
Case Prep: Depressed Skull Fracture Elevation
Case / Approach Snapshot
- Anatomy at risk: hematoma compartment, fracture and sinus landmarks, cortical/venous/arterial injury, swollen brain physiology, dural edges, and decompressive flap constraints.
- Operative steps: move quickly from imaging to exposure, choose flap or burr-hole strategy, evacuate clot or decompress, control bleeding, decide duraplasty/bone-flap/drain strategy, and hand off to ICU resuscitation goals; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: refractory swelling, coagulopathy, venous sinus bleeding, arterial source, seizures, infection, hydrocephalus, malignant ICP, and staged decompression or reoperation.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [closed/open (compound)] depressed skull fracture of the [location] [± underlying dural/parenchymal injury] following [mechanism] planned for craniotomy for elevation and debridement.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
External sources — operative figures/atlases are copyrighted (linked, not copied). See media-sources.md for licensing.
Operative technique & approach
- The Neurosurgical Atlas — search “depressed skull fracture” (operative illustrations + HD video)
- AANS Neurosurgeon — trauma craniotomy and skull fracture management articles
Imaging
Open-access figures
High-Yield Literature
- Elevation of Depressed Skull Fracture in Neonates Using a Breast Pump and a Custom-Molded Flange — Martinez EL. Operative neurosurgery (Hagerstown, Md.) 2024. PubMed
- Depressed Skull Fracture in Infants: The Role of Vacuum-Assisted Intervention — Villahermosa A. NeoReviews 2024. PubMed
- Depressed skull fracture compressing eloquent cortex causing focal neurologic deficits — In A. Brain injury 2023. PubMed
- Everted skull fracture — Balasubramaniam S. World neurosurgery 2011. PubMed
- Midline depressed skull fracture presenting with quadriplegia: A rare phenomenon — Mathew MJ. Surgical neurology international 2017. PubMed
- Delayed repair of open depressed skull fracture — Curry DJ. Pediatric neurosurgery 1999. PubMed
- The Evolution of Modern Treatment for Depressed Skull Fractures — Stein SC. World neurosurgery 2019. PubMed
- Pediatric ping-pong skull fractures treated with vacuum-assisted elevation — Ahmed SD. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2024. PubMed
- Depressed skull fracture overlying the superior sagittal sinus causing benign intracranial hypertension. Description of two cases and review of the literature — Fuentes S. British journal of neurosurgery 2005. PubMed
- Depressed skull fracture in Ping Pong: elevation with Medeva extractor — Mastrapa TL. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2007. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
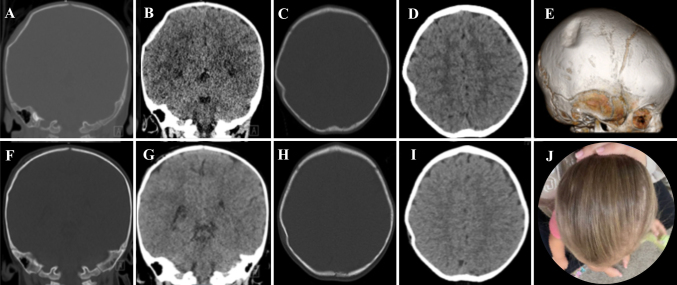 FIG. 1.. Case 1.Preoperative coronal bone (A) and brain (B) window noncontrast CT scans, axial bone (C) and brain (D) window noncontrast CT scans, and a 3D reconstruction (E) showing a depressed… Source: Use of a percutaneous bone fiducial screw for elevating simple closed depressed skull fractures: illustrative cases — Journal of Neurosurgery: Case Lessons 2024; CC BY-NC-ND.
FIG. 1.. Case 1.Preoperative coronal bone (A) and brain (B) window noncontrast CT scans, axial bone (C) and brain (D) window noncontrast CT scans, and a 3D reconstruction (E) showing a depressed… Source: Use of a percutaneous bone fiducial screw for elevating simple closed depressed skull fractures: illustrative cases — Journal of Neurosurgery: Case Lessons 2024; CC BY-NC-ND.
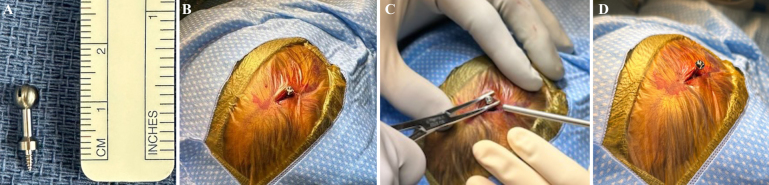 FIG. 2.. Case 1. A: The bone fiducial used: total length 1.5 cm, screwhead length 3 mm. B: Percutaneous placement of the bone fiducial at the point of maximal fracture depression. C: Elevation of… Source: Use of a percutaneous bone fiducial screw for elevating simple closed depressed skull fractures: illustrative cases — Journal of Neurosurgery: Case Lessons 2024; CC BY-NC-ND.
