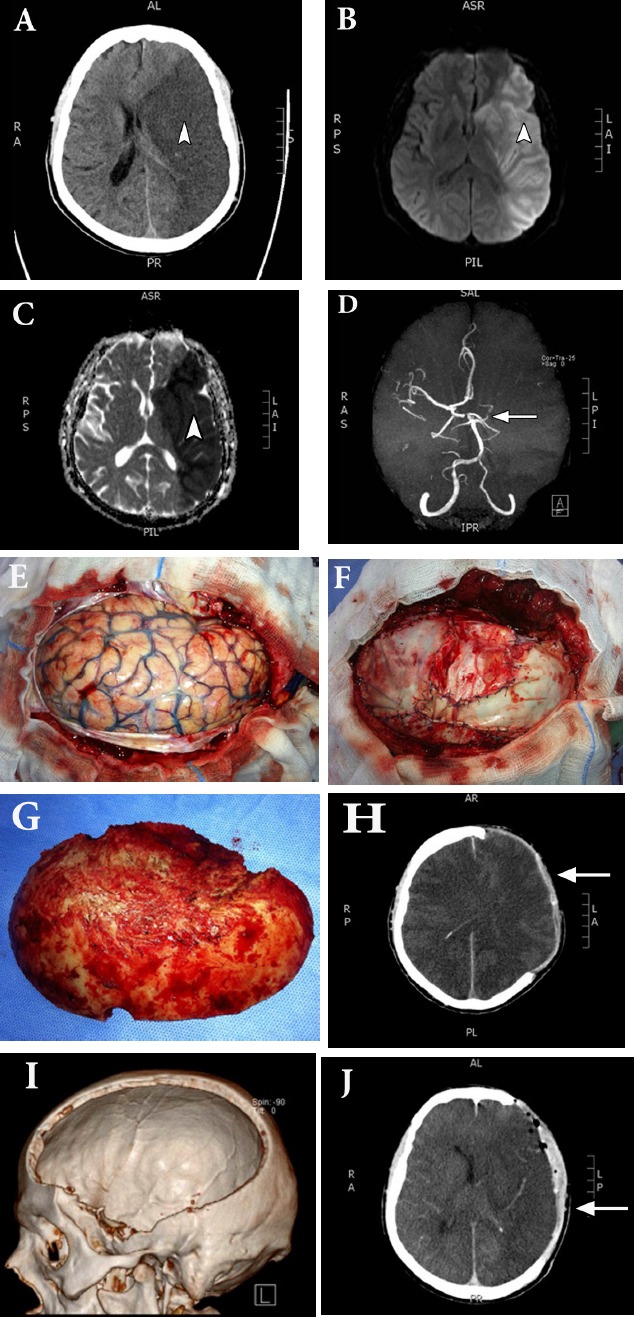 Figure 1. Case illustration of a 39-year-old male (case 4) who presented with left massive MCA infarction demonstrated on A) plain CT scan which was delineated by MRI diffusion B) and ADC scan C)… Source: Decompressive hemicraniectomy for malignant middle cerebral artery infarction — Neurosciences 2017; CC BY.
Figure 1. Case illustration of a 39-year-old male (case 4) who presented with left massive MCA infarction demonstrated on A) plain CT scan which was delineated by MRI diffusion B) and ADC scan C)… Source: Decompressive hemicraniectomy for malignant middle cerebral artery infarction — Neurosciences 2017; CC BY.
