
Case Prep: Anterior Temporal Lobectomy / Selective Amygdalohippocampectomy (Epilepsy)
Case / Approach Snapshot
- Anatomy at risk: target nuclei or cortical regions, trajectories, vessels, ventricles, cranial nerves, white-matter tracts, and stimulation/lesion side-effect pathways.
- Operative steps: confirm diagnosis and target, plan trajectory or exposure, use mapping/monitoring/stereotaxy as appropriate, place/lesion/resect with physiologic confirmation, close hardware or wound, and plan programming/follow-up; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: hemorrhage, seizure, neurologic or mood/cognitive change, lead/device migration or infection, stimulation side effects, hardware failure, and revision or programming strategy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with medically refractory [left/right] mesial temporal lobe epilepsy (hippocampal sclerosis) planned for [left/right] anterior temporal lobectomy with amygdalohippocampectomy.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Anterior temporal lobectomy and selective AmygdaloHippocampectomy complications across Europe: review, meta-analysis, and Delphi consensus — Karagianni MD. Brain & spine 2025. PubMed
- An examination of seizure-free outcome and visual field deficits: Anterior temporal lobectomy versus selective amygdalohippocampectomy for temporal lobe epilepsy-a systematic review and meta-analysis for comprehensive understanding — Rangwala BS. Acta neurochirurgica 2024. PubMed
- Selective Amygdalohippocampectomy — Hoyt AT. Neurosurgery clinics of North America 2016. PubMed
- Comparisons of the seizure-free outcome and visual field deficits between anterior temporal lobectomy and selective amygdalohippocampectomy: A systematic review and meta-analysis — Xu K. Seizure 2020. PubMed
- Selective amygdalohippocampectomy versus anterior temporal lobectomy in the management of mesial temporal lobe epilepsy: a meta-analysis of comparative studies — Hu WH. Journal of neurosurgery 2013. PubMed
- Comparison of therapeutic effects between selective amygdalohippocampectomy and anterior temporal lobectomy for the treatment of temporal lobe epilepsy: a meta-analysis — Kuang Y. British journal of neurosurgery 2014. PubMed
- Selective amygdalohippocampectomy — Spencer D. Epilepsy research and treatment 2012. PubMed
- Selective amygdalohippocampectomy: the trans-middle temporal gyrus approach — Wheatley BM. Neurosurgical focus 2008. PubMed
- Visual outcomes after anterior temporal lobectomy and transsylvian selective amygdalohippocampectomy: A quantitative comparison of clinical and diffusion data — Pruckner P. Epilepsia 2023. PubMed
- Anterior temporal lobectomy versus selective amygdalohippocampectomy in patients with mesial temporal lobe epilepsy — Nascimento FA. Arquivos de neuro-psiquiatria 2016. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
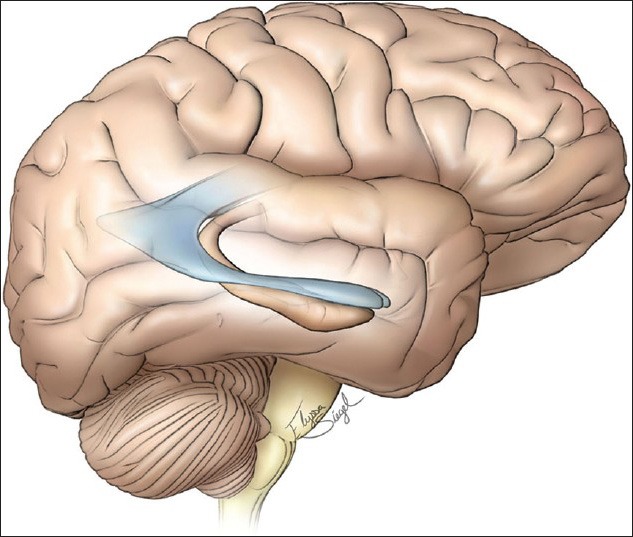 Figure 1. Schematic drawing of the typically noted position of the temporal horn. ©The Neurosurgical Atlas by Aaron A. Cohen-Gadol, MD, used with permission Source: External cortical landmarks and measurements for the temporal horn: Anatomic study with application to surgery of the temporal lobe — Surgical Neurology International 2015; CC BY-NC-SA.