FIG. 2.. Case 1. A: The bone fiducial used: total length 1.5 cm, screwhead length 3 mm. B: Percutaneous placement of the bone fiducial at the point of maximal fracture depression. C: Elevation of… Source: Use of a percutaneous bone fiducial screw for elevating simple closed depressed skull fractures: illustrative cases — Journal of Neurosurgery: Case Lessons 2024; CC BY-NC-ND.
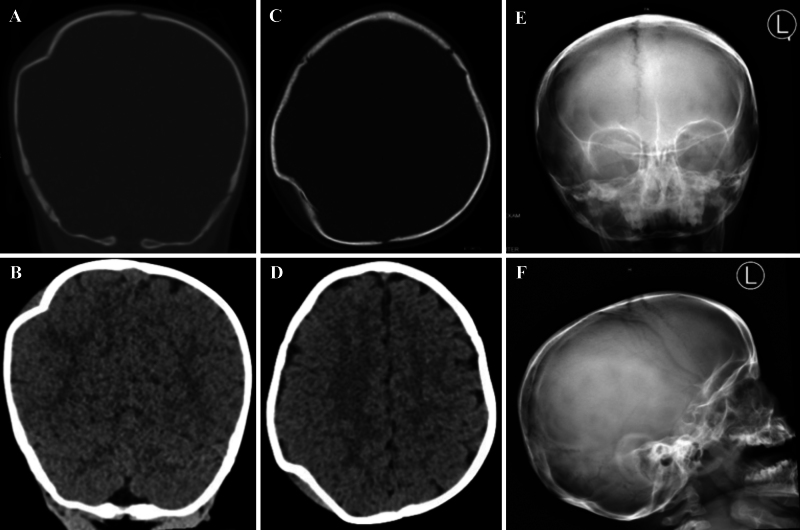 FIG. 3.. Case 2.Images showing the elevation of a right parietal depressed skull fracture. Preoperative coronal bone (A) and brain (B) window noncontrast CT scans. Preoperative axial bone (C) and… Source: Use of a percutaneous bone fiducial screw for elevating simple closed depressed skull fractures: illustrative cases — Journal of Neurosurgery: Case Lessons 2024; CC BY-NC-ND.
FIG. 3.. Case 2.Images showing the elevation of a right parietal depressed skull fracture. Preoperative coronal bone (A) and brain (B) window noncontrast CT scans. Preoperative axial bone (C) and… Source: Use of a percutaneous bone fiducial screw for elevating simple closed depressed skull fractures: illustrative cases — Journal of Neurosurgery: Case Lessons 2024; CC BY-NC-ND.
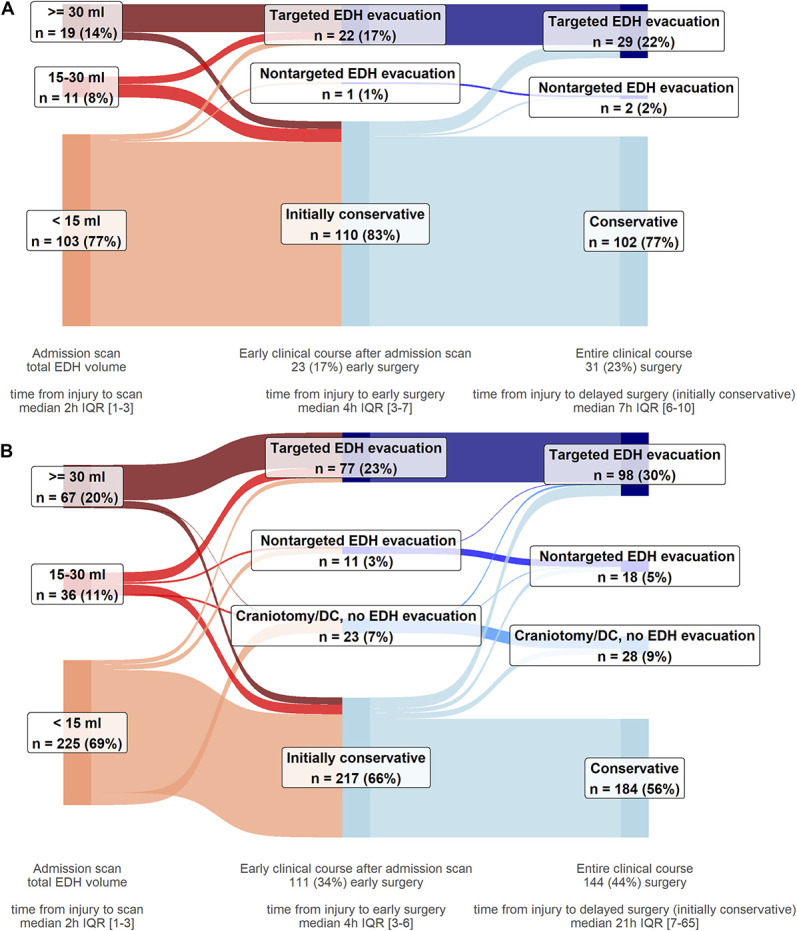 FIGURE 2.. Surgical care pathways of participants with EDHs, by presence of concomitant acute subdural hematomas and/or IPHs on the first scan. A, Participants with isolated EDHs (n = 133). Most of… Source: Clinical and Imaging Characteristics, Care Pathways, and Outcomes of Traumatic Epidural Hematomas: A Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury Study — Neurosurgery 2024; CC BY.
