
Case Prep: Pineal Region Tumor Resection
Case / Approach Snapshot
- Anatomy at risk: tumor compartment, arterial supply, venous drainage/sinuses, cranial nerves, white-matter tracts, pituitary/CSF pathways when relevant, and functional cortex.
- Operative steps: review imaging and goals, choose exposure, obtain brain relaxation, devascularize when possible, debulk internally, dissect capsule from critical structures, verify extent/safety, and reconstruct watertight closure; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: venous or arterial injury, swelling, seizure, cranial nerve or endocrine change, CSF leak, residual tumor left for safety, staged surgery, radiation, or adjuvant therapy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a pineal region tumor presenting with [Parinaud syndrome / hydrocephalus / headache] planned for [supracerebellar infratentorial / occipital transtentorial] approach for resection [after CSF diversion and tumor marker workup].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Supracerebellar-infratentorial approach — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- History of the pineal region tumor — Mottolese C. Neuro-Chirurgie 2015. PubMed
- Pineal region tumor: surgical anatomy and approach — Yamamoto I. Journal of neuro-oncology 2001. PubMed
- Desmoplastic myxoid tumor of the pineal region, SMARCB1 mutant: illustrative case — Zhou C. Journal of neurosurgery. Case lessons 2024. PubMed
- Papillary tumor of the pineal region in pediatric populations: An additional case and systematic review of a rare tumor entity — Mathkour M. Clinical neurology and neurosurgery 2021. PubMed
- Neurosurgical application of pineal region tumor resection with 3D 4K exoscopy via infratentorial approach: a retrospective cohort study — Hua W. International journal of surgery (London, England) 2023. PubMed
- Surgical corridor formation by minimally invasive lateral occipital infracortical supra-/transtentorial (OICST) approach in pineal region tumor surgery: A review of 11 cases — Staribacher D. Clinical neurology and neurosurgery 2024. PubMed
- Interhemispheric transcallosal intervenous approach to a pineal region tumor — Donoho DA. Neurosurgical focus: Video 2021. PubMed
- Intraoperative Imprint Cytology of SMARCB1-Mutant Desmoplastic Myxoid Tumor of the Pineal Region: A Case Report with Cytologic Differential Diagnosis and Literature Review — Kinoshita Y. Annals of clinical and laboratory science 2026. PubMed
- Microsurgical Management of Pineal Region Tumors — Ji X. World neurosurgery 2024. PubMed
- Pure endoscopic resection of pineal region tumors through supracerebellar infratentorial approach with ‘head-up’ park-bench position — Hua W. Neurological research 2023. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
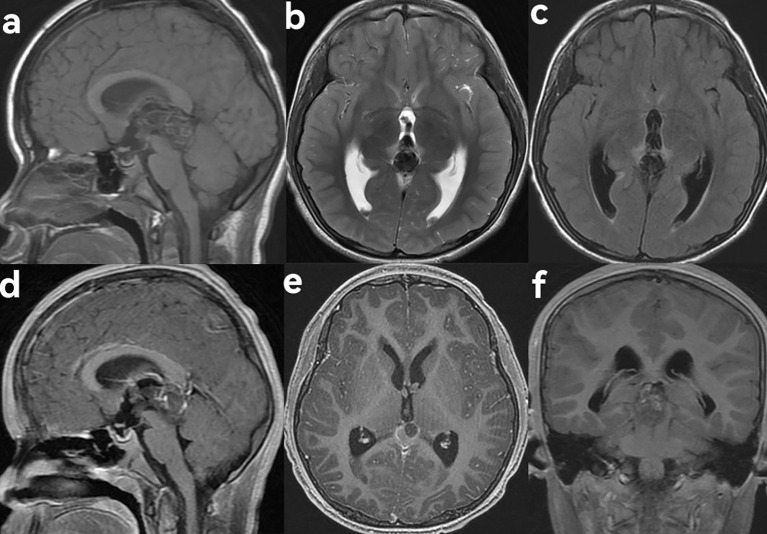 Figure 2. MRI findings of pineal region choriocarcinoma in a 9-year-old male patient presenting with dizziness and headache. (a) Sagittal T1WI showed a slightly hyperintense mass in the pineal… Source: Case Report: Primary choriocarcinoma of the pineal region — Frontiers in Oncology 2026; CC BY.