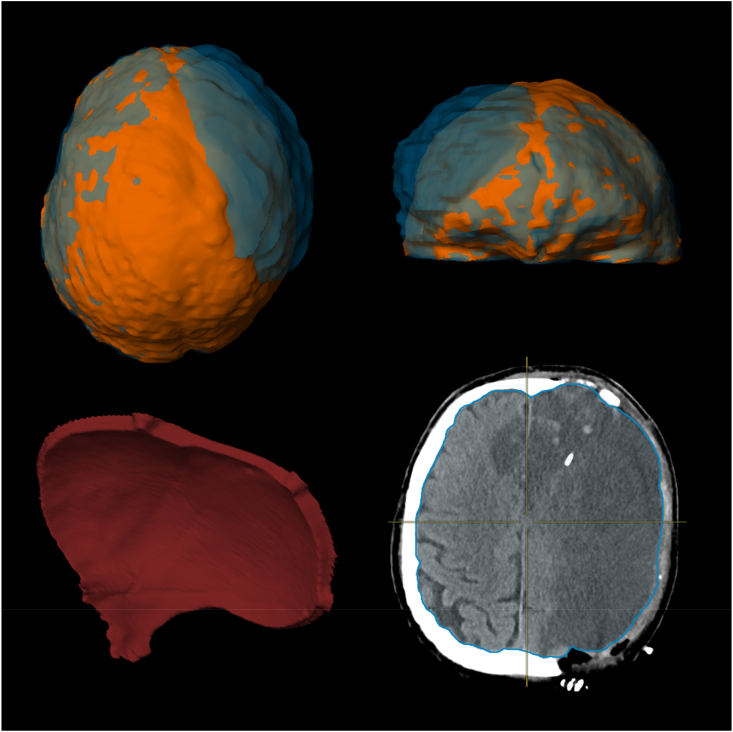 Fig. 1. (clockwise from top left) overhead view of a 3D-rendered fully segmented brain before (orange) and after (blue) decompressive hemicraniectomy (DCE); front view of a 3D-rendered fully… Source: How much space is needed for decompressive surgery in malignant middle cerebral artery infarction: Enabling single-stage surgery — Brain & Spine 2023; CC BY-NC-ND.
Fig. 1. (clockwise from top left) overhead view of a 3D-rendered fully segmented brain before (orange) and after (blue) decompressive hemicraniectomy (DCE); front view of a 3D-rendered fully… Source: How much space is needed for decompressive surgery in malignant middle cerebral artery infarction: Enabling single-stage surgery — Brain & Spine 2023; CC BY-NC-ND.
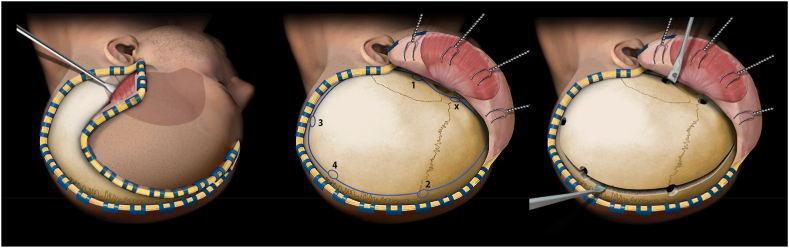 Fig. 2. Schematic representation of the main surgical steps of a decompressive hemicraniectomy as described by Raabe et al. (Raabe, 2019) Dural incision after bony decompression is not shown…. Source: How much space is needed for decompressive surgery in malignant middle cerebral artery infarction: Enabling single-stage surgery — Brain & Spine 2023; CC BY-NC-ND.
Fig. 2. Schematic representation of the main surgical steps of a decompressive hemicraniectomy as described by Raabe et al. (Raabe, 2019) Dural incision after bony decompression is not shown…. Source: How much space is needed for decompressive surgery in malignant middle cerebral artery infarction: Enabling single-stage surgery — Brain & Spine 2023; CC BY-NC-ND.
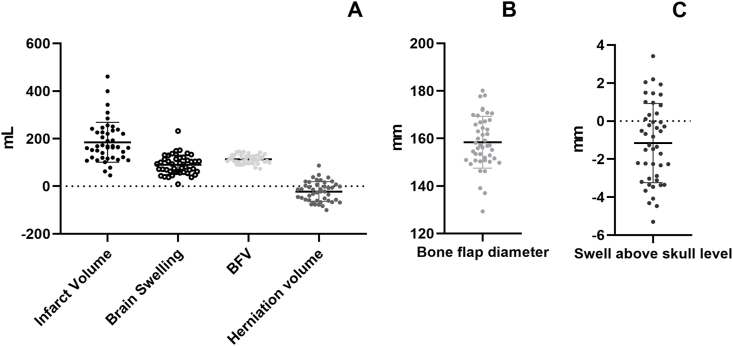 Fig. 4. A.Distribution of the different measured volumes in mL,B.the distribution of bone flap diameters, andC.the modeled swelling above the previous outer skull rim after decompressive… Source: How much space is needed for decompressive surgery in malignant middle cerebral artery infarction: Enabling single-stage surgery — Brain & Spine 2023; CC BY-NC-ND.