Figure 1. Schematic drawing of the typically noted position of the temporal horn. ©The Neurosurgical Atlas by Aaron A. Cohen-Gadol, MD, used with permission Source: External cortical landmarks and measurements for the temporal horn: Anatomic study with application to surgery of the temporal lobe — Surgical Neurology International 2015; CC BY-NC-SA.
 Figure 2. Right-sided brain with pins in the anterior and posterior extent of the temporal horn Source: External cortical landmarks and measurements for the temporal horn: Anatomic study with application to surgery of the temporal lobe — Surgical Neurology International 2015; CC BY-NC-SA.
Figure 2. Right-sided brain with pins in the anterior and posterior extent of the temporal horn Source: External cortical landmarks and measurements for the temporal horn: Anatomic study with application to surgery of the temporal lobe — Surgical Neurology International 2015; CC BY-NC-SA.
 Figure 3. Left sided brain with pins marking the anterior and posterior extent of the temporal horn Source: External cortical landmarks and measurements for the temporal horn: Anatomic study with application to surgery of the temporal lobe — Surgical Neurology International 2015; CC BY-NC-SA.
Figure 3. Left sided brain with pins marking the anterior and posterior extent of the temporal horn Source: External cortical landmarks and measurements for the temporal horn: Anatomic study with application to surgery of the temporal lobe — Surgical Neurology International 2015; CC BY-NC-SA.
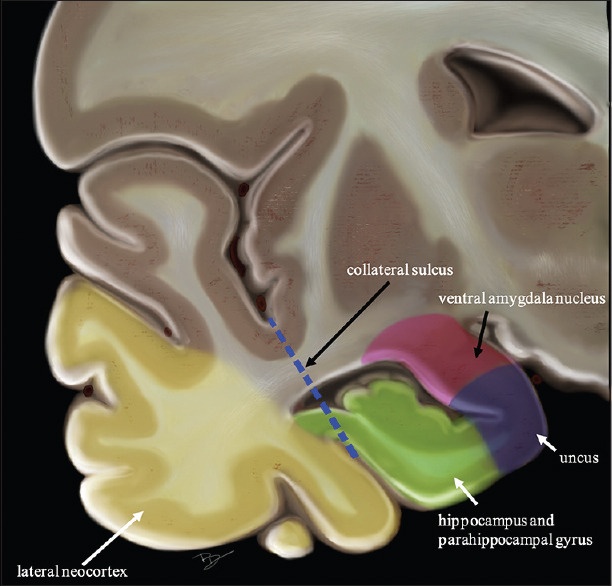 Figure 1. Coronal view of temporal lobe Source: Seizure Outcome after Lesionectomy With or Without Concomitant Anteromedial Temporal Lobectomy for Low-Grade Gliomas of the Medial Temporal Lobe — Asian Journal of Neurosurgery 2021; CC BY-NC-SA.
Figure 1. Coronal view of temporal lobe Source: Seizure Outcome after Lesionectomy With or Without Concomitant Anteromedial Temporal Lobectomy for Low-Grade Gliomas of the Medial Temporal Lobe — Asian Journal of Neurosurgery 2021; CC BY-NC-SA.
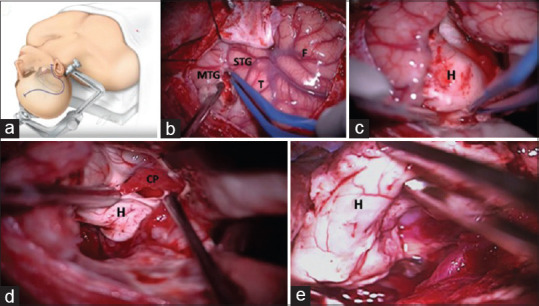 Figure 2. Operative steps of AMTR. Incision on superior temporal sulcus between superior and middle temporal Gyrus [Figure 2a,b]; tumor infiltrating hippocampus [Figure 2c]. Gross total excision… Source: Seizure Outcome after Lesionectomy With or Without Concomitant Anteromedial Temporal Lobectomy for Low-Grade Gliomas of the Medial Temporal Lobe — Asian Journal of Neurosurgery 2021; CC BY-NC-SA.
