
Case Prep: Awake Craniotomy with Cortical/Subcortical Mapping
Case / Approach Snapshot
- Anatomy at risk: target nuclei or cortical regions, trajectories, vessels, ventricles, cranial nerves, white-matter tracts, and stimulation/lesion side-effect pathways.
- Operative steps: confirm diagnosis and target, plan trajectory or exposure, use mapping/monitoring/stereotaxy as appropriate, place/lesion/resect with physiologic confirmation, close hardware or wound, and plan programming/follow-up; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: hemorrhage, seizure, neurologic or mood/cognitive change, lead/device migration or infection, stimulation side effects, hardware failure, and revision or programming strategy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [left/right] [location] lesion involving/adjacent to [eloquent language/motor cortex] planned for awake craniotomy with intraoperative brain mapping for maximal safe resection.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Awake surgery with cortical-subcortical mapping in diffuse gliomas adjacent to central lobe. Report of two cases and literature review — Núñez-Velasco S. Cirugia y cirujanos 2019. PubMed
- A Review of Cortical and Subcortical Stimulation Mapping for Language — Young JS. Neurosurgery 2021. PubMed
- Awake brain mapping of cortex and subcortical pathways in brain tumor surgery — Freyschlag CF. Journal of neurosurgical sciences 2014. PubMed
- White matter tracts and executive functions: a review of causal and correlation evidence — Ribeiro M. Brain : a journal of neurology 2024. PubMed
- Awake brain mapping by direct cortical stimulation; technical note to get higher resection rate and low morbidity in low-grade glioma patients — Ahmed Khan R. Annals of medicine and surgery (2012) 2024. PubMed
- Awake Craniotomy with Cortical and Subcortical Speech Mapping for Supramarginal Cavernoma Resection — Domingo RA. World neurosurgery 2020. PubMed
- [Awake neurosurgery: usefullness of intraoperative cortical and subcortical functional mapping] — Mikuni N. No shinkei geka. Neurological surgery 2004. PubMed
- Surgery for gliomas — Tate MC. Cancer treatment and research 2015. PubMed
- Functional cortical mapping and structural subcortical anatomy predicts intra-operative speech arrest: a nTMS-tractography study — Jung J. Clinical neurophysiology : official journal of the International Federation of Clinical Neurophysiology 2025. PubMed
- Intraoperative augmented reality fiber tractography complements cortical and subcortical mapping — Chidambaram S. World neurosurgery: X 2023. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
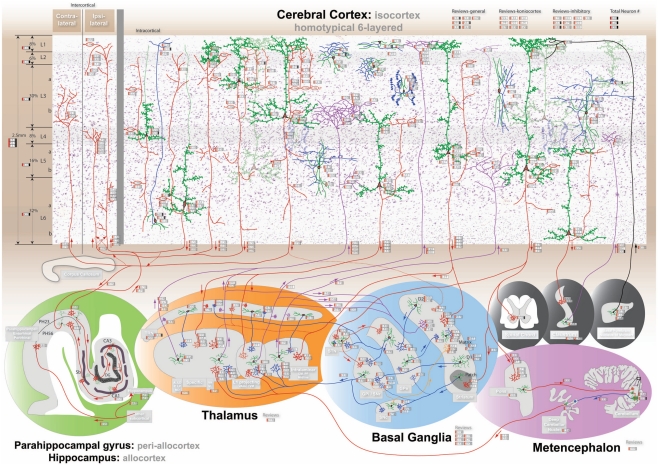 Figure 1. The comprehensive neuroanatomical picture formed by synthesizing hundreds of original neuroanatomical studies into the homotypical blueprint underlying cognition. The interactive… Source: Cognitive Consilience: Primate Non-Primary Neuroanatomical Circuits Underlying Cognition — Frontiers in Neuroanatomy 2011; CC BY-NC.
Figure 1. The comprehensive neuroanatomical picture formed by synthesizing hundreds of original neuroanatomical studies into the homotypical blueprint underlying cognition. The interactive… Source: Cognitive Consilience: Primate Non-Primary Neuroanatomical Circuits Underlying Cognition — Frontiers in Neuroanatomy 2011; CC BY-NC.