Figure 2. MRI findings of pineal region choriocarcinoma in a 9-year-old male patient presenting with dizziness and headache. (a) Sagittal T1WI showed a slightly hyperintense mass in the pineal… Source: Case Report: Primary choriocarcinoma of the pineal region — Frontiers in Oncology 2026; CC BY.
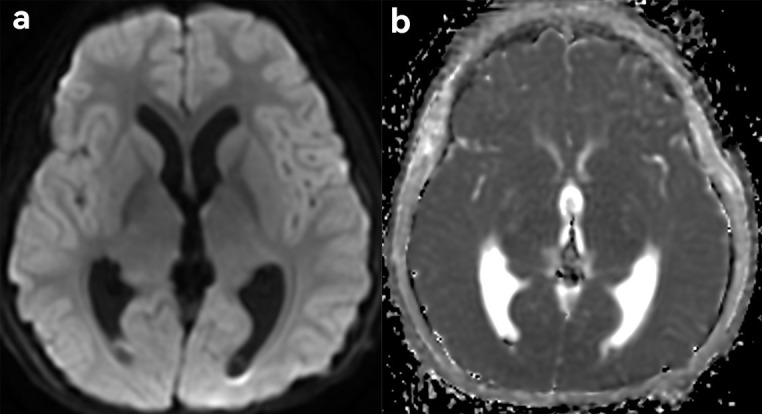 Figure 3. Diffusion-weighted imaging features (DWI). (a) On DWI, the solid component of the lesion appeared hypointense. (b) On apparent diffusion coefficient (ADC) mapping, the solid component… Source: Case Report: Primary choriocarcinoma of the pineal region — Frontiers in Oncology 2026; CC BY.
Figure 3. Diffusion-weighted imaging features (DWI). (a) On DWI, the solid component of the lesion appeared hypointense. (b) On apparent diffusion coefficient (ADC) mapping, the solid component… Source: Case Report: Primary choriocarcinoma of the pineal region — Frontiers in Oncology 2026; CC BY.
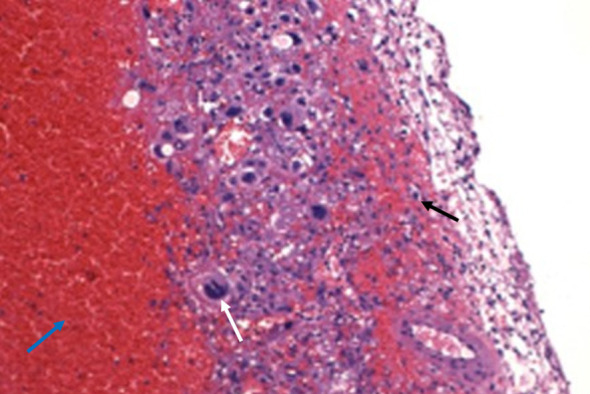 Figure 4. Pathological findings. Hemorrhage (blue arrow) and necrosis were observed within the lesion, with visible syncytiotrophoblasts (white arrow) and cytotrophoblasts (black arrow) showing… Source: Case Report: Primary choriocarcinoma of the pineal region — Frontiers in Oncology 2026; CC BY.
Figure 4. Pathological findings. Hemorrhage (blue arrow) and necrosis were observed within the lesion, with visible syncytiotrophoblasts (white arrow) and cytotrophoblasts (black arrow) showing… Source: Case Report: Primary choriocarcinoma of the pineal region — Frontiers in Oncology 2026; CC BY.