Figure 2. Operative steps of AMTR. Incision on superior temporal sulcus between superior and middle temporal Gyrus [Figure 2a,b]; tumor infiltrating hippocampus [Figure 2c]. Gross total excision… Source: Seizure Outcome after Lesionectomy With or Without Concomitant Anteromedial Temporal Lobectomy for Low-Grade Gliomas of the Medial Temporal Lobe — Asian Journal of Neurosurgery 2021; CC BY-NC-SA.
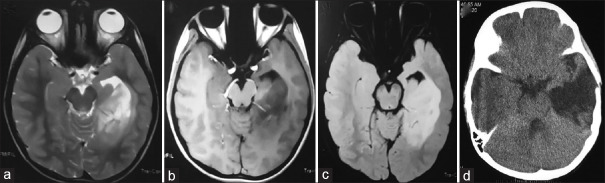 Figure 3. Magnetic resonance imaging (a-c) and computed tomography (d) of ganglioneuroma operated by AMTR with gross total excision Source: Seizure Outcome after Lesionectomy With or Without Concomitant Anteromedial Temporal Lobectomy for Low-Grade Gliomas of the Medial Temporal Lobe — Asian Journal of Neurosurgery 2021; CC BY-NC-SA.
Figure 3. Magnetic resonance imaging (a-c) and computed tomography (d) of ganglioneuroma operated by AMTR with gross total excision Source: Seizure Outcome after Lesionectomy With or Without Concomitant Anteromedial Temporal Lobectomy for Low-Grade Gliomas of the Medial Temporal Lobe — Asian Journal of Neurosurgery 2021; CC BY-NC-SA.
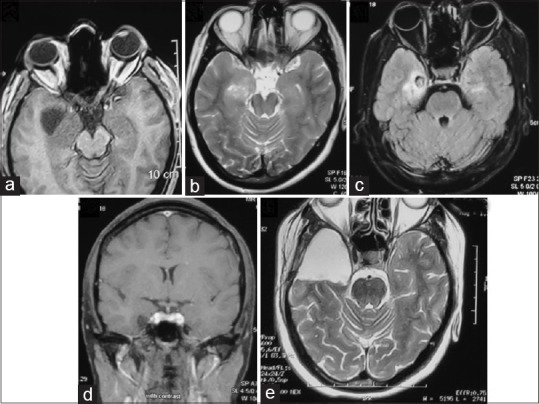 Figure 4. (a-e) Magnetic resonance imaging of a patient with medial temporal pilocytic astrocytoma operated by AMTR Source: Seizure Outcome after Lesionectomy With or Without Concomitant Anteromedial Temporal Lobectomy for Low-Grade Gliomas of the Medial Temporal Lobe — Asian Journal of Neurosurgery 2021; CC BY-NC-SA.
Figure 4. (a-e) Magnetic resonance imaging of a patient with medial temporal pilocytic astrocytoma operated by AMTR Source: Seizure Outcome after Lesionectomy With or Without Concomitant Anteromedial Temporal Lobectomy for Low-Grade Gliomas of the Medial Temporal Lobe — Asian Journal of Neurosurgery 2021; CC BY-NC-SA.
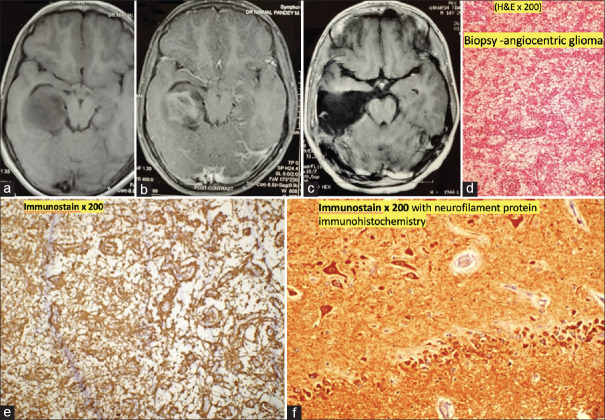 Figure 5. (a-c) The patient underwent AMTR. Histopathology showing mildly anisomorphic astrocytes around thin vascular spaces with microcystic degeneration (d). GFAP (Glial fibrillary acidic… Source: Seizure Outcome after Lesionectomy With or Without Concomitant Anteromedial Temporal Lobectomy for Low-Grade Gliomas of the Medial Temporal Lobe — Asian Journal of Neurosurgery 2021; CC BY-NC-SA.