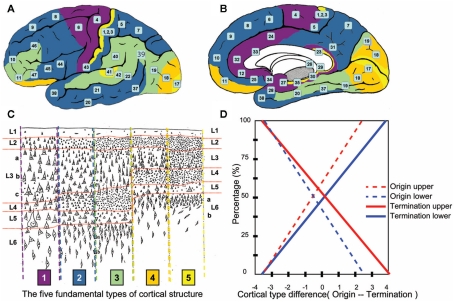 Figure 3. Prediction of human laminar corticocortical projections. Synthesis of von Economo cortical laminar types and homotypical laminar corticocortical projections in the monkey. Lateral (A)… Source: Cognitive Consilience: Primate Non-Primary Neuroanatomical Circuits Underlying Cognition — Frontiers in Neuroanatomy 2011; CC BY-NC.
Figure 3. Prediction of human laminar corticocortical projections. Synthesis of von Economo cortical laminar types and homotypical laminar corticocortical projections in the monkey. Lateral (A)… Source: Cognitive Consilience: Primate Non-Primary Neuroanatomical Circuits Underlying Cognition — Frontiers in Neuroanatomy 2011; CC BY-NC.
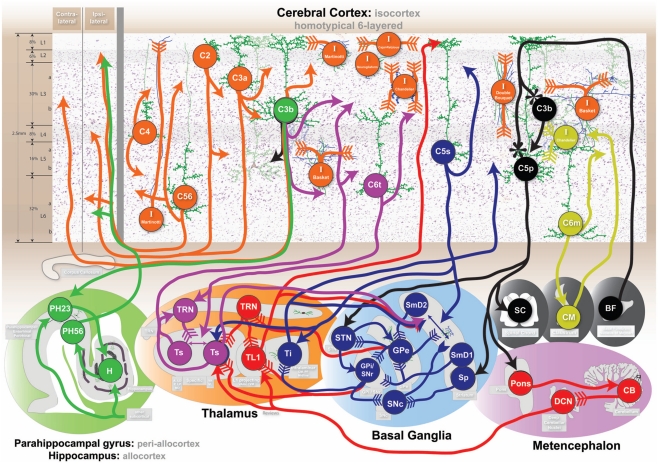 Figure 4. Cognitive circuits as shown at http://www.frontiersin.org/files/cognitiveconsilience/index.html. Circuits from left to right. Orange: consolidated declarative long-term memory. Green:… Source: Cognitive Consilience: Primate Non-Primary Neuroanatomical Circuits Underlying Cognition — Frontiers in Neuroanatomy 2011; CC BY-NC.
Figure 4. Cognitive circuits as shown at http://www.frontiersin.org/files/cognitiveconsilience/index.html. Circuits from left to right. Orange: consolidated declarative long-term memory. Green:… Source: Cognitive Consilience: Primate Non-Primary Neuroanatomical Circuits Underlying Cognition — Frontiers in Neuroanatomy 2011; CC BY-NC.
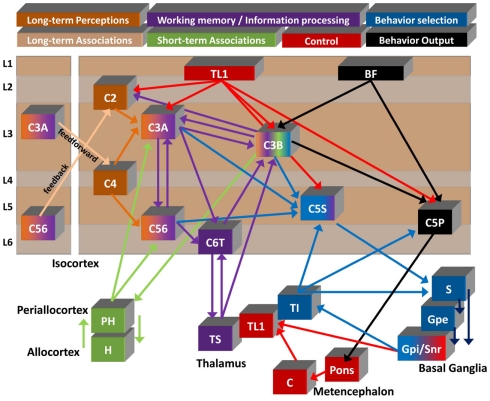 Figure 5. Summary diagram of proposed flow of cognitive information. Seven of the circuits described in the text are shown to illustrate a summarized functional viewpoint of the hypothesized flow… Source: Cognitive Consilience: Primate Non-Primary Neuroanatomical Circuits Underlying Cognition — Frontiers in Neuroanatomy 2011; CC BY-NC.
Figure 5. Summary diagram of proposed flow of cognitive information. Seven of the circuits described in the text are shown to illustrate a summarized functional viewpoint of the hypothesized flow… Source: Cognitive Consilience: Primate Non-Primary Neuroanatomical Circuits Underlying Cognition — Frontiers in Neuroanatomy 2011; CC BY-NC.