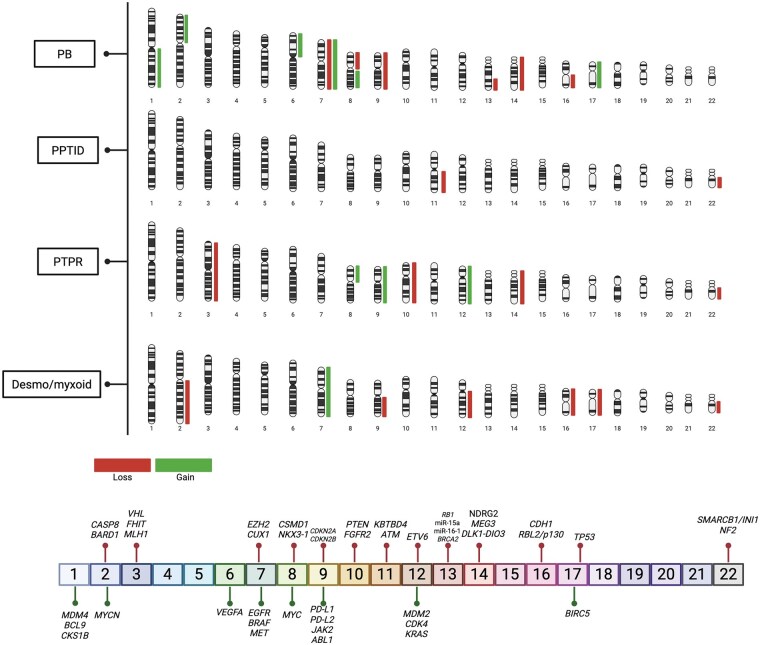 Figure 1.. Cytogenetic landscape of pineal parenchymal tumors. Representative chromosomal ideograms illustrating recurrent copy-number alterations (CNAs) across major pineal tumor subtypes,… Source: Genetic landscape and molecular targets in pediatric pineal tumors — Neuro-Oncology Advances 2026; CC BY.
Figure 1.. Cytogenetic landscape of pineal parenchymal tumors. Representative chromosomal ideograms illustrating recurrent copy-number alterations (CNAs) across major pineal tumor subtypes,… Source: Genetic landscape and molecular targets in pediatric pineal tumors — Neuro-Oncology Advances 2026; CC BY.
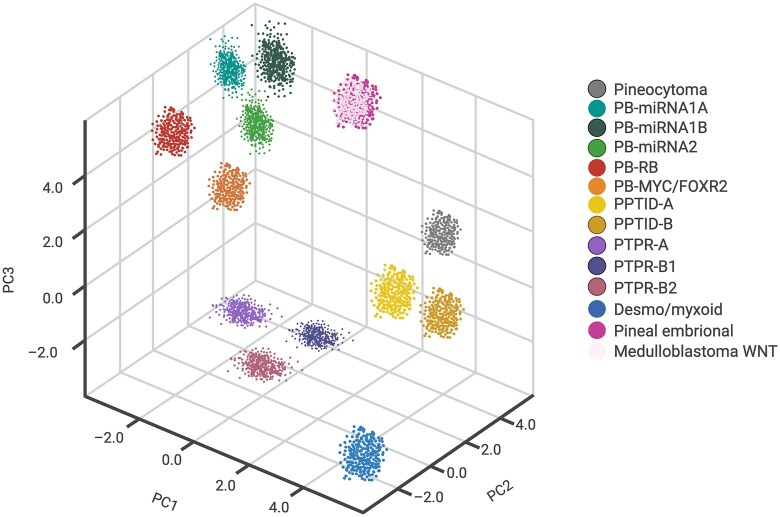 Figure 2.. Schematic overview of epigenetic clustering of pineal parenchymal tumors and related embryonal entities. This figure provides an illustrative summary of DNA methylation-based… Source: Genetic landscape and molecular targets in pediatric pineal tumors — Neuro-Oncology Advances 2026; CC BY.
Figure 2.. Schematic overview of epigenetic clustering of pineal parenchymal tumors and related embryonal entities. This figure provides an illustrative summary of DNA methylation-based… Source: Genetic landscape and molecular targets in pediatric pineal tumors — Neuro-Oncology Advances 2026; CC BY.