Figure 5. (a-c) The patient underwent AMTR. Histopathology showing mildly anisomorphic astrocytes around thin vascular spaces with microcystic degeneration (d). GFAP (Glial fibrillary acidic… Source: Seizure Outcome after Lesionectomy With or Without Concomitant Anteromedial Temporal Lobectomy for Low-Grade Gliomas of the Medial Temporal Lobe — Asian Journal of Neurosurgery 2021; CC BY-NC-SA.
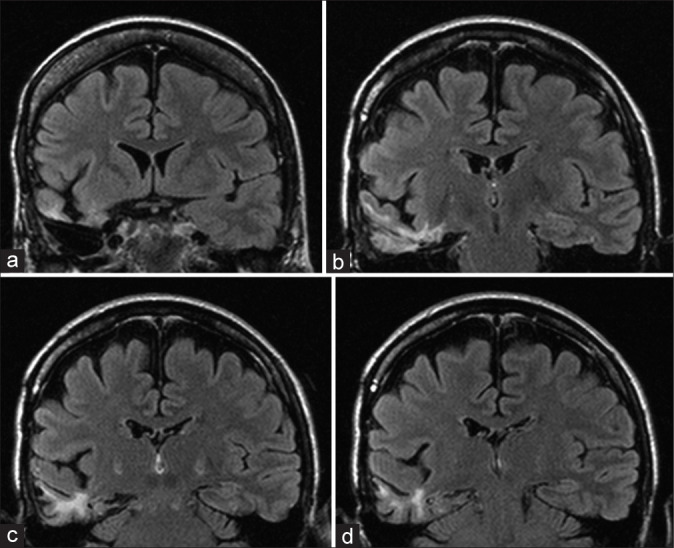 Figure 1:. (a-d) Gliotic changes in the temporal lobe with complete hippocampal resection in patient no. 6. Source: One-year neuropsychological outcome after temporal lobe epilepsy surgery in large Czech sample: Search for factors contributing to memory decline — Surgical Neurology International 2022; CC BY-NC-SA.
Figure 1:. (a-d) Gliotic changes in the temporal lobe with complete hippocampal resection in patient no. 6. Source: One-year neuropsychological outcome after temporal lobe epilepsy surgery in large Czech sample: Search for factors contributing to memory decline — Surgical Neurology International 2022; CC BY-NC-SA.
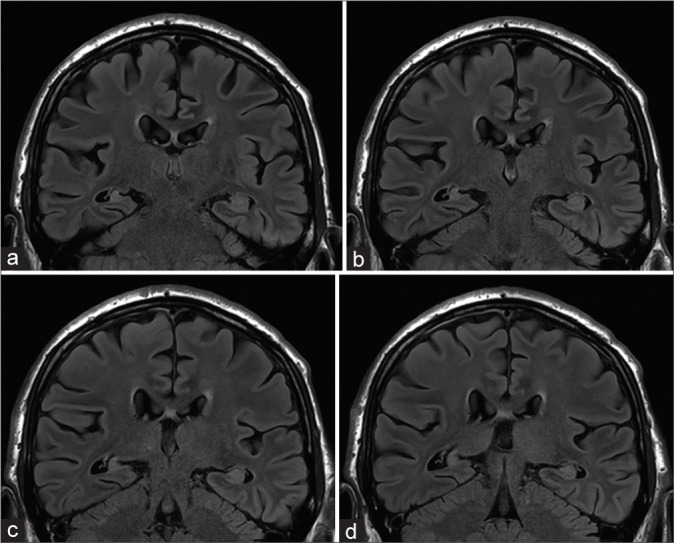 Figure 2:. (a-d) Hippocampal remnants after the right-sided anteromesial temporal resection in patient no. 2. Source: One-year neuropsychological outcome after temporal lobe epilepsy surgery in large Czech sample: Search for factors contributing to memory decline — Surgical Neurology International 2022; CC BY-NC-SA.
