
Case Prep: Cerebral Metastasis Resection
Case / Approach Snapshot
- Anatomy at risk: tumor compartment, arterial supply, venous drainage/sinuses, cranial nerves, white-matter tracts, pituitary/CSF pathways when relevant, and functional cortex.
- Operative steps: review imaging and goals, choose exposure, obtain brain relaxation, devascularize when possible, debulk internally, dissect capsule from critical structures, verify extent/safety, and reconstruct watertight closure; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: venous or arterial injury, swelling, seizure, cranial nerve or endocrine change, CSF leak, residual tumor left for safety, staged surgery, radiation, or adjuvant therapy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [known/newly diagnosed] [primary] and a [size] cm [left/right] [location] brain metastasis presenting with [seizures / focal deficit / headache] planned for craniotomy for resection.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
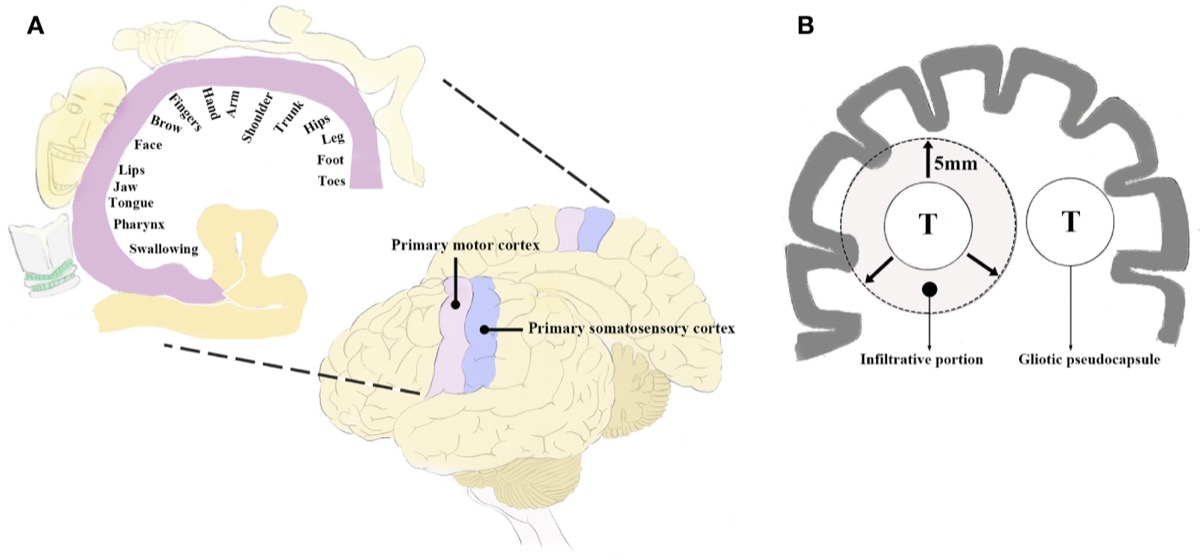
Perirolandic functional anatomy and BM infiltration up to ~5 mm beyond the pseudocapsule. Source: Zuo et al., Front Oncol 2020;10:572644, Fig 1. CC BY 4.0.
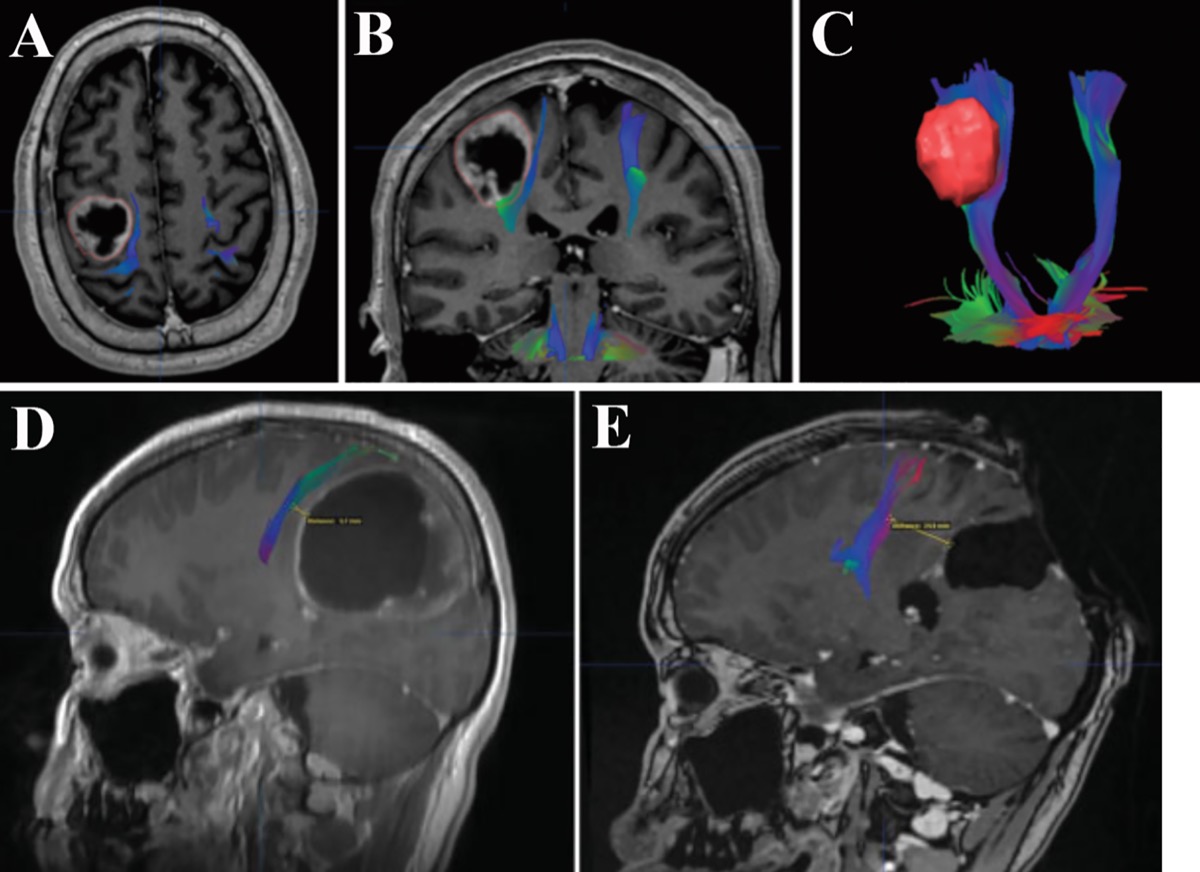
DTI/MRI fusion showing CST proximity and displacement; postop MRI confirming total removal. Source: Zuo et al., Front Oncol 2020;10:572644, Fig 2. CC BY 4.0.