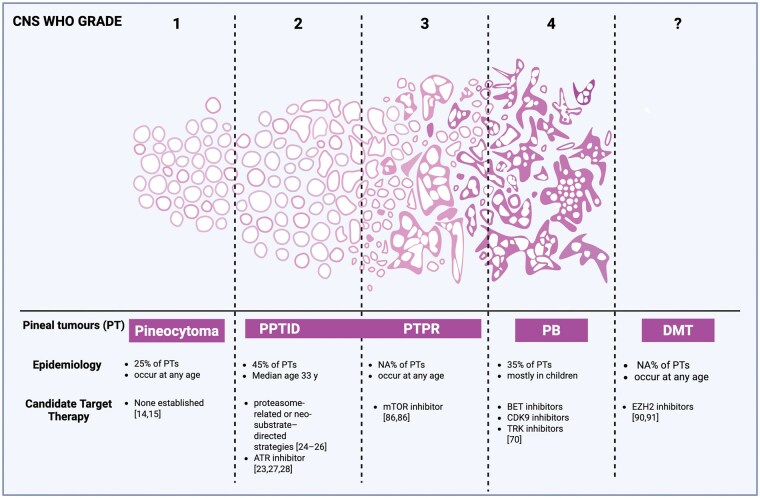 Figure 3.. Spectrum of pineal region tumors across WHO grades, epidemiological features, and candidate targeted therapies. Schematic overview of pineal parenchymal tumor entities according to CNS… Source: Genetic landscape and molecular targets in pediatric pineal tumors — Neuro-Oncology Advances 2026; CC BY.
Figure 3.. Spectrum of pineal region tumors across WHO grades, epidemiological features, and candidate targeted therapies. Schematic overview of pineal parenchymal tumor entities according to CNS… Source: Genetic landscape and molecular targets in pediatric pineal tumors — Neuro-Oncology Advances 2026; CC BY.
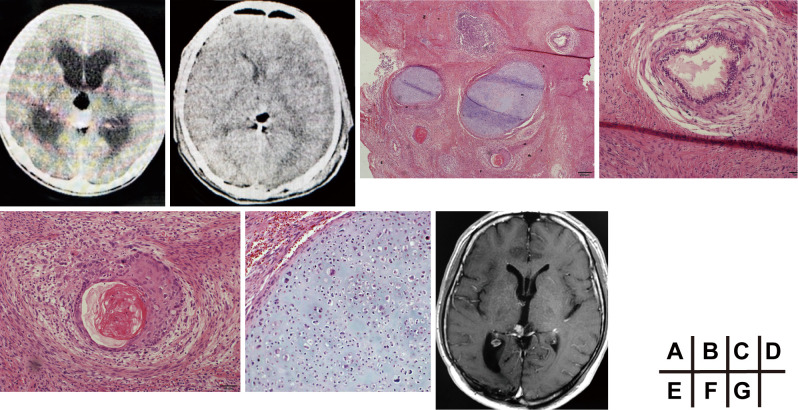 Figure 1. Preoperative imaging and initial histopathology.(A) Axial non-contrast CT showing a pineal region mass with acute obstructive hydrocephalus.(B) Postoperative non-contrast CT showing the… Source: An Ultra-late Recurrence with Adenoid Cystic Carcinoma-like Malignant Transformation of a Pineal Immature Teratoma after 35 Years: A Case Report — NMC Case Report Journal 2026; CC BY-NC-ND.
Figure 1. Preoperative imaging and initial histopathology.(A) Axial non-contrast CT showing a pineal region mass with acute obstructive hydrocephalus.(B) Postoperative non-contrast CT showing the… Source: An Ultra-late Recurrence with Adenoid Cystic Carcinoma-like Malignant Transformation of a Pineal Immature Teratoma after 35 Years: A Case Report — NMC Case Report Journal 2026; CC BY-NC-ND.