Figure 2:. (a-d) Hippocampal remnants after the right-sided anteromesial temporal resection in patient no. 2. Source: One-year neuropsychological outcome after temporal lobe epilepsy surgery in large Czech sample: Search for factors contributing to memory decline — Surgical Neurology International 2022; CC BY-NC-SA.
History of Present Illness
- Chief complaint: Drug-resistant focal epilepsy (failed ≥ 2 appropriate AEDs)
- Seizure semiology (aura — epigastric/déjà vu, automatisms, focal to bilateral tonic-clonic), frequency
- Comprehensive epilepsy workup completed:
- Video-EEG (ictal onset localization)
- MRI (hippocampal sclerosis)
- Neuropsychological testing
- PET/SPECT, MEG as needed
- Wada test or fMRI (language/memory lateralization — critical for dominant-side resection)
- Intracranial monitoring (SEEG/grids) if non-localizing
Imaging Review
MRI (epilepsy protocol — thin coronal hippocampal cuts, FLAIR)
- Hippocampal sclerosis — atrophy, T2/FLAIR hyperintensity
- Mesial temporal structures (amygdala, hippocampus, parahippocampus)
- Exclude other lesions (tumor, dysplasia, cavernoma)
- Vascular anatomy (MCA, anterior choroidal, PCA, basal vein), temporal horn
Functional
- Wada/fMRI (language and memory dominance)
- PET (temporal hypometabolism), ictal SPECT
Labs
- CBC, BMP, Coags, Type and screen
- AED levels
Neurological Examination
- Language (dominant side), memory, visual fields (Meyer’s loop risk), full exam
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: mapping cart, neuropsych/language team, ECoG/stimulation equipment, navigation/DTI, microscope, airway plan for asleep-awake-asleep when used, and bailout conversion-to-GA plan.
- Special needs: antiepileptic continuation/loading plan, steroid plan if edema risk, nausea/pain regimen that preserves exam, seizure rescue medications, and clear baseline language/motor/visual-field documentation.
- Immediate postop orders: frequent neuro checks focused on mapped functions, seizure precautions, AED orders, CT/MRI timing, steroid taper if used, visual-field/language assessment, and rehab/neuropsych follow-up.
Diagnosis & Indication
- Indication: Drug-resistant mesial temporal lobe epilepsy with concordant EEG/MRI/semiology
- Procedure choice: Anterior temporal lobectomy (ATL) with amygdalohippocampectomy, OR selective amygdalohippocampectomy (SAH) (spares lateral temporal neocortex — may better preserve naming/memory but similar seizure outcomes debated)
- Dominant side: limit lateral resection (language), Wada-guided
Position
- Supine, head rotated 60-90 degrees contralateral, slight extension, vertex down; Mayfield
Approach: Temporal Craniotomy
Key Surgical Steps (ATL)
- Question-mark/reverse-question-mark temporal incision, temporal craniotomy (low to middle fossa floor)
- Open dura, expose temporal lobe
- Lateral neocortical resection: measure from temporal tip — typically ~4-4.5 cm dominant, ~5-5.5 cm non-dominant along middle temporal gyrus (stay anterior to avoid Wernicke; limit superior temporal gyrus on dominant side)
- Subpial resection of superior/middle/inferior temporal gyri; enter the temporal horn of the lateral ventricle
- Identify ventricular landmarks: choroid plexus, choroidal fissure, hippocampus, collateral eminence
- Mesial resection: resect amygdala (anterior, up to level of choroidal point — avoid going superomedial into basal ganglia/optic tract), then hippocampus and parahippocampal gyrus
- Disconnect hippocampus posteriorly (en bloc or piecemeal), divide hippocampal/fimbrial attachments
- Preserve the pia over the medial structures protecting the brainstem, CN III, PCA, anterior choroidal artery, and basal vein in the ambient cistern
- Hemostasis, closure
Critical Anatomy & Structures at Risk
- Optic radiations / Meyer’s loop — superior/lateral resection → contralateral superior quadrantanopia (“pie in the sky”)
- Language cortex (dominant — Wernicke posterior, basal temporal language) — limit posterior/superior extent
- MCA branches (Sylvian), anterior choroidal & PCA, basal vein of Rosenthal (medial, ambient cistern)
- CN III, midbrain (medial — preserve pia)
- Memory (contralateral hippocampal reserve — Wada)
Equipment
- Microscope, navigation, CUSA, subpial dissection instruments, bipolar
- ECoG electrodes (optional intraoperative), ultrasonic aspirator