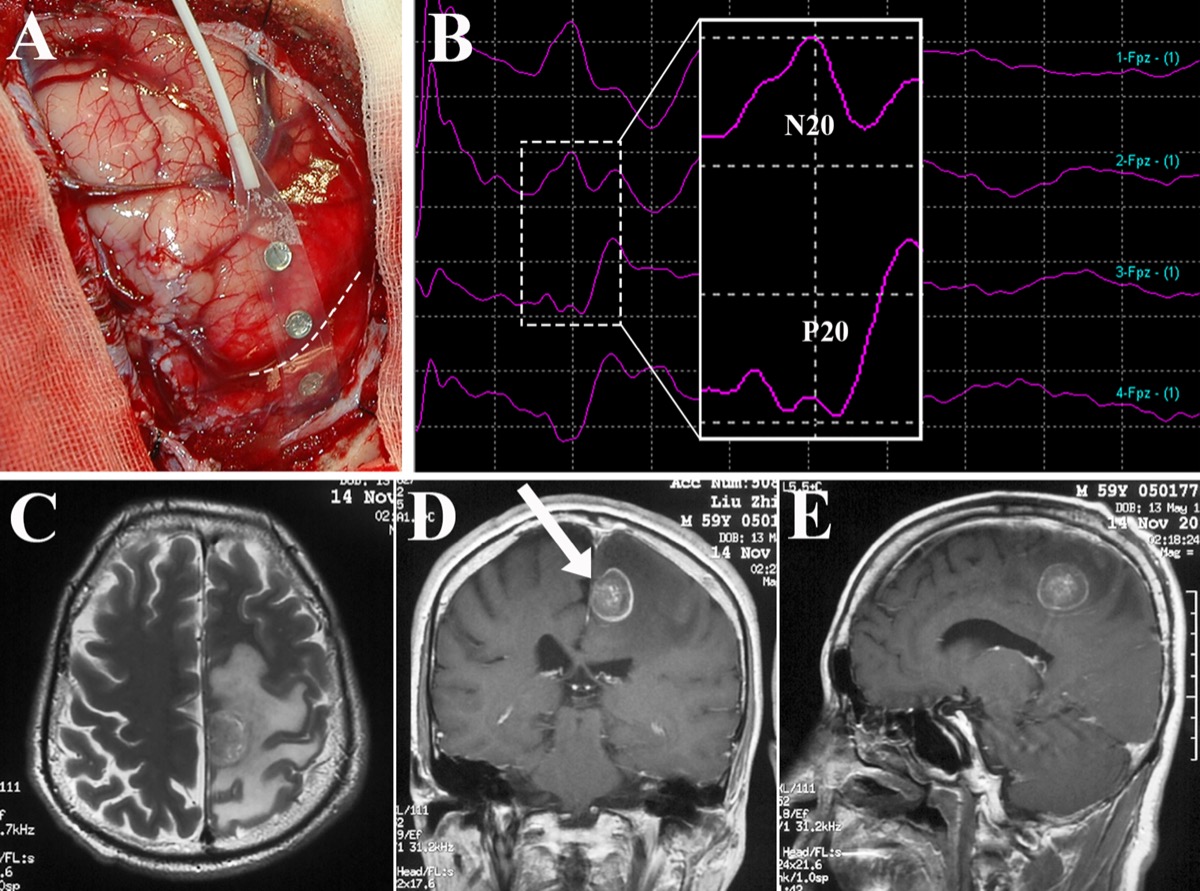
Central-sulcus identification by SEP phase reversal and motor mapping prior to perirolandic metastasis removal. Source: Zuo et al., Front Oncol 2020;10:572644, Fig 3. CC BY 4.0.