Fig. 4. A.Distribution of the different measured volumes in mL,B.the distribution of bone flap diameters, andC.the modeled swelling above the previous outer skull rim after decompressive… Source: How much space is needed for decompressive surgery in malignant middle cerebral artery infarction: Enabling single-stage surgery — Brain & Spine 2023; CC BY-NC-ND.
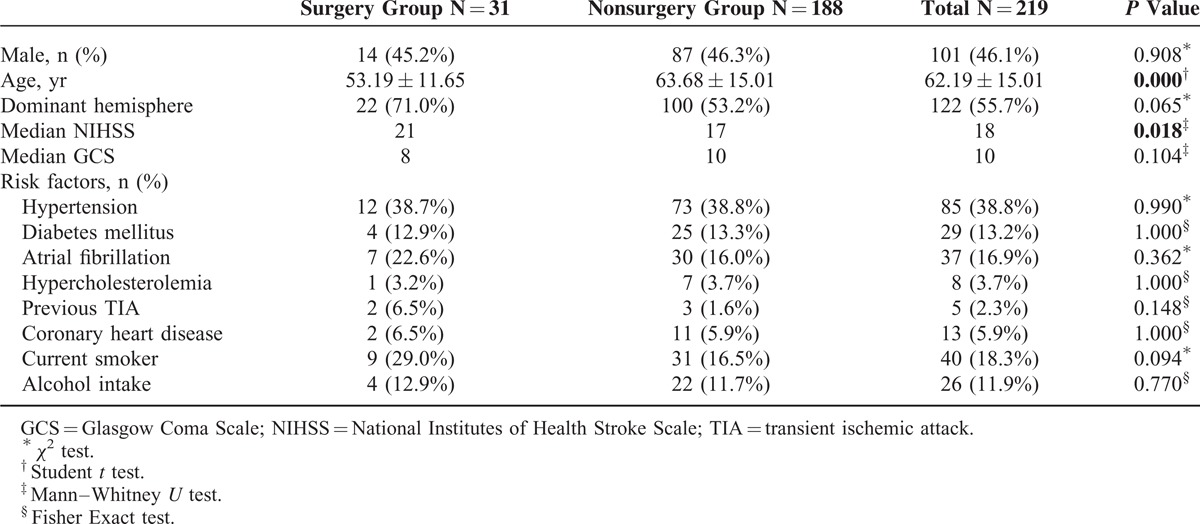 Figure 8. Source: A Cohort Study of Decompressive Craniectomy for Malignant Middle Cerebral Artery Infarction: A Real-World Experience in Clinical Practice — Medicine (Baltimore). 2015 Jun 26;94(25):e1039. doi: 10.1097/MD.0000000000001039; CC BY-NC-ND.
Figure 8. Source: A Cohort Study of Decompressive Craniectomy for Malignant Middle Cerebral Artery Infarction: A Real-World Experience in Clinical Practice — Medicine (Baltimore). 2015 Jun 26;94(25):e1039. doi: 10.1097/MD.0000000000001039; CC BY-NC-ND.