Monitoring
- Optional ECoG; awake language mapping if resection near dominant language cortex
Anesthesia
- Arterial line, AED continuation, standard; awake protocol if mapping
Potential Complications
- Visual field deficit (superior quadrantanopia — Meyer’s loop) — common, often subclinical
- Memory decline (dominant hippocampus — Wada predicts), naming difficulty (dominant)
- Vascular injury (anterior choroidal → hemiparesis; PCA, MCA)
- CN III palsy, hemiparesis, hemorrhage, infection
- Persistent seizures (~30% not seizure-free)
Operative Note Template
Preoperative Diagnosis: Drug-resistant [left/right] mesial temporal lobe epilepsy (hippocampal sclerosis)
Postoperative Diagnosis: Same
Procedure: [Left/Right] anterior temporal lobectomy with amygdalohippocampectomy
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Adjuncts: Neuronavigation, microscope, CUSA; [ECoG; awake mapping if dominant] Implants: None Complications: None
Indications: [Age]yo [M/F] with drug-resistant mesial temporal lobe epilepsy and concordant EEG/MRI (hippocampal sclerosis); Wada/fMRI established [language/memory] lateralization. Risks (visual field cut, memory/naming, vascular) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced and the head positioned (rotated ~60–90°). A temporal craniotomy low to the middle fossa floor was performed and the dura opened. A lateral neocortical resection was carried out along the middle temporal gyrus (~[4–4.5 cm dominant / 5–5.5 cm non-dominant] from the temporal tip), and the temporal horn entered, identifying the choroid plexus, hippocampus, and collateral eminence.
The amygdala was resected (up to the level of the choroidal point) and the hippocampus and parahippocampal gyrus removed. The pia over the medial structures was preserved, protecting the brainstem, CN III, PCA, anterior choroidal artery, and basal vein in the ambient cistern; vascular structures were preserved. [ECoG was used as indicated.]
Hemostasis was obtained, the dura closed, the bone replaced, and the scalp closed. The patient was awakened and transferred for postoperative visual-field assessment.
Postoperative Plan
- ICU/step-down, neuro checks q1h
- CT/MRI postop; formal visual fields (quadrantanopia)
- Continue AEDs (taper later per epileptologist if seizure-free)
- Neuropsych follow-up (memory/language), Engel/ILAE outcome tracking
- DVT prophylaxis; epilepsy team follow-up
Chief-Level Case Review
Use these as the senior-level mental model for Anterior Temporal Lobectomy / Selective Amygdalohippocampectomy (Epilepsy):
- Decision point: Define the symptom physiology: target circuit or offending vessel/nerve must match the history, exam, imaging, and intraoperative monitoring plan.
- Technical lever: Small errors matter: trajectory, lead/contact position, arachnoid dissection, cranial-nerve handling, or mapping threshold can be the difference between success and morbidity.
- Bailout: Have a stop rule: unacceptable mapping response, BAER/MEP/SSEP change, hemorrhage, CSF loss, poor target confidence, or patient intolerance should trigger a defined pivot.
- Postop watch: Postop success requires programming/follow-up details: neurologic exam, imaging, medication adjustment, device restrictions, wound care, and symptom-specific outcome tracking.
Common Pimp Questions
Use these to pressure-test preparation for Anterior Temporal Lobectomy / Selective Amygdalohippocampectomy (Epilepsy):
- What is the symptom target and what finding proves the correct neural structure is being treated?
- What imaging, tractography, MER, stimulation, or mapping information changes the trajectory?
- What medication adjustments or anesthesia constraints matter on the day of surgery?
- What complication would be subtle but important to detect in recovery?
- What postop programming, imaging, seizure, swallow, or cranial-nerve plan is needed?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Awake/asleep technique, MER/stimulation thresholds, and imaging confirmation: [attending-specific]
- Medication hold/restart protocol and programming timeline: [attending-specific]
- Hardware brand, tunneling side, battery pocket, and antibiotic envelope preference: [attending-specific]
- Postop CT/MRI timing and symptom-specific neuro checks: [attending-specific]