FIGURE 2.. Surgical care pathways of participants with EDHs, by presence of concomitant acute subdural hematomas and/or IPHs on the first scan. A, Participants with isolated EDHs (n = 133). Most of… Source: Clinical and Imaging Characteristics, Care Pathways, and Outcomes of Traumatic Epidural Hematomas: A Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury Study — Neurosurgery 2024; CC BY.
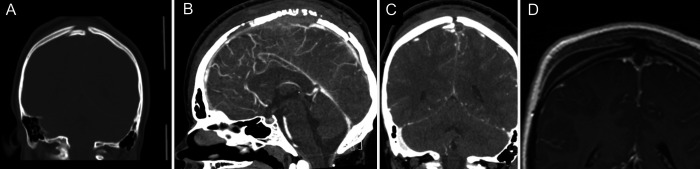 FIG. 1.. A: Coronal CT shows depressed skull fracture fragment at midline. B: Sagittal CT venogram (CTV) shows occlusion of SSS anterior to fracture. C: Coronal CTV shows thrombus in sagittal… Source: Pediatric skull fracture with injury and thrombosis of the superior sagittal sinus: illustrative case — Journal of Neurosurgery: Case Lessons 2022; CC BY-NC-ND.
FIG. 1.. A: Coronal CT shows depressed skull fracture fragment at midline. B: Sagittal CT venogram (CTV) shows occlusion of SSS anterior to fracture. C: Coronal CTV shows thrombus in sagittal… Source: Pediatric skull fracture with injury and thrombosis of the superior sagittal sinus: illustrative case — Journal of Neurosurgery: Case Lessons 2022; CC BY-NC-ND.
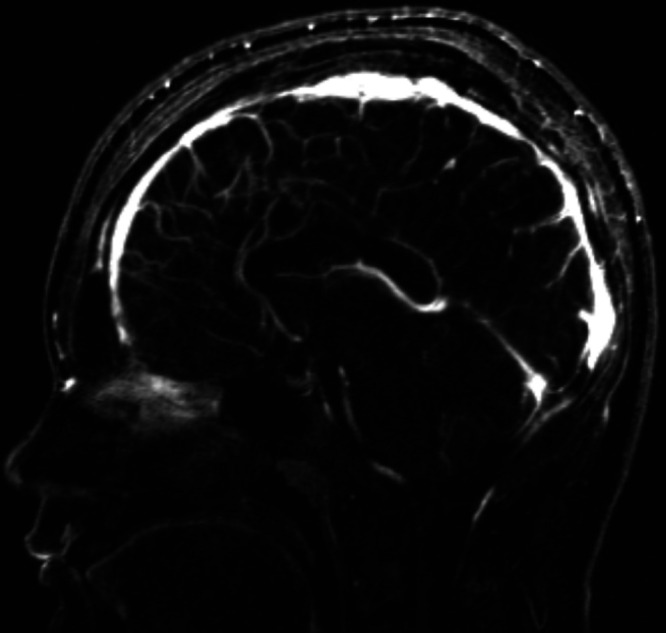 FIG. 2.. MRV at follow-up showing resolution of sagittal sinus thrombosis. Source: Pediatric skull fracture with injury and thrombosis of the superior sagittal sinus: illustrative case — Journal of Neurosurgery: Case Lessons 2022; CC BY-NC-ND.
FIG. 2.. MRV at follow-up showing resolution of sagittal sinus thrombosis. Source: Pediatric skull fracture with injury and thrombosis of the superior sagittal sinus: illustrative case — Journal of Neurosurgery: Case Lessons 2022; CC BY-NC-ND.
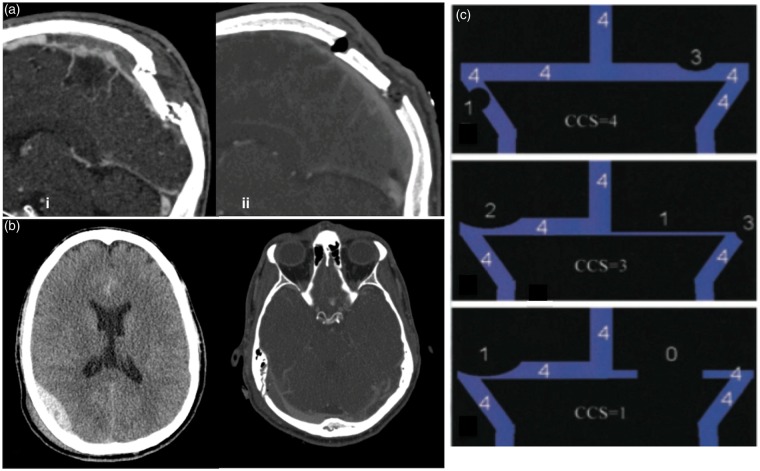 Figure 4.. (a) Depressed skull fracture and subsequent (superior sagittal sinus) SSS thrombosis caused by a hammer blow – (i) midsagittal reconstruction on day 2 with increasing headaches… Source: Monro-Kellie 2.0: The dynamic vascular and venous pathophysiological components of intracranial pressure — Journal of Cerebral Blood Flow & Metabolism 2016; CC BY-NC.
Figure 4.. (a) Depressed skull fracture and subsequent (superior sagittal sinus) SSS thrombosis caused by a hammer blow – (i) midsagittal reconstruction on day 2 with increasing headaches… Source: Monro-Kellie 2.0: The dynamic vascular and venous pathophysiological components of intracranial pressure — Journal of Cerebral Blood Flow & Metabolism 2016; CC BY-NC.
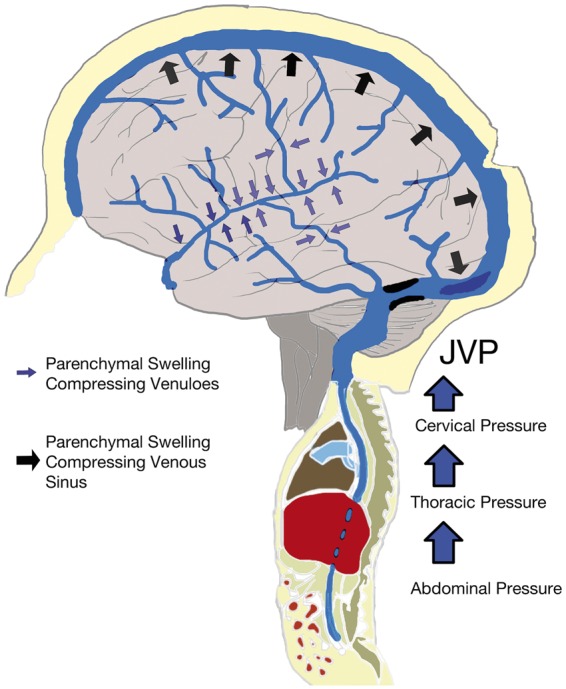 Figure 7.. Diagram demonstrating that relative venous outflow restriction can occur intracranially (with compression/obstruction (e.g. with thrombus or fractures) of isolated or diffuse venous… Source: Monro-Kellie 2.0: The dynamic vascular and venous pathophysiological components of intracranial pressure — Journal of Cerebral Blood Flow & Metabolism 2016; CC BY-NC.
Figure 7.. Diagram demonstrating that relative venous outflow restriction can occur intracranially (with compression/obstruction (e.g. with thrombus or fractures) of isolated or diffuse venous… Source: Monro-Kellie 2.0: The dynamic vascular and venous pathophysiological components of intracranial pressure — Journal of Cerebral Blood Flow & Metabolism 2016; CC BY-NC.
 Figure 1. Illustrative case – Lateral head photograph showing the depressed skull fracture (black arrow). Source: Closed Depressed Skull Fracture in Childhood Reduced with Suction Cup Vacuum Method: Case Report and a Systematic Literature Review — Cureus 2019; CC BY.
Figure 1. Illustrative case – Lateral head photograph showing the depressed skull fracture (black arrow). Source: Closed Depressed Skull Fracture in Childhood Reduced with Suction Cup Vacuum Method: Case Report and a Systematic Literature Review — Cureus 2019; CC BY.
 Figure 2. Illustrative case – Anteroposterior X-ray showing the bone deformity (white arrow). Source: Closed Depressed Skull Fracture in Childhood Reduced with Suction Cup Vacuum Method: Case Report and a Systematic Literature Review — Cureus 2019; CC BY.
Figure 2. Illustrative case – Anteroposterior X-ray showing the bone deformity (white arrow). Source: Closed Depressed Skull Fracture in Childhood Reduced with Suction Cup Vacuum Method: Case Report and a Systematic Literature Review — Cureus 2019; CC BY.
History of Present Illness
- Chief complaint: Head trauma with scalp laceration / focal deficit / seizure
- Mechanism: blunt focal impact, assault, fall, projectile
- Open vs closed: open (compound) = scalp laceration communicating with fracture → infection risk → urgent surgery
- GCS at scene → current:
- Focal deficits, seizure, CSF leak from wound
- Time since injury:
- Contamination: soil, debris, hair in wound (open fractures)
Past Medical History
- Anticoagulant use (warfarin, DOACs — apixaban, rivaroxaban, dabigatran)
- Antiplatelet use (aspirin, clopidogrel, ticagrelor)
- Coagulopathy (hemophilia, liver disease, thrombocytopenia)
- Immunosuppression (steroids, chemotherapy, transplant) — increased infection risk with open fractures
- Prior craniotomy or craniectomy (altered anatomy, existing hardware)
- Seizure history
- Prior TBI
- Diabetes (wound healing, infection risk)
- Alcohol/substance use (fall risk, coagulopathy)
- Tetanus immunization status (critical for open/compound fractures)
- Allergies:
- Medications:
Imaging Review
CT Head — Bone Windows
- Depression depth: Surgical if depressed greater than full skull thickness (~1 table width) or beyond the inner table
- Fragment pattern: Single depressed fragment vs comminuted (multiple fragments)
- Location: Convexity (frontal, parietal, temporal, occipital); over a venous sinus (relative caution)
- Overlying laceration / air: Suggests open (compound) fracture
- Frontal sinus involvement: Requires cranialization or obliteration if posterior wall fractured
- Foreign body: Projectile fragments, bone driven intracranially
CT Head — Brain Windows
- Underlying contusion: Hemorrhagic contusion beneath the depressed segment
- Epidural / subdural hematoma: Associated extra-axial collection requiring evacuation
- Pneumocephalus: Air intracranially confirms dural violation
- Intraventricular hemorrhage: Severity marker
- Midline shift: From underlying mass lesion
CT Venogram (if fracture overlies a venous sinus)
- Sinus patency: Patent vs thrombosed vs lacerated
- Relationship of depressed fragments to sinus wall
- Collateral venous drainage (if sinus sacrifice may be required)
Criteria for Surgical Intervention
- Depression greater than one full table thickness (inner table)
- Open (compound) fracture — urgent debridement and elevation
- Underlying mass lesion requiring evacuation (EDH, SDH, contusion)
- Dural laceration / CSF leak
- Gross cosmetic deformity
- Neurological deficit attributable to the fracture
- Frontal sinus posterior wall involvement
- Non-operative candidates: Closed fracture, minimal depression, no dural breach, no deficit, no cosmetic concern — serial imaging and observation
Labs
- CBC (Hgb baseline, Plt > 100K for surgery)
- Coagulation panel (PT/INR, PTT) — reverse anticoagulation before surgery
- INR > 1.5 on warfarin: 4-factor PCC (KCentra) + vitamin K 10 mg IV
- On DOACs: reversal per agent (idarucizumab for dabigatran; andexanet alfa or 4F-PCC for factor Xa inhibitors)
- Type and crossmatch (2 units pRBC — especially if fracture over a venous sinus)
- BMP (Na, K, Cr — baseline)
- Blood alcohol level and urine drug screen (trauma protocol)
- Wound culture — obtain if open/contaminated fracture before antibiotic administration (guides targeted therapy)
- Tetanus status — administer Td/Tdap if immunization not current; add TIG if immunization history unknown or incomplete
Neurological Examination
Glasgow Coma Scale (GCS)
- Eye opening (E): Spontaneous (4) / To voice (3) / To pain (2) / None (1)
- Verbal (V): Oriented (5) / Confused (4) / Inappropriate words (3) / Incomprehensible (2) / None (1)
- Motor (M): Obeys (6) / Localizes (5) / Withdraws (4) / Flexion (3) / Extension (2) / None (1)
- Total GCS: ___ /15
- Trend: Improving / Stable / Declining
Focal Deficits (depend on location of depression)
- Frontal: Motor weakness (contralateral), personality change, expressive aphasia (dominant hemisphere)
- Parietal: Sensory deficit (contralateral), neglect (non-dominant), receptive language difficulty
- Temporal: Receptive aphasia (dominant — Wernicke area), visual field cut
- Occipital: Visual field deficit (contralateral hemianopia)
- Motor strip / central sulcus: Contralateral weakness in specific distribution
Open vs Closed Fracture Assessment
- Inspect wound: scalp laceration communicating with fracture fragments
- Visible bone / brain / CSF in wound = open fracture
- Palpable step-off (closed fracture — do not probe aggressively)
- Foreign material, hair, debris in wound (contamination grade)
- Active CSF leak from wound (dural violation)
Cranial Nerve Exam
- Pupillary exam: Baseline before anesthesia
- All cranial nerves: Document baseline (especially if near skull base)
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: trauma craniotomy/craniectomy tray, rapid blood availability, suction/bipolar/hemostatics, dural substitute, bone-flap storage or plating plan, ICP monitor/EVD supplies, and postop CT pathway cleared.
- Special needs: reversal of anticoagulants, seizure prophylaxis, hyperosmolar therapy plan, arterial line, Foley, temperature/glucose/coagulation targets, antibiotic/tetanus plan for open injuries, and family/ICU handoff.