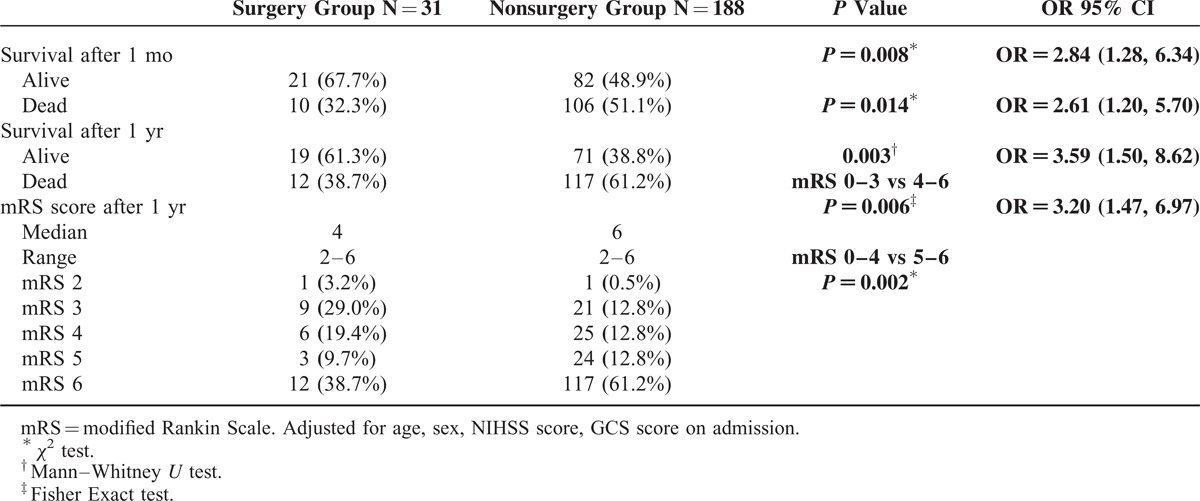 Figure 9. Source: A Cohort Study of Decompressive Craniectomy for Malignant Middle Cerebral Artery Infarction: A Real-World Experience in Clinical Practice — Medicine (Baltimore). 2015 Jun 26;94(25):e1039. doi: 10.1097/MD.0000000000001039; CC BY-NC-ND.
Figure 9. Source: A Cohort Study of Decompressive Craniectomy for Malignant Middle Cerebral Artery Infarction: A Real-World Experience in Clinical Practice — Medicine (Baltimore). 2015 Jun 26;94(25):e1039. doi: 10.1097/MD.0000000000001039; CC BY-NC-ND.
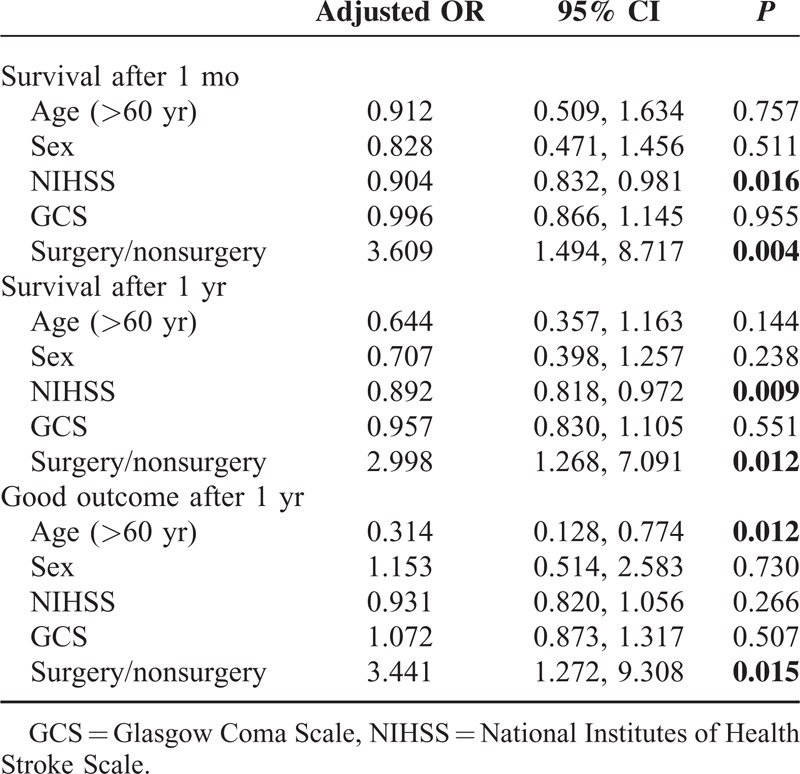 Figure 10. Source: A Cohort Study of Decompressive Craniectomy for Malignant Middle Cerebral Artery Infarction: A Real-World Experience in Clinical Practice — Medicine (Baltimore). 2015 Jun 26;94(25):e1039. doi: 10.1097/MD.0000000000001039; CC BY-NC-ND.