 Figure 5. Source: Cognitive Profiles and Determinants of Eligibility for Awake Surgery in Non‐Dominant Hemisphere Gliomas: A Narrative Review — Brain Behav. 2025 May 30;15(6):e70604. doi: 10.1002/brb3.70604; CC BY.
Figure 5. Source: Cognitive Profiles and Determinants of Eligibility for Awake Surgery in Non‐Dominant Hemisphere Gliomas: A Narrative Review — Brain Behav. 2025 May 30;15(6):e70604. doi: 10.1002/brb3.70604; CC BY.
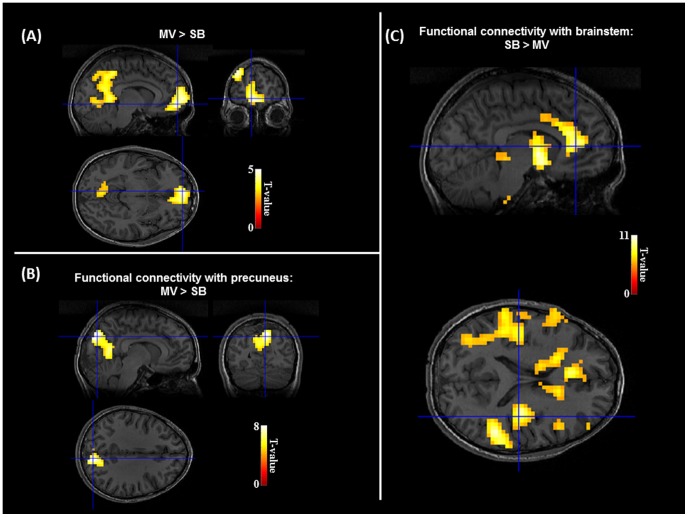 Figure 2. Restoration of DMN under mechanical ventilation.(A). Comparison of BOLD signal between MV and SB revealed a specific increase of activation in the default-mode network associated in… Source: The Cerebral Cost of Breathing: An fMRI Case-Study in Congenital Central Hypoventilation Syndrome — PLoS ONE 2014; CC0.
Figure 2. Restoration of DMN under mechanical ventilation.(A). Comparison of BOLD signal between MV and SB revealed a specific increase of activation in the default-mode network associated in… Source: The Cerebral Cost of Breathing: An fMRI Case-Study in Congenital Central Hypoventilation Syndrome — PLoS ONE 2014; CC0.
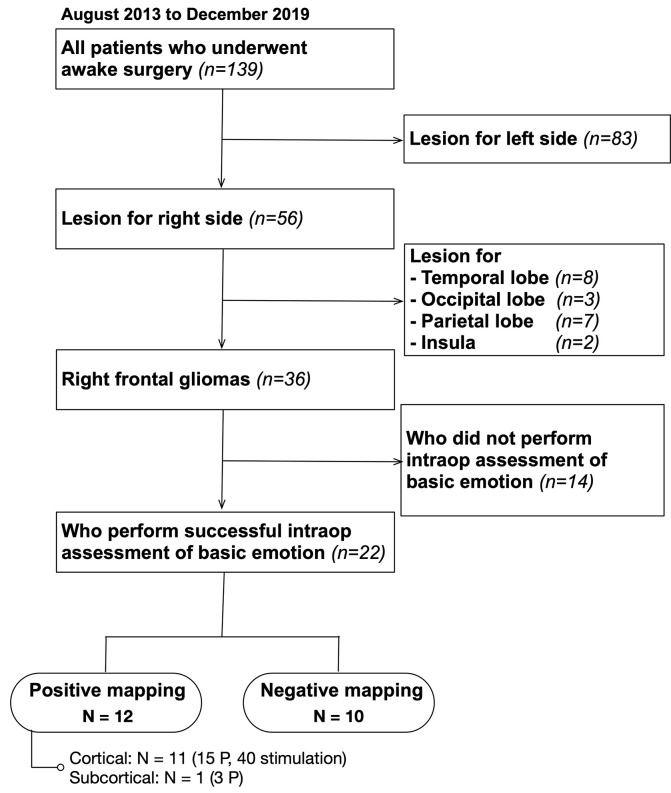 Figure 1. Inclusion criteria. A total of 139 patients who underwent awake surgery in our institution were included; 36 of them matched our inclusion criteria. Of these, 22 patients underwent… Source: Preserving Right Pre-motor and Posterior Prefrontal Cortices Contribute to Maintaining Overall Basic Emotion — Frontiers in Human Neuroscience 2021; CC BY.