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Cerebral Metastasis of Hepatoblastoma: A Review — Rai P. Journal of pediatric hematology/oncology 2016. PubMed
- Cerebral Metastasis of Common Cancers — Kros JM. Cancers 2020. PubMed
- Cerebral metastasis and other central nervous system complications of pleuropulmonary blastoma — Priest JR. Pediatric blood & cancer 2007. PubMed
- Cerebral metastasis of cervical cancer, report of two cases and review of the literature — Setoodeh R. International journal of clinical and experimental pathology 2012. PubMed
- Cerebral metastasis from osteosarcoma: “Bone” in the brain — Kokkali S. Radiology case reports 2020. PubMed
- Single Cerebral Metastasis Mimicking Pyogenic Abscess in a Patient with Lung Adenocarcinoma — Pérez-Riverola V. Radiology. Imaging cancer 2023. PubMed
- Cerebral metastasis from ovarian cancer treated with a multidisciplinary approach. Case report and review of literature — Porzio G. European journal of gynaecological oncology 2003. PubMed
- Pleomorphic dermal sarcoma with cerebral metastasis — Trennheuser L. Journal der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology : JDDG 2020. PubMed
- Multiple cerebral aneurysms and brain metastasis from primary cardiac myxosarcoma: a case report and literature review — Lee TH. Chang Gung medical journal 2011. PubMed
- Ovarian Carcinoma Initially-presented as Cerebral Metastasis: Epidemiology, Pathology, and Outcomes — Qudsieh S. Materia socio-medica 2025. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
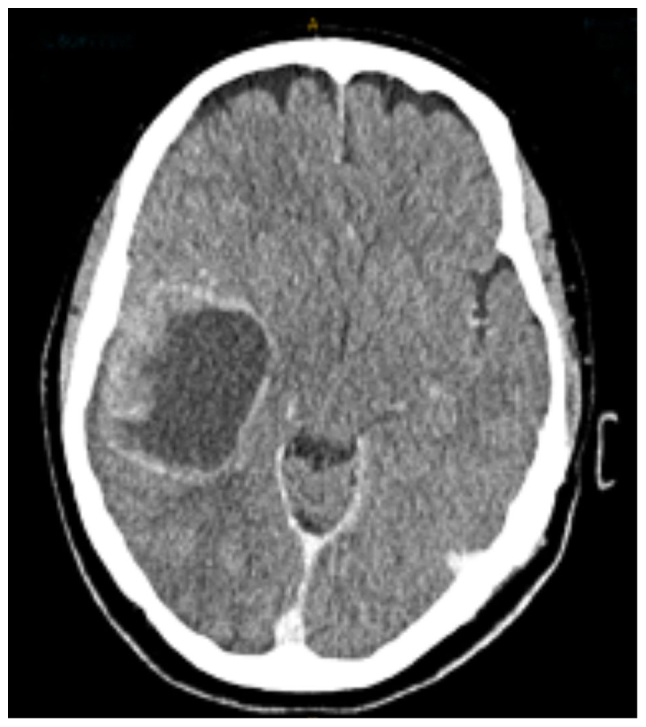 Figure 1.. Post-contrast axial CT scan demonstrating large peripherally enhancing heterogenous solid-cystic tumour with localised mass effect. CT, computed tomography. Source: Cerebral metastasis from anal squamous cell carcinoma: A case report and literature review — Oncology Letters 2025; CC BY.
Figure 1.. Post-contrast axial CT scan demonstrating large peripherally enhancing heterogenous solid-cystic tumour with localised mass effect. CT, computed tomography. Source: Cerebral metastasis from anal squamous cell carcinoma: A case report and literature review — Oncology Letters 2025; CC BY.