Figure 10. Source: A Cohort Study of Decompressive Craniectomy for Malignant Middle Cerebral Artery Infarction: A Real-World Experience in Clinical Practice — Medicine (Baltimore). 2015 Jun 26;94(25):e1039. doi: 10.1097/MD.0000000000001039; CC BY-NC-ND.
History of Present Illness
- Chief complaint: Large MCA stroke with deteriorating consciousness
- Stroke onset time; tPA/thrombectomy given?
- Progression: declining GCS, anisocoria, worsening edema on serial CT
- Evidence-based: DESTINY, DECIMAL, HAMLET trials — decompression within 48h reduces mortality in malignant MCA infarction, especially age < 60
- Premorbid functional status, goals of care (decompression survivors often have significant disability — counsel family)
Imaging Review
CT Head
- MCA territory infarct (> 50% MCA territory, or > 145 cm³ on DWI)
- Cytotoxic edema, sulcal effacement
- Midline shift, uncal herniation, basal cistern effacement
- Hemorrhagic transformation
- Involvement of ACA/PCA territory
Labs
- CBC, BMP, Coags (especially if post-tPA/thrombectomy — correct coagulopathy)
- Type and screen
Neurological Examination
- GCS, pupils, motor (dense contralateral hemiplegia expected), gaze deviation
- Decline in consciousness is the key surgical trigger
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: large trauma craniectomy tray, dural expansion graft, bone-flap storage plan, ICP/EVD supplies if needed, and CT/CTA/MRI reviewed for dominant side and infarct extent.
- Special needs: arterial line, sodium/osmotherapy plan, antiplatelet/anticoagulation hold/restart plan, DVT/aspiration precautions, and family counseling about malignant edema trajectory.
- Immediate postop orders: ICU neuro checks, HOB 30, sodium/BP goals, CT timing, helmet precautions, DVT prophylaxis timing, swallow/rehab consults, and cranioplasty follow-up planning.
Diagnosis & Indication
- Working diagnosis: Malignant MCA infarction with mass effect
- Indication: Clinical deterioration (declining GCS), radiographic herniation, age (best outcomes < 60 but individualized), within ~48h of onset, before irreversible brainstem injury
- Goals: Relieve mass effect, prevent fatal herniation (life-saving, not function-restoring)
Position
- Supine, head turned contralateral, shoulder roll, Mayfield or horseshoe
Approach: Large Decompressive Hemicraniectomy
Key Surgical Steps
- Large reverse question-mark incision (frontotemporoparietal)
- Large bone flap — must be ≥ 12 cm AP diameter (ideally 14-15 cm) — inadequate size is the most common error and risks venous strangulation at bone edges
- Extend craniectomy to the floor of the middle fossa (temporal decompression critical — uncal/brainstem)
- Keep ~2-3 cm from midline (avoid sagittal sinus)
- Open dura widely — stellate or C-shaped
- Expansile duraplasty — dural substitute sewn in loosely to augment volume; do NOT close dura tightly
- Do NOT resect infarcted brain routinely (unless strangulated/necrotic herniating tissue causing closure problems)
- Bone flap stored (subcutaneous abdominal pocket or bone bank/freezer)
- Hemostasis, subgaleal drain, scalp closure
- [± ICP monitor]
Critical Anatomy & Structures at Risk
- Superior sagittal sinus — keep medial bone edge ~2.5 cm from midline
- Bridging veins / cortical veins — at bone edge if craniectomy too small → venous infarction/strangulation
- Middle fossa floor / temporal lobe — decompress to relieve uncal herniation
- Transverse sinus — posterior-inferior limit
Equipment
- Craniotome, high-speed drill
- Dural substitute (large graft for duraplasty)
- Bone storage materials
- ICP monitor/EVD
Anesthesia
- Arterial line, central line, Foley
- Mannitol/hypertonic saline (bridge to OR)
- Correct any coagulopathy
- Cefazolin 2g
Potential Complications
- Inadequate decompression (flap too small) → persistent herniation
- Hemorrhagic transformation of infarct
- Hydrocephalus
- Sinking skin flap syndrome (pre-cranioplasty)
- Infection
- Survivors with significant disability (counsel family pre-op)
Operative Note Template
Preoperative Diagnosis: Malignant [left/right] MCA territory infarction with cerebral edema, mass effect, and [declining consciousness / herniation]
Postoperative Diagnosis: Same
Procedure: [Left/Right] decompressive hemicraniectomy with expansile duraplasty [and ICP monitor placement]
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Implants: Dural substitute; bone flap stored [abdominal pocket / bone bank]; [ICP monitor] Complications: None
Indications: [Age]yo [M/F] with a malignant [left/right] MCA infarction (>50% territory) and clinical/radiographic deterioration (declining GCS, midline shift, cistern effacement). Decompression was offered as a life-saving measure; the family was counseled that survivors may have significant disability and elected to proceed.