Figure 1. Inclusion criteria. A total of 139 patients who underwent awake surgery in our institution were included; 36 of them matched our inclusion criteria. Of these, 22 patients underwent… Source: Preserving Right Pre-motor and Posterior Prefrontal Cortices Contribute to Maintaining Overall Basic Emotion — Frontiers in Human Neuroscience 2021; CC BY.
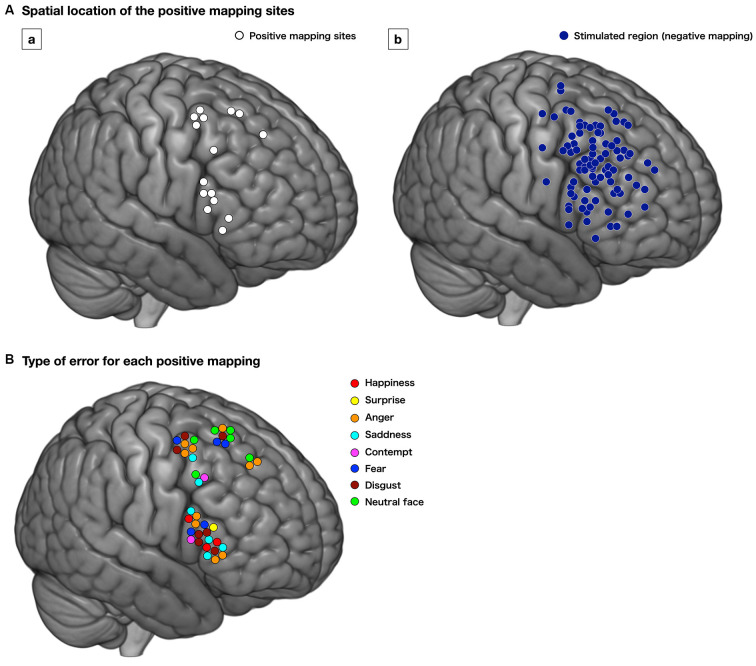 Figure 3. Distribution of the positive mapping sites (Aa, white circle) and regions with negative responses (Ab, dark blue circle) at the cortical level. Each positive mapping site is stimulated… Source: Preserving Right Pre-motor and Posterior Prefrontal Cortices Contribute to Maintaining Overall Basic Emotion — Frontiers in Human Neuroscience 2021; CC BY.
Figure 3. Distribution of the positive mapping sites (Aa, white circle) and regions with negative responses (Ab, dark blue circle) at the cortical level. Each positive mapping site is stimulated… Source: Preserving Right Pre-motor and Posterior Prefrontal Cortices Contribute to Maintaining Overall Basic Emotion — Frontiers in Human Neuroscience 2021; CC BY.
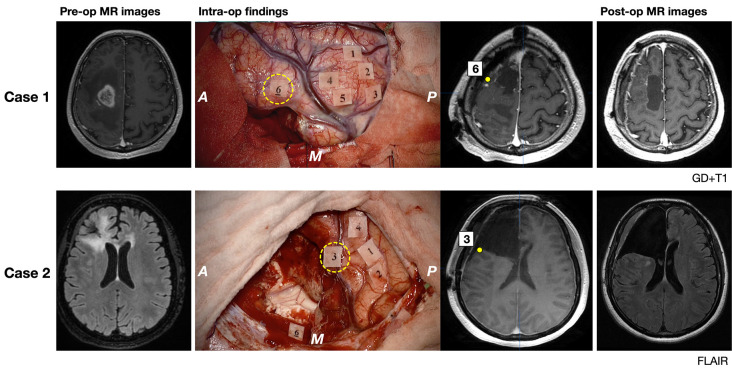 Figure 6. Pre- and postoperative magnetic resonance (MR) images (gadolinium-enhanced T1 image for Case 1 and FLAIR image for Case 2) and intraoperative findings of illustrative two cases are… Source: Preserving Right Pre-motor and Posterior Prefrontal Cortices Contribute to Maintaining Overall Basic Emotion — Frontiers in Human Neuroscience 2021; CC BY.