History of Present Illness
- Chief complaint: Headache, Parinaud syndrome (upgaze palsy, convergence-retraction nystagmus, light-near dissociation), hydrocephalus symptoms
- Tumor markers and hydrocephalus management precede resection
- Differential: germ cell tumors (germinoma — radiosensitive; teratoma), pineal parenchymal (pineocytoma/pineoblastoma), gliomas, meningioma
Imaging Review
MRI (T1±Gad, T2) + full neuraxis (germ cell/pineoblastoma — drop mets)
- Pineal region mass, aqueduct compression/hydrocephalus
- Relationship to deep venous system (internal cerebral veins, vein of Galen, basal veins, precentral cerebellar vein)
- Tentorial incisura, midbrain tectum, splenium
Workup — CRITICAL BEFORE SURGERY
- Serum + CSF tumor markers: AFP, beta-hCG (elevated → non-germinomatous germ cell tumor → chemo/RT, may avoid resection; pure germinoma → biopsy + RT/chemo)
- CSF cytology
- If markers diagnostic → may treat without resection
Labs
- CBC, BMP, Coags, AFP, beta-hCG (serum), Type and crossmatch
Neurological Examination
- Eye movements (upgaze, convergence, pupils), papilledema, ataxia, mental status
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: Mayfield, navigation, microscope/endoscope, cranial nerve monitoring/BAER when relevant, EVD/CSF diversion plan, watertight closure and fat/fascia graft materials, and blood available for vascular tumors.
- Special needs: arterial line, Foley, dexamethasone for edema, antiemetic plan, lower-CN airway/swallow contingency, EVD/ETV plan for hydrocephalus, and audiology/facial-nerve baseline when relevant.
- Immediate postop orders: ICU neuro checks, CN/eye movement/facial/swallow/voice exams, HOB 30, CT for hemorrhage/hydrocephalus, MRI for EOR, CSF-leak/pseudomeningocele watch, dex taper, and early swallow/ENT consult when lower CN risk exists.
Hydrocephalus & Diagnosis First
- ETV (treats hydrocephalus + allows endoscopic biopsy + CSF markers/cytology) OR EVD
- Tissue diagnosis guides whether resection needed (germinoma → RT, not resection)
Approach Selection
- Supracerebellar infratentorial (Krause): Midline, below deep veins, natural corridor above cerebellum under tentorium — workhorse for pineal tumors below the venous complex; sitting/Concorde/prone
- Occipital transtentorial (Poppen): For tumors extending supratentorially or above/lateral to venous complex; lateral to deep veins
- Paramedian supracerebellar variant to avoid midline bridging veins
Position
- Supracerebellar: sitting (gravity drops cerebellum — ideal) or Concorde/prone; Mayfield, neck flexed
- Occipital transtentorial: lateral or prone, occipital lobe retracted (gravity)
Key Surgical Steps (Supracerebellar Infratentorial)
- Midline suboccipital craniotomy above to expose transverse sinus/torcula
- Open dura, divide bridging veins from cerebellum to tentorium (paramedian variant preserves midline vermian veins)
- Let cerebellum fall away (gravity), develop supracerebellar corridor under tentorium
- Open arachnoid of quadrigeminal cistern; identify precentral cerebellar vein (may coagulate), vein of Galen complex above
- Stay below the deep venous system
- Debulk tumor (CUSA), dissect off tectum/midbrain, internal cerebral veins, vein of Galen
- Preserve deep veins; accept residual if adherent to veins/midbrain
- Hemostasis, watertight closure
Critical Anatomy & Structures at Risk
- Deep venous system — internal cerebral veins, vein of Galen, basal vein of Rosenthal, precentral cerebellar vein — injury catastrophic (venous infarction/hemorrhage)
- Midbrain tectum (quadrigeminal plate) — Parinaud, oculomotor
- Cerebellum, vermis
Equipment
- Microscope, navigation, CUSA, ICG
- Endoscope (ETV/biopsy), EVD kit
- Hemostatic agents, dural substitute
Monitoring
- SSEPs, MEPs; precordial Doppler (sitting — VAE)
Anesthesia
- Arterial line, VAE precautions (sitting) — central line, Doppler, end-tidal CO2; crossmatched blood; antiemetics
Potential Complications
- Venous infarction/hemorrhage (deep veins) — major mortality source
- Worsened Parinaud/oculomotor, ataxia