Description of Procedure: After consent and time-out, general anesthesia was induced and the patient positioned supine with the head turned contralateral on a shoulder roll. A large reverse-question-mark incision was made and the myocutaneous flap reflected. Burr holes were placed and a large frontotemporoparietal bone flap was elevated with a craniotome; the AP diameter was [__] cm (≥12 cm). The temporal squama was rongeured down to the floor of the middle fossa, and the medial margin kept ~2.5 cm from the midline to protect the superior sagittal sinus and bridging veins.
The dura was opened widely in a stellate fashion, decompressing the swollen, infarcted hemisphere; non-viable infarcted brain was [not resected / debrided only where herniating and necrotic]. An expansile duraplasty was fashioned with a dural substitute sewn in loosely to augment intradural volume. [An ICP monitor was placed.] The bone flap was stored in [a subcutaneous abdominal pocket / the bone bank] for future cranioplasty. Hemostasis was confirmed, a subgaleal drain placed, and the scalp closed loosely in layers. The patient was transferred intubated to the NSICU in critical but stable condition.
Postoperative Plan
- NSICU, neuro checks q1h, ICP management
- HOB 30 degrees, Na 145-155 target if edema
- Serial CT (monitor edema peak days 2-5, hemorrhagic transformation)
- DVT prophylaxis (delayed chemical, esp. post-tPA)
- Seizure prophylaxis per practice
- Cranioplasty in ~6-12 weeks once edema resolved
- Early rehab evaluation, goals-of-care discussions
Chief-Level Case Review
Use these as the senior-level mental model for Decompressive Hemicraniectomy for Malignant MCA Infarction:
- Decision point: The operation is won or lost on control: identify inflow, outflow, perforators, collateral options, and the fastest route to temporary control before exposing the lesion itself.
- Technical lever: Do not accept a cosmetic result over physiology: ICG/Doppler/DSA, branch patency, perforator preservation, and parent-vessel caliber matter more than how the clip or resection bed looks.
- Bailout: Have a rupture or ischemia script ready: lower pressure, suction strategy, temporary occlusion time, heparin/reversal plan, bypass/reconstruction threshold, and postop BP targets.
- Postop watch: Postop danger is delayed: vasospasm, thromboembolism, hyperperfusion, hemorrhage, edema, hydrocephalus, and seizure plans need explicit orders.
Common Pimp Questions
Use these to pressure-test preparation for Decompressive Hemicraniectomy for Malignant MCA Infarction:
- What is the proximal-control plan before the lesion is manipulated?
- Which branch, perforator, or venous structure is most likely to be injured in this exposure?
- What are the intraoperative rupture steps, including temporary clip, suction, BP, and backup clip strategy?
- What confirms treatment success: ICG, Doppler, puncture/deflation, DSA, or postoperative CTA?
- What postoperative BP, vasospasm, antiplatelet, or anticoagulation issue changes the orders tonight?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Preferred approach side, sylvian split style, and cisternal-opening sequence: [attending-specific]
- Temporary clip threshold, burst-suppression preference, and BP during occlusion: [attending-specific]
- Clip manufacturer/shape sequence and whether Doppler, ICG, puncture, or intraop DSA is routine: [attending-specific]
- Antiplatelet/anticoagulation reversal and restart timing: [attending-specific]