Figure 6. Pre- and postoperative magnetic resonance (MR) images (gadolinium-enhanced T1 image for Case 1 and FLAIR image for Case 2) and intraoperative findings of illustrative two cases are… Source: Preserving Right Pre-motor and Posterior Prefrontal Cortices Contribute to Maintaining Overall Basic Emotion — Frontiers in Human Neuroscience 2021; CC BY.
History of Present Illness
- Chief complaint: Lesion (glioma, metastasis, cavernoma, epileptogenic focus) in/near eloquent cortex
- Indication for awake: dominant-hemisphere language area, primary motor cortex, insula, or any eloquent-adjacent lesion where real-time functional feedback maximizes safe resection
- Patient cooperation essential — assess ability to tolerate awake phase (anxiety, claustrophobia, cognitive/language baseline, airway)
- Handedness/language dominance
Imaging Review
MRI + fMRI + DTI
- Lesion location relative to eloquent cortex (fMRI: language, motor)
- DTI tractography: corticospinal tract, arcuate fasciculus, IFOF, SLF
- Navigation planning
Labs
- CBC, BMP, Coags, Type and screen
Neurological Examination
- Detailed baseline language (fluency, naming, comprehension, repetition, reading), motor, cognition — establishes the testing baseline and tasks
- Pre-op session with neuropsychologist/speech therapist to rehearse intraoperative tasks
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: mapping cart, neuropsych/language team, ECoG/stimulation equipment, navigation/DTI, microscope, airway plan for asleep-awake-asleep when used, and bailout conversion-to-GA plan.
- Special needs: antiepileptic continuation/loading plan, steroid plan if edema risk, nausea/pain regimen that preserves exam, seizure rescue medications, and clear baseline language/motor/visual-field documentation.
- Immediate postop orders: frequent neuro checks focused on mapped functions, seizure precautions, AED orders, CT/MRI timing, steroid taper if used, visual-field/language assessment, and rehab/neuropsych follow-up.
Diagnosis & Indication
- Goal: Maximal safe resection defined by functional boundaries (positive mapping sites), not just anatomic margins
Anesthetic Technique
- Asleep-Awake-Asleep (AAA) or Monitored Anesthesia Care (conscious sedation throughout)
- Scalp block (regional anesthesia: supraorbital, supratrochlear, auriculotemporal, zygomaticotemporal, greater/lesser occipital nerves) — key to comfort
Position
- Lateral or supine with head turned; comfortable, face visible/accessible to the mapping team; airway accessible; padded; not fully rigid feeling
- Mayfield (pin sites infiltrated with local)
Key Surgical Steps
- Asleep phase (if AAA): induce, LMA/airway, position, scalp block, craniotomy
- Open dura (infiltrate dura/middle meningeal with local — dura is pain-sensitive)
- Awaken patient, remove airway, confirm comfort and task performance
- Cortical mapping (bipolar stimulator, e.g., 50-60 Hz, escalating mA; or high-frequency):
- Motor: stimulation → contralateral movement (or interrupts movement)
- Language: patient counts/names/reads while stimulating → speech arrest, anomia, paraphasia, dysarthria mark eloquent sites
- Tag positive sites; ECoG to detect afterdischarges/stimulation-induced seizures
- Resection within functional boundaries, with continuous subcortical mapping and ongoing language/motor testing
- Stop at positive subcortical tracts (corticospinal → motor response; arcuate/IFOF → language errors)
- Monitor patient continuously; resect to functional (not just anatomic) limits
- [Re-sedate for closure if AAA]; hemostasis, closure
Critical Anatomy & Structures at Risk
- Language network — Broca, Wernicke, arcuate fasciculus, IFOF, SLF
- Motor cortex / corticospinal tract
- Vasculature (MCA branches), draining veins
Equipment
- Microscope, navigation (fMRI/DTI), CUSA, ultrasound, 5-ALA (HGG)
- Cortical/subcortical bipolar stimulator, ECoG, sterile mapping tags
- Mapping team (neuropsychologist/SLP), task materials (naming cards, screen)
Monitoring
- Direct cortical & subcortical stimulation, continuous clinical testing, ECoG
Anesthesia
- Scalp block, dexmedetomidine ± propofol/remifentanil (titratable, awake on demand), antiemetics (ondansetron), Foley
- Seizure management plan: iced saline to cortex, low-dose propofol/midazolam, antiepileptics
- Airway backup plan (LMA/intubation if needed); avoid oversedation/respiratory depression during awake phase
Potential Complications
- Intraoperative seizure (stimulation-induced) — cold saline, benzodiazepine/propofol
- New/worsened language or motor deficit (often transient if functional boundaries respected)
- Patient intolerance/agitation, airway compromise, nausea/vomiting (aspiration risk)
- Brain swelling, venous air embolism (semi-sitting), hemorrhage
Operative Note Template
Preoperative Diagnosis: [Left/Right] [location] lesion involving/adjacent to eloquent [language/motor] cortex
Postoperative Diagnosis: Same (pending pathology)
Procedure: [Left/Right] awake craniotomy with cortical and subcortical mapping for resection of [lesion]
Surgeon / Assistant: + neuropsychologist/SLP for mapping Anesthesia: Asleep-awake-asleep [/ MAC] with scalp block EBL / Fluids: Adjuncts: Neuronavigation (fMRI/DTI), cortical/subcortical bipolar stimulator, ECoG, ultrasound, [5-ALA] Complications: None
Indications: [Age]yo [M/F] with a [lesion] in/near eloquent cortex; awake mapping was chosen to maximize safe resection by functional boundaries. The patient was assessed as able to tolerate the awake phase. Risks (seizure, deficit, intolerance) discussed.
Description of Procedure: After consent and time-out, [the asleep phase was induced with an airway, and] a scalp block placed; the craniotomy was performed and the dura opened (infiltrated with local). The patient was awakened and confirmed comfortable and performing tasks. Cortical mapping with the bipolar stimulator identified [language/motor] sites (speech arrest/anomia/motor response), tagged as positive, with ECoG monitoring for afterdischarges.
The lesion was resected within the functional boundaries with continuous subcortical mapping and ongoing testing, stopping at positive subcortical tracts ([corticospinal/arcuate/IFOF]). [Iced saline managed a stimulation-induced seizure.] The patient remained neurologically [intact/at functional baseline] throughout. [The patient was re-sedated for closure.]
Hemostasis was obtained and closure performed. The patient was transferred to the ICU; neuro checks were compared to the detailed baseline.
Postoperative Plan
- ICU, neuro checks q1h — compare to detailed baseline (language, motor)
- MRI < 48h (EOR), CT if concern
- Expect possible transient deficit (e.g., SMA syndrome, transient aphasia) with recovery; speech/PT/OT
- Steroid taper, AEDs, DVT prophylaxis
- Pathology/molecular; tumor board; rehab referral
Chief-Level Case Review
Use these as the senior-level mental model for Awake Craniotomy with Cortical/Subcortical Mapping:
- Decision point: Define the symptom physiology: target circuit or offending vessel/nerve must match the history, exam, imaging, and intraoperative monitoring plan.
- Technical lever: Small errors matter: trajectory, lead/contact position, arachnoid dissection, cranial-nerve handling, or mapping threshold can be the difference between success and morbidity.
- Bailout: Have a stop rule: unacceptable mapping response, BAER/MEP/SSEP change, hemorrhage, CSF loss, poor target confidence, or patient intolerance should trigger a defined pivot.
- Postop watch: Postop success requires programming/follow-up details: neurologic exam, imaging, medication adjustment, device restrictions, wound care, and symptom-specific outcome tracking.
Common Pimp Questions
Use these to pressure-test preparation for Awake Craniotomy with Cortical/Subcortical Mapping:
- What is the symptom target and what finding proves the correct neural structure is being treated?
- What imaging, tractography, MER, stimulation, or mapping information changes the trajectory?
- What medication adjustments or anesthesia constraints matter on the day of surgery?
- What complication would be subtle but important to detect in recovery?
- What postop programming, imaging, seizure, swallow, or cranial-nerve plan is needed?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Awake/asleep technique, MER/stimulation thresholds, and imaging confirmation: [attending-specific]
- Medication hold/restart protocol and programming timeline: [attending-specific]
- Hardware brand, tunneling side, battery pocket, and antibiotic envelope preference: [attending-specific]
- Postop CT/MRI timing and symptom-specific neuro checks: [attending-specific]