- Immediate postop orders: ICU neuro checks, BP/CPP/ICP goals when monitored, CT head timing, drain/EVD settings, seizure prophylaxis duration, antibiotics for open/contaminated injuries, DVT prophylaxis timing, and repeat labs/coags.
Diagnosis & Indication
- Working diagnosis: [Open (compound) / Closed] depressed skull fracture of the [location]
- Surgical indication: Open depressed fracture (urgent — debride, prevent infection), depression > thickness of skull, underlying mass lesion, dural laceration/CSF leak, gross cosmetic deformity, neurological deficit, frontal sinus involvement
- Closed depressed fracture without dural breach/deficit can sometimes be managed conservatively
- Caution: Depressed fracture over a major venous sinus — elevation may cause torrential bleeding (prep, blood available, consider leaving depressed if asymptomatic and sinus intact)
Open vs Closed Fracture Management Differences
| Feature | Open (compound) | Closed |
|---|---|---|
| Timing | Urgent (within 24h; earlier if contaminated) | Semi-elective if stable |
| Antibiotics | Broad-spectrum empiric + wound culture | Standard surgical prophylaxis only |
| Debridement | Required — excise devitalized scalp, remove debris | Minimal |
| Bone fragments | Discard if grossly contaminated or comminuted | Replace if single fragment, clean edges |
| Dural repair | Mandatory watertight closure if violated | Repair if torn |
| Infection risk | High (meningitis, abscess, osteomyelitis) | Low |
| Cranioplasty | Often delayed (6-12 months) if bone discarded | Primary replacement typical |
Antibiotic Protocol for Open Fractures
- Empiric: Cefazolin 2g IV (vancomycin if MRSA concern or penicillin allergy)
- Contaminated wound (soil, organic material): Add metronidazole 500 mg IV or gentamicin
- Duration: 48-72h for clean open fractures; 7-14 days if heavily contaminated
- Obtain wound culture before starting antibiotics when possible
Timing of Surgery
- Open fracture: Urgent — within 24 hours (sooner if heavily contaminated, CSF leak, or neurological deterioration)
- Closed fracture with indication: Semi-elective; within 24-48 hours
- Mass lesion / declining GCS: Emergent
Position
- Per location, Mayfield or horseshoe; head positioned with fracture site up and accessible
- Slight reverse Trendelenburg for venous drainage
- Pressure points: All padded
- Arms: Tucked at sides
Key Surgical Steps
- Wound debridement (open fractures): Excise devitalized scalp edges (minimal — preserve vascularity), remove gross contamination, hair, foreign material; extend laceration if needed for adequate exposure
- Incision planning: Use existing laceration if adequate; otherwise curvilinear incision centered on the fracture with adequate margins in normal bone
- Craniotomy / burr hole placement: Place burr hole(s) in normal bone adjacent to the depressed segment — never through the fractured fragments; use craniotome to create a rim of craniotomy around the depressed area
- Elevation of depressed fragments: Using a periosteal elevator or Penfield dissector, carefully lever fragments upward from the adjacent craniotomy edge; avoid plunging — the dura and cortex are directly beneath; apply upward force only, never push inward
- Dural inspection: Examine dura under the entire depressed area; document intact vs lacerated
- Dural repair (if lacerated): Primary repair with 4-0 Nurolon if edges approximate; dural substitute graft (DuraGen, AlloDerm, pericranium) if defect too large; watertight closure mandatory; apply dural sealant (DuraSeal)
- Evacuate underlying hematoma / foreign material: Remove epidural or subdural clot if present; debride contused brain only if necrotic/pulped; remove indriven bone fragments, hair, debris under direct visualization
- Copious irrigation: Normal saline (open injuries — minimum 1-2 L)
- Fragment management:
- Clean, single fragments (closed or minimally contaminated open): Replace and fix with titanium microplates/screws
- Contaminated or comminuted fragments: Discard; plan delayed cranioplasty
- Fragments over a venous sinus: May leave in place if sinus intact and removal risks hemorrhage
- Frontal sinus involvement: If posterior wall fractured — cranialization (strip mucosa, plug nasofrontal duct with muscle/bone) or obliteration
- Cranioplasty options for bone loss: Titanium mesh (immediate if clean), custom implant (PEEK, titanium — delayed), methylmethacrylate, autologous split calvarial graft; delayed reconstruction preferred if infection concern
- Sinus bleeding: Control with Gelfoam, Surgicel, packing, or repair; may leave fragment over patent sinus if removal risks exsanguination
- Closure: Galea with 3-0 Vicryl, skin with staples or nylon; subgaleal drain if large dead space; do not close contaminated wounds under tension
Critical Anatomy & Structures at Risk
- Dura and underlying cortex — laceration, contusion, indriven bone fragments
- Dural venous sinuses (superior sagittal, transverse, sigmoid) — major hemorrhage if fragment elevated off sinus
- Frontal sinus (anterior fractures) — mucocele, ascending infection if not addressed
- Middle meningeal artery — may be lacerated by fracture; epidural hematoma source
- Cortical veins — at risk during fragment elevation and dural repair
- Eloquent cortex — motor strip, language areas (location-dependent)
Equipment
- Craniotome, high-speed drill, perforator
- Periosteal elevators (Penfield, Freer), Kerrison rongeurs
- Dural substitute (DuraGen, AlloDerm, pericranial graft)
- Dural sealant (DuraSeal, Tisseel)
- Cranial fixation (titanium microplates/screws, mesh)
- Hemostatic agents (Surgicel, Gelfoam, Floseal, bone wax)
- Copious irrigation (NS, bulb syringe or pulse lavage)
- Debridement instruments (curettes, rongeurs, forceps)
- Raney clips for scalp hemostasis
Anesthesia
- Cefazolin 2g IV (broad-spectrum if open — see antibiotic protocol above)
- Tetanus prophylaxis (Td/Tdap ± TIG for open fractures)
- Blood available (type and crossmatch; have in room if fracture over sinus)
- Levetiracetam 1000 mg IV (seizure prophylaxis — cortical injury)
- Mannitol 1 g/kg available if elevated ICP or brain swelling
- RSI if trauma / full stomach
Potential Complications
- Infection (open injuries) — meningitis, brain abscess, osteomyelitis, wound infection; debridement, antibiotics, discard contaminated bone
- Venous sinus hemorrhage — torrential bleeding if fragment elevated off sinus; have blood products, hemostatic agents, and packing ready
- Sinus thrombosis — can occur from sinus compression or surgical manipulation
- Seizures — cortical injury/irritation; prophylaxis indicated
- CSF leak — inadequate dural repair; may require re-exploration or lumbar drain
- Cosmetic deformity — inadequate elevation or bone loss requiring delayed cranioplasty
- Frontal sinus mucocele — late complication if sinus not properly cranialized
- Growing skull fracture (pediatric) — dural tear + growing brain herniates through fracture; presents months later with enlarging palpable defect; requires dural repair and cranioplasty
Operative Note Template
Preoperative Diagnosis: [Open (compound)/Closed] depressed skull fracture of the [left/right] [frontal/parietal/temporal/occipital] region [± dural laceration / underlying hematoma / frontal sinus involvement]
Postoperative Diagnosis: Same [or updated findings]
Procedure: Craniotomy for elevation of depressed skull fracture [with debridement / dural repair / cranioplasty / frontal sinus cranialization]
Surgeon: Assistant: Anesthesia: General endotracheal anesthesia
EBL: Fluids: Specimens: [Bone fragments / wound culture / none] Drains: [Subgaleal drain / none] Complications: None Implants: [Titanium microplates and screws / titanium mesh / dural graft / none]
Indications: The patient is a [age]yo [M/F] who presented following [mechanism] with [scalp laceration and palpable depressed fracture / focal deficit / GCS ]. CT head demonstrated a [open/closed] depressed skull fracture of the [left/right] [location], depressed [ mm / greater than one full table thickness] beyond the inner table [with underlying contusion / epidural hematoma / pneumocephalus / frontal sinus involvement]. [Open compound fracture with contamination risk.] Given [depression depth / open fracture / dural violation / deficit / cosmetic deformity], surgical elevation and debridement were indicated. Risks (infection, hemorrhage, seizure, CSF leak, cranioplasty) discussed with [patient / family]; consent obtained. [Anticoagulation reversed with ___.] Antibiotics, tetanus, and seizure prophylaxis administered.
Description of Procedure: After informed consent was verified and the surgical site was confirmed, the patient was brought to the operating room. General endotracheal anesthesia was induced [via rapid sequence induction]. An arterial line, Foley catheter, and two large-bore IVs were placed. Preoperative cefazolin [2g IV] [and metronidazole 500 mg IV], levetiracetam [1000 mg IV], and [tetanus prophylaxis] were administered.
The patient was positioned [supine/lateral] with the head rotated to place the [location] fracture site uppermost. The head was secured in a [Mayfield skull clamp / horseshoe headrest]. All pressure points were padded. A time-out was performed. The [left/right] [region] was prepped and draped in standard sterile fashion.
[The scalp laceration was debrided — devitalized wound edges excised, gross contamination removed, and wound culture obtained.] [For closed fractures: A curvilinear scalp incision was made centered over the fracture.] Burr holes were placed in normal bone adjacent to the depressed segment. A craniotomy was performed with the craniotome, creating a rim of bone removal around the depressed area. The depressed fragment(s) were carefully elevated using a periosteal elevator, applying upward force only. [The fragment was a single piece / multiple comminuted fragments were encountered.]
The dura was inspected under the entire depressed area and found to be [intact / lacerated]. [A __ cm dural laceration was repaired primarily with 4-0 Nurolon / repaired with a [pericranial / DuraGen] graft secured with 4-0 Nurolon sutures. Dural sealant was applied.] [The underlying cortex was intact / an underlying contusion was debrided / an epidural hematoma of __ mL was evacuated.] The field was copiously irrigated with normal saline.
[The bone fragment was clean and replaced in anatomic position with titanium microplates and screws. / The fragments were contaminated and comminuted — discarded; delayed cranioplasty planned. / Titanium mesh was contoured and secured over the defect.] [The frontal sinus mucosa was stripped, nasofrontal duct plugged, and sinus cranialized.] [A subgaleal drain was placed.] The galea was closed with 3-0 Vicryl, skin with [staples / nylon]. A sterile dressing was applied.
The patient was awakened, extubated [/ remained intubated], and found to be [following commands / GCS ___]. Transferred to the [ICU / floor] in stable condition.
Postoperative Plan
- ICU or floor admission per injury severity and GCS
- Neuro checks q1h x 24h (GCS, pupils, focal deficits)
- HOB 30 degrees
- CT head postop within 6 hours (confirm fragment elevation, assess for new/expanding hematoma, pneumocephalus)
- Antibiotics:
- Closed fracture: Standard perioperative prophylaxis only (cefazolin x 24h)
- Open fracture (clean): IV antibiotics x 48-72 hours (cefazolin)
- Open fracture (contaminated): IV antibiotics x 7-14 days; tailor to wound culture results; infectious disease consultation for heavily contaminated wounds
- Monitor for infection: fever, wound erythema, CSF leak, meningismus
- Tetanus prophylaxis: Confirm Td/Tdap ± TIG administered (open fractures)
- Seizure prophylaxis: Levetiracetam 500 mg BID x 7 days (Temkin criteria — cortical injury from depressed fracture; consider extending to 6 months if cortical laceration or hemorrhagic contusion; late seizures may warrant long-term AEDs)
- Wound care: Keep dressing clean and dry x 48h; inspect wound daily; staple/suture removal at 10-14 days; for contaminated wounds, monitor closely for dehiscence and purulent drainage
- DVT prophylaxis: SCDs immediately; pharmacologic (heparin SQ) starting POD1 after stable follow-up CT
- Pain management: Acetaminophen scheduled, opioids PRN; avoid NSAIDs x 48h
- Follow-up imaging: CT head before discharge; repeat CT at 4-6 weeks in clinic; MRI if concern for abscess or evolving contusion
- Late complications to monitor:
- Growing skull fracture (pediatric < 3 years): Dural tear → leptomeningeal cyst herniates through fracture → enlarging palpable defect over weeks-months; requires dural repair and cranioplasty
- Infection: Osteomyelitis, empyema, brain abscess — may present weeks post-op; CT/MRI with contrast if fever or declining exam
- CSF leak: Persistent wound drainage or rhinorrhea (frontal sinus); may require re-exploration or lumbar drain
- Post-traumatic epilepsy: Risk elevated with dural penetration and cortical injury; counsel on driving restrictions
- Delayed cranioplasty: If bone not replaced — reconstruct at 6-12 months (PEEK, titanium, or autologous graft); helmet precautions interim
- Follow-up: Clinic 2-4 weeks with wound check + CT; 3 and 6 months for delayed complications
Chief-Level Case Review
Use these as the senior-level mental model for Depressed Skull Fracture Elevation:
- Decision point: Treat physiology while preparing the room: airway, reversal, transfusion, ICP/CPP, sodium/osmolality, temperature, and repeat imaging drive timing as much as the scan finding.
- Technical lever: Know the operative priority: decompression, hemorrhage control, debridement, dural closure, reconstruction, stabilization, or contamination control.
- Bailout: Plan for swelling and coagulopathy: bone flap decision, duraplasty size, drain/EVD need, hemostatic adjuncts, and ICU handoff should be decided early.
- Postop watch: Postop failure modes are predictable: expanding hematoma, malignant edema, seizure, infection, CSF leak, venous sinus injury, and missed associated spine/vascular injury.
Common Pimp Questions
Use these to pressure-test preparation for Depressed Skull Fracture Elevation:
- What is the life-threatening mass-effect problem and what is the operative endpoint?
- What anticoagulant/antiplatelet reversal and blood-product plan is required before incision?
- What exposure gives rapid control while preserving options for expansion?
- What ICP, seizure, sodium, ventilation, and blood-pressure targets matter immediately postop?
- What injury pattern or associated lesion would change the incision, bone flap, or disposition?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Bone flap replacement versus decompressive storage threshold: [attending-specific]
- Preferred hemostatic agents, dural substitute, tack-up pattern, and drain use: [attending-specific]
- ICP monitor/EVD threshold, sodium target, seizure prophylaxis, and repeat CT timing: [attending-specific]
- Reversal product sequence and postop anticoagulation/DVT timing: [attending-specific]