- VAE (sitting), hydrocephalus, hemorrhage into residual
- Pineal apoplexy
Operative Note Template
Preoperative Diagnosis: Pineal region tumor with [Parinaud syndrome / obstructive hydrocephalus]
Postoperative Diagnosis: Same (pending pathology)
Procedure: [Supracerebellar infratentorial / occipital transtentorial] approach for resection of pineal region tumor [following ETV/EVD]
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Adjuncts: Neuronavigation, CUSA, ICG, SSEP/MEP; [VAE precautions if sitting] Implants: Dural substitute; [EVD] Complications: None
Indications: [Age]yo [M/F] with a pineal region tumor and [hydrocephalus]. Serum/CSF tumor markers (AFP, beta-hCG) were [non-diagnostic, warranting resection] and hydrocephalus was managed with [ETV/EVD]. Risks (deep venous injury, Parinaud worsening, VAE) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced [with VAE precautions for the sitting position], and neuromonitoring established. [A prior ETV/EVD had been performed for CSF diversion and markers.] The patient was positioned [sitting/Concorde/prone] in Mayfield, and a midline suboccipital craniotomy performed exposing the transverse sinus/torcula.
The dura was opened and, via the supracerebellar infratentorial corridor, bridging veins from the cerebellum to the tentorium were divided as the cerebellum fell away, developing the corridor below the deep venous system. The quadrigeminal cistern arachnoid was opened, and the tumor debulked (CUSA) and dissected off the tectum, preserving the internal cerebral veins, vein of Galen, and basal veins; residual adherent to the deep veins/midbrain was left. [Occipital transtentorial: the occipital lobe was retracted with gravity and the tentorium divided to access supratentorial extension lateral to the deep veins.]
Hemostasis was obtained, a watertight closure performed, and the patient transferred to the ICU.
Postoperative Plan
- ICU, neuro checks q1h, eye movement exam
- CT 6h (hemorrhage), MRI postop; EVD/ETV management
- VAE monitoring if sitting used
- Pathology → tumor board: germinoma (RT/chemo), NGGCT (chemo+RT), pineal parenchymal/glioma per grade; neuraxis staging
- Antiemetics, steroid taper, DVT prophylaxis
Chief-Level Case Review
Use these as the senior-level mental model for Pineal Region Tumor Resection:
- Decision point: Decide the real endpoint before opening: cure, cytoreduction, diagnosis, decompression, separation from critical structures, or safe maximal resection.
- Technical lever: Map what must be left behind: perforators, cranial nerves, venous sinuses, eloquent cortex/tracts, hypothalamus/pituitary axis, and adherent capsule planes.
- Bailout: Sequence matters: devascularize early when safe, create CSF/working space, debulk before traction, and preserve the arachnoid plane unless oncologic goals justify violating it.
- Postop watch: The postop plan should match the risk structure: endocrine/vision/swallow/CN checks, steroid taper, seizure plan, MRI timing, CSF-leak watch, and adjuvant-treatment handoff.
Common Pimp Questions
Use these to pressure-test preparation for Pineal Region Tumor Resection:
- What is the surgical goal: gross-total, maximal safe, decompression, diagnosis, or cytoreduction?
- What eloquent cortex, tract, cranial nerve, vessel, or sinus defines the stopping point?
- What adjunct changes the case: navigation, mapping, 5-ALA, ultrasound, endoscope, ICG, or neuromonitoring?
- What is the edema, steroid, seizure, DVT, and postop imaging plan?
- What complication would you check for first in PACU based on this lesion location?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Extent-of-resection goal and functional stopping points: [attending-specific]
- Mapping/monitoring, 5-ALA, ultrasound, ICG, endoscope, or tractography preferences: [attending-specific]
- Steroid, antiepileptic, mannitol/hypertonic saline, and antibiotic plan: [attending-specific]
- Postop MRI timing, ICU/floor threshold, and adjuvant-referral workflow: [attending-specific]