
Case Prep: Ventriculopleural (VPL) Shunt Placement
Case / Approach Snapshot
- Anatomy at risk: entry point, ventricular target, choroid plexus and deep veins, cortical vessels, eloquent cortex/tracts, catheter path, and distal hardware route.
- Operative steps: confirm indication and side, plan trajectory, prepare hardware, access ventricle or cistern safely, confirm flow/position, tunnel/connect devices when needed, and define infection/obstruction surveillance; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: malposition, hemorrhage, poor CSF return, overdrainage/underdrainage, obstruction, infection, abdominal/pleural complication, slit ventricles, and revision algorithm.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with hydrocephalus and [peritoneal AND atrial sites unavailable] planned for right ventriculopleural shunt placement.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Spontaneous Extrusion of Ventriculopleural Shunt Catheter Associated with Pleural Effusion — Robles LA. World neurosurgery 2020. PubMed
- Ventriculopleural shunt: Review of literature and novel ways to improve ventriculopleural shunt tolerance — Wong T. Journal of the neurological sciences 2021. PubMed
- Are ventriculopleural shunts the second option for treating hydrocephalus? A meta-analysis of 543 patients — Brenner LBO. Clinical neurology and neurosurgery 2024. PubMed
- Abdominal pseudocyst complicating ventriculoperitoneal shunt: A rare indication for ventriculopleural shunt conversion — Shrestha N. Clinical case reports 2023. PubMed
- Ultrasound-guided percutaneous ventriculopleural shunt placement: a minimally invasive technique — Baro V. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2020. PubMed
- Ventriculopleural shunts in a pediatric population: a review of 170 consecutive patients — Christian EA. Journal of neurosurgery. Pediatrics 2021. PubMed
- Case series of ventriculopleural shunts in adults: a single-center experience — Craven C. Journal of neurosurgery 2017. PubMed
- Ventriculopleural shunts for hydrocephalus: a useful alternative — Jones RF. Neurosurgery 1988. PubMed
- Cross-sectional imaging of thoracic and abdominal complications of cerebrospinal fluid shunt catheters — Bolster F. Emergency radiology 2016. PubMed
- Migration of the abdominal catheter of a ventriculoperitoneal shunt into the mouth: a rare presentation — Low SW. The Malaysian journal of medical sciences : MJMS 2010. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
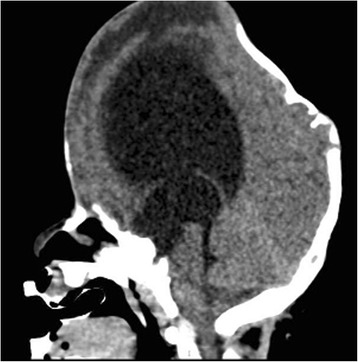 Fig. 1. Sagittal MR image shows marked ventricular dilatation in our patient affected by Pfeiffer syndrome Source: Pleural effusion from intrathoracic migration of a ventriculo-peritoneal shunt catheter: pediatric case report and review of the literature — Italian Journal of Pediatrics 2018; CC BY.
Fig. 1. Sagittal MR image shows marked ventricular dilatation in our patient affected by Pfeiffer syndrome Source: Pleural effusion from intrathoracic migration of a ventriculo-peritoneal shunt catheter: pediatric case report and review of the literature — Italian Journal of Pediatrics 2018; CC BY.