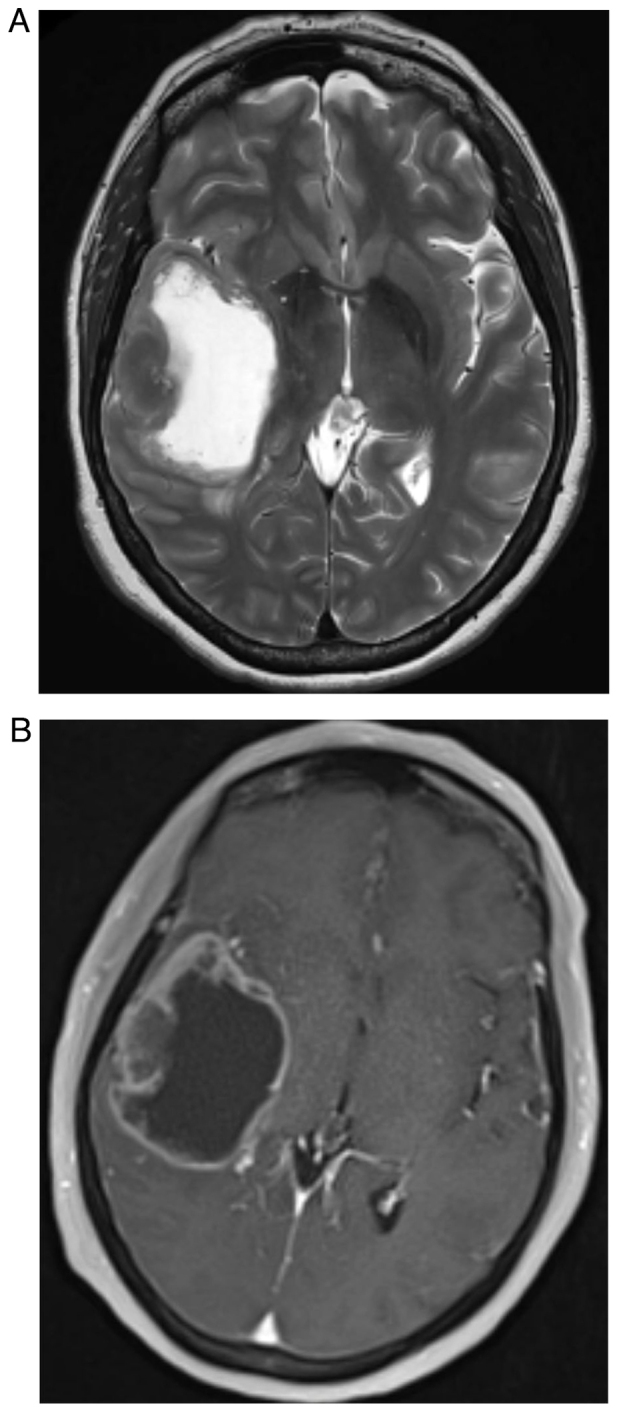 Figure 2.. T1 and T2 MR images demonstrating the metastatic tumour. (A) T2 MRI sequence demonstrating high signal intensity within a cystic centre surrounded by thickened heterogenous rim of tumour… Source: Cerebral metastasis from anal squamous cell carcinoma: A case report and literature review — Oncology Letters 2025; CC BY.
Figure 2.. T1 and T2 MR images demonstrating the metastatic tumour. (A) T2 MRI sequence demonstrating high signal intensity within a cystic centre surrounded by thickened heterogenous rim of tumour… Source: Cerebral metastasis from anal squamous cell carcinoma: A case report and literature review — Oncology Letters 2025; CC BY.
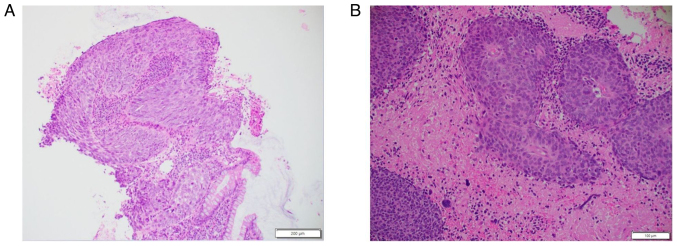 Figure 3.. Representative haematoxylin and eosin-stained sections. Stained sections demonstrating squamous cell carcinoma in the (A) primary anal tumour (scale bar, 200 µm) and (B) metastatic brain… Source: Cerebral metastasis from anal squamous cell carcinoma: A case report and literature review — Oncology Letters 2025; CC BY.
Figure 3.. Representative haematoxylin and eosin-stained sections. Stained sections demonstrating squamous cell carcinoma in the (A) primary anal tumour (scale bar, 200 µm) and (B) metastatic brain… Source: Cerebral metastasis from anal squamous cell carcinoma: A case report and literature review — Oncology Letters 2025; CC BY.
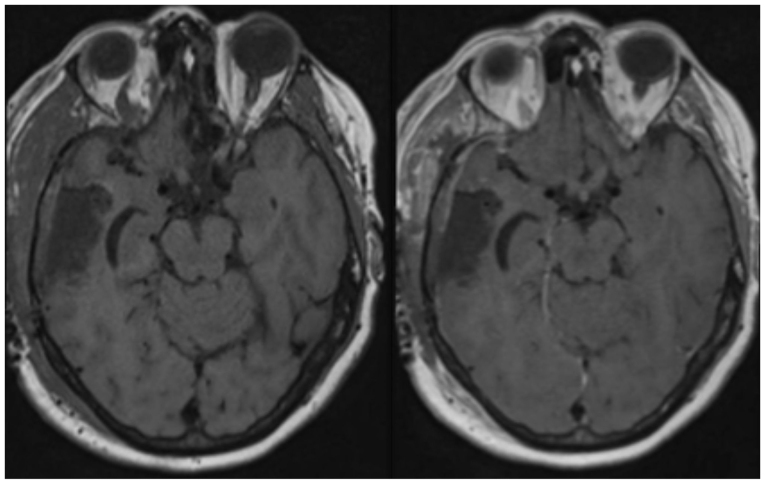 Figure 4.. Day 1 post-operative axial pre- and post-contrast T1-weighted MRI showing no significant residual tumour post-craniotomy and resection. Source: Cerebral metastasis from anal squamous cell carcinoma: A case report and literature review — Oncology Letters 2025; CC BY.
Figure 4.. Day 1 post-operative axial pre- and post-contrast T1-weighted MRI showing no significant residual tumour post-craniotomy and resection. Source: Cerebral metastasis from anal squamous cell carcinoma: A case report and literature review — Oncology Letters 2025; CC BY.
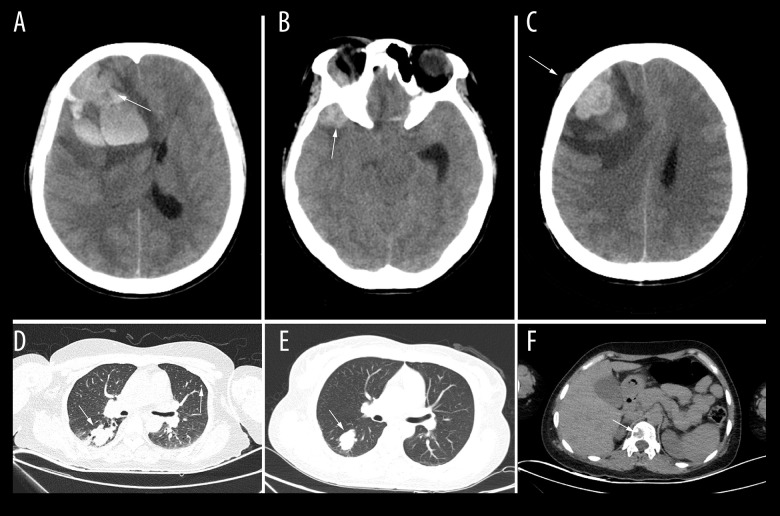 Figure 1.. Preoperative head and lung computed tomography (CT) showed late cerebral metastasis of melanoma. (A) Right frontal melanoma brain metastasis with intracranial hemorrhage compressing the… Source: A 41-Year-Old Woman with a Late Cerebral Metastasis 16 Years After an Initial Diagnosis of Cutaneous Melanoma — The American Journal of Case Reports 2022; CC BY-NC-ND.
Figure 1.. Preoperative head and lung computed tomography (CT) showed late cerebral metastasis of melanoma. (A) Right frontal melanoma brain metastasis with intracranial hemorrhage compressing the… Source: A 41-Year-Old Woman with a Late Cerebral Metastasis 16 Years After an Initial Diagnosis of Cutaneous Melanoma — The American Journal of Case Reports 2022; CC BY-NC-ND.
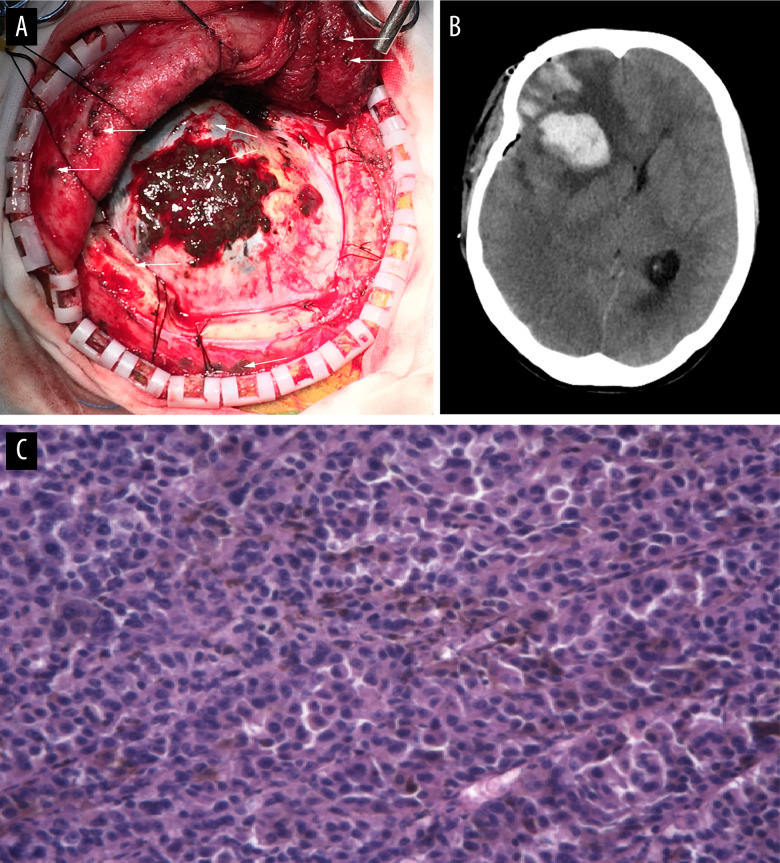 Figure 2.. Late cerebral metastasis of melanoma presents widespread dissemination in dural matter and adjacent temporal bone, temporalis and hypodermis. (A) The extradural part grew infiltratively… Source: A 41-Year-Old Woman with a Late Cerebral Metastasis 16 Years After an Initial Diagnosis of Cutaneous Melanoma — The American Journal of Case Reports 2022; CC BY-NC-ND.
Figure 2.. Late cerebral metastasis of melanoma presents widespread dissemination in dural matter and adjacent temporal bone, temporalis and hypodermis. (A) The extradural part grew infiltratively… Source: A 41-Year-Old Woman with a Late Cerebral Metastasis 16 Years After an Initial Diagnosis of Cutaneous Melanoma — The American Journal of Case Reports 2022; CC BY-NC-ND.
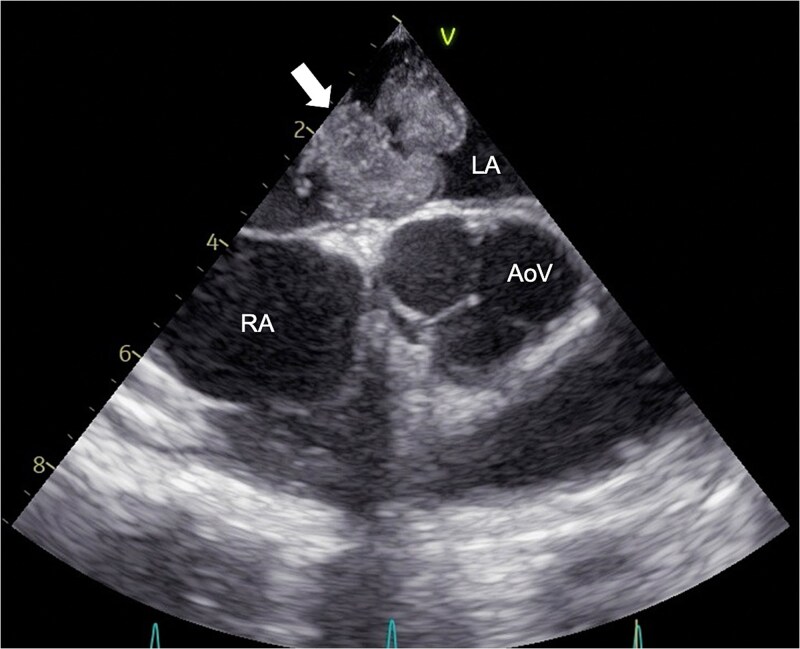 Figure 1. Preoperative echocardiography. Transesophageal echocardiography showing a 40-mm pedunculated tumor (arrowed) attached to the LA side of the atrial septum. RA, right atrium; LA, left… Source: Delayed cerebral metastasis after complete resection of left atrial cardiac myxoma: a case report — Oxford Medical Case Reports 2026; CC BY.
Figure 1. Preoperative echocardiography. Transesophageal echocardiography showing a 40-mm pedunculated tumor (arrowed) attached to the LA side of the atrial septum. RA, right atrium; LA, left… Source: Delayed cerebral metastasis after complete resection of left atrial cardiac myxoma: a case report — Oxford Medical Case Reports 2026; CC BY.
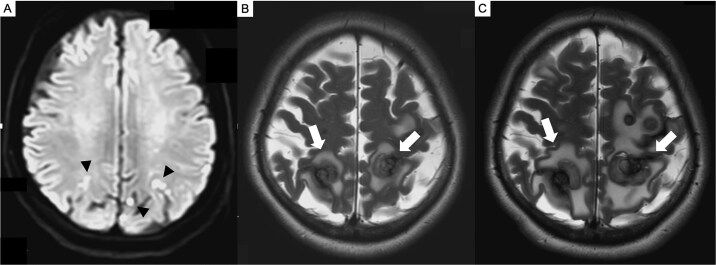 Figure 2. Brain MRI. (A) Preoperative diffusion-weighted imaging (DWI) showing multiple acute cerebral infarcts (arrowed) in the parietal lobe. (B) MRI (T2-weighted imaging) at 7 months… Source: Delayed cerebral metastasis after complete resection of left atrial cardiac myxoma: a case report — Oxford Medical Case Reports 2026; CC BY.
Figure 2. Brain MRI. (A) Preoperative diffusion-weighted imaging (DWI) showing multiple acute cerebral infarcts (arrowed) in the parietal lobe. (B) MRI (T2-weighted imaging) at 7 months… Source: Delayed cerebral metastasis after complete resection of left atrial cardiac myxoma: a case report — Oxford Medical Case Reports 2026; CC BY.
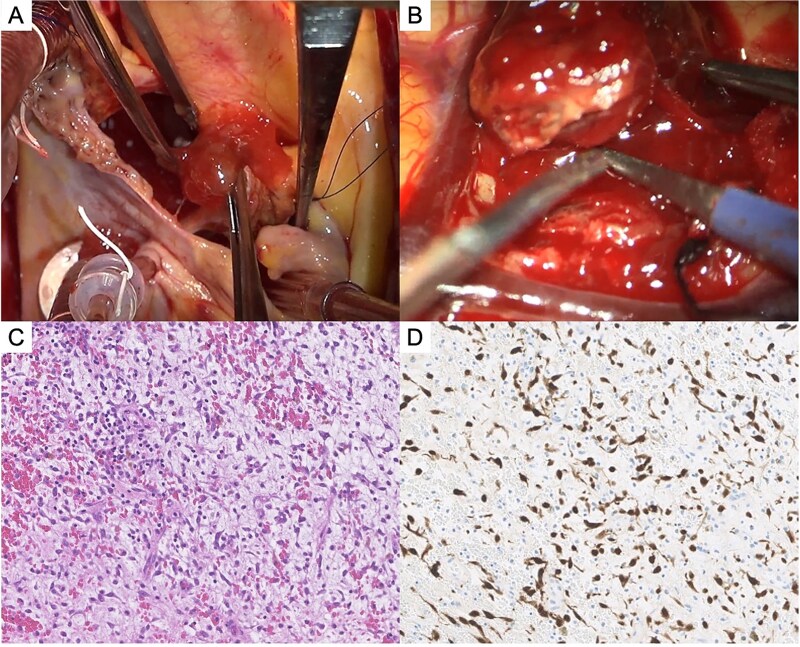 Figure 3. Tumor findings. (A) Intraoperative photograph of left atrial myxoma. (B) Intraoperative photograph of resected frontal lobe metastatic lesion. (C) Histopathology of cerebral metastatic… Source: Delayed cerebral metastasis after complete resection of left atrial cardiac myxoma: a case report — Oxford Medical Case Reports 2026; CC BY.
Figure 3. Tumor findings. (A) Intraoperative photograph of left atrial myxoma. (B) Intraoperative photograph of resected frontal lobe metastatic lesion. (C) Histopathology of cerebral metastatic… Source: Delayed cerebral metastasis after complete resection of left atrial cardiac myxoma: a case report — Oxford Medical Case Reports 2026; CC BY.
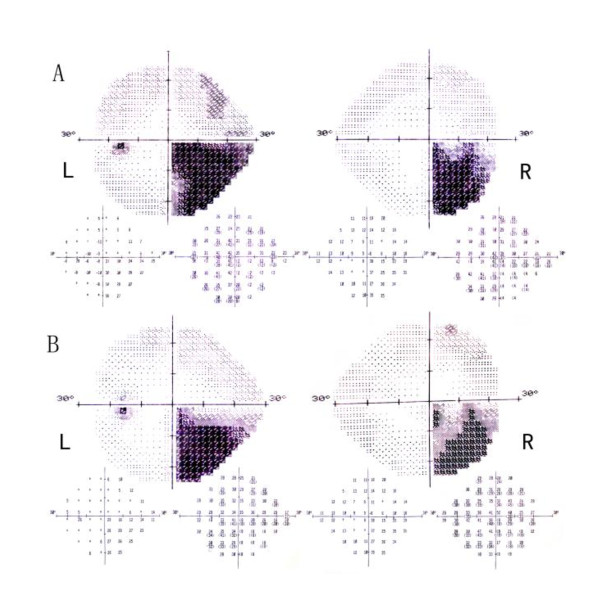 Figure 1. A (L: left eye; R: right eye) Humphrey visual field demonstrating a congruous right homonymous inferior quadrantanopsia. B Repeat visual field test showed slight improvement. Source: Homonymous Quadrantanopsia as the First Manifestation of Cerebral Metastasis of Invasive Mole: a case report — Journal of Medical Case Reports 2012; CC BY.
Figure 1. A (L: left eye; R: right eye) Humphrey visual field demonstrating a congruous right homonymous inferior quadrantanopsia. B Repeat visual field test showed slight improvement. Source: Homonymous Quadrantanopsia as the First Manifestation of Cerebral Metastasis of Invasive Mole: a case report — Journal of Medical Case Reports 2012; CC BY.
History of Present Illness
- Chief complaint: Seizure, focal deficit, headache, cognitive change
- Known primary (lung, breast, melanoma, renal, colorectal most common) vs metastasis as presentation
- Number of lesions (solitary vs oligometastatic vs multiple), systemic disease status, KPS
- Prior brain RT/SRS, prior craniotomy
Imaging Review
MRI (T1±Gad, T2, FLAIR, DWI, SWI)
- Location, size, number (full brain — surgical for symptomatic/large/dominant lesion)
- Classic: enhancing, gray-white junction, disproportionate vasogenic edema, often round/well-circumscribed
- Hemorrhagic mets (melanoma, renal, choriocarcinoma, thyroid) — SWI
- Eloquence, mass effect, herniation, midline shift
- DTI/fMRI if eloquent
Staging
- CT chest/abdomen/pelvis, PET, primary workup if unknown (tissue diagnosis may be the goal)
Labs
- CBC, BMP, Coags, Type and screen
- Hold anticoagulation; hemorrhagic mets considerations
Neurological Examination
- Complete exam per location; document baseline; KPS
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: Mayfield, navigation with latest MRI/DTI/functional data, microscope/exoscope, ultrasound/5-ALA/fluorescence when used, CUSA, cortical/subcortical mapping tools for eloquent lesions, and specimens/pathology workflow ready.
- Special needs: arterial line for large/eloquent/vascular tumors, dexamethasone plan, seizure prophylaxis for cortical lesions or seizure history, mannitol/hypertonic availability, language/motor mapping plan, and blood available for meningioma/skull-base cases.
- Immediate postop orders: neuro checks with deficit-specific exam, MRI brain with contrast within 24-48h when resection assessment matters, CT for hemorrhage concern, dex taper, antiepileptic duration, DVT timing, pathology/molecular follow-up, and rehab consults as needed.
Diagnosis & Indication
- Indication: Solitary/dominant symptomatic metastasis, accessible, good KPS/controlled systemic disease, need for tissue diagnosis, large lesion with mass effect; oligometastatic resectable disease
- Goals: Gross total en bloc resection (reduces local recurrence and leptomeningeal seeding vs piecemeal), relieve mass effect, tissue diagnosis
- Adjuvant: SRS to cavity (improves local control) ± SRS to other lesions; WBRT selectively
Position & Approach
- Per lesion location, navigation-guided craniotomy, lesion at highest point; awake/mapping if eloquent
Key Surgical Steps
- Navigation-planned craniotomy centered over lesion
- Corticotomy over/through sulcus near lesion (or directly if superficial), minimize normal cortex transgression
- Circumferential dissection in the gliotic/peritumoral plane (mets are usually well-demarcated, non-infiltrative)
- En bloc removal when feasible (supramarginal/circumferential technique reduces seeding/recurrence) — avoid piecemeal/internal debulking if possible (especially superficial)
- For deep/large: may debulk to mobilize, then deliver capsule
- Inspect cavity walls; consider resecting a margin of surrounding tissue if non-eloquent (improves local control)
- Hemostasis (mets can be vascular/hemorrhagic), navigation/ultrasound to confirm gross total
Critical Anatomy & Structures at Risk
- Eloquent cortex / white matter tracts (location-dependent)
- Draining veins, en passage vessels
- Deep nuclei (deep mets)
Equipment
- Microscope, navigation, ultrasound, CUSA (for debulking if needed)
- Bipolar, hemostatic agents, mapping (if eloquent)
Monitoring
- SSEPs/MEPs/mapping if eloquent location
Anesthesia
- Standard; dexamethasone (edema), levetiracetam, mannitol PRN
Potential Complications
- New neurological deficit (eloquent location)
- Hemorrhage (vascular mets)
- Leptomeningeal dissemination (reduced by en bloc)
- Edema, seizures, infection
Operative Note Template
Preoperative Diagnosis: [Solitary/dominant] [left/right] [location] brain metastasis [from known ___ primary] with [mass effect/edema/symptom]
Postoperative Diagnosis: Same
Procedure: [Left/Right] [location] craniotomy for microsurgical resection of brain metastasis [with neuronavigation] [with intraoperative mapping]
Surgeon / Assistant: Anesthesia: General endotracheal [/ awake with mapping] EBL / Fluids: Specimens: Brain tumor (metastasis) for permanent pathology Implants: None Monitoring: [SSEP/MEP/mapping if eloquent — stable] Complications: None
Indications: [Age]yo [M/F] with [known/newly diagnosed] [primary] and a [size] cm symptomatic [location] brain metastasis causing [deficit/seizure/mass effect]. Given the accessible location, [solitary/dominant] lesion, and [good KPS/controlled systemic disease / need for tissue diagnosis], surgical resection (with planned adjuvant SRS to the cavity) was recommended. Risks/benefits/alternatives discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced and the head fixed in Mayfield. Neuronavigation was registered and the lesion projected; a [location] craniotomy was planned over the lesion. The patient was positioned with the lesion at the highest point. [Mapping was set up for the eloquent-adjacent location.]
The scalp was opened and a craniotomy turned over the navigated target; the dura was opened. The cortical surface was inspected and the lesion localized with navigation [and ultrasound]. A corticotomy was made [through a sulcus / over the superficial lesion], and the metastasis — which was [well-circumscribed] — was circumferentially dissected in the surrounding gliotic plane. The lesion was removed en bloc [/ debulked then delivered for the deep component] to minimize tumor spillage and seeding. The cavity walls were inspected [and a margin of non-eloquent peritumoral tissue resected to improve local control]. Meticulous hemostasis was obtained and gross-total resection confirmed by navigation/ultrasound.
The dura was closed, the bone flap replaced and fixed, and the scalp closed in layers. The patient was awakened neurologically [at baseline] and transferred to the [ICU/step-down] in stable condition.
Postoperative Plan
- ICU/step-down, neuro checks q1h
- MRI with gad < 48h (EOR), CT if hemorrhage concern
- Dexamethasone taper, seizure prophylaxis per practice
- DVT prophylaxis
- Adjuvant: SRS to resection cavity (tumor board), systemic therapy coordination with oncology
- Pathology (confirm primary/molecular markers), restage, oncology follow-up
Chief-Level Case Review
Use these as the senior-level mental model for Cerebral Metastasis Resection:
- Decision point: Decide the real endpoint before opening: cure, cytoreduction, diagnosis, decompression, separation from critical structures, or safe maximal resection.
- Technical lever: Map what must be left behind: perforators, cranial nerves, venous sinuses, eloquent cortex/tracts, hypothalamus/pituitary axis, and adherent capsule planes.
- Bailout: Sequence matters: devascularize early when safe, create CSF/working space, debulk before traction, and preserve the arachnoid plane unless oncologic goals justify violating it.
- Postop watch: The postop plan should match the risk structure: endocrine/vision/swallow/CN checks, steroid taper, seizure plan, MRI timing, CSF-leak watch, and adjuvant-treatment handoff.
Common Pimp Questions
Use these to pressure-test preparation for Cerebral Metastasis Resection:
- What is the surgical goal: gross-total, maximal safe, decompression, diagnosis, or cytoreduction?
- What eloquent cortex, tract, cranial nerve, vessel, or sinus defines the stopping point?
- What adjunct changes the case: navigation, mapping, 5-ALA, ultrasound, endoscope, ICG, or neuromonitoring?
- What is the edema, steroid, seizure, DVT, and postop imaging plan?
- What complication would you check for first in PACU based on this lesion location?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Extent-of-resection goal and functional stopping points: [attending-specific]
- Mapping/monitoring, 5-ALA, ultrasound, ICG, endoscope, or tractography preferences: [attending-specific]
- Steroid, antiepileptic, mannitol/hypertonic saline, and antibiotic plan: [attending-specific]
- Postop MRI timing, ICU/floor threshold, and adjuvant-referral workflow: [attending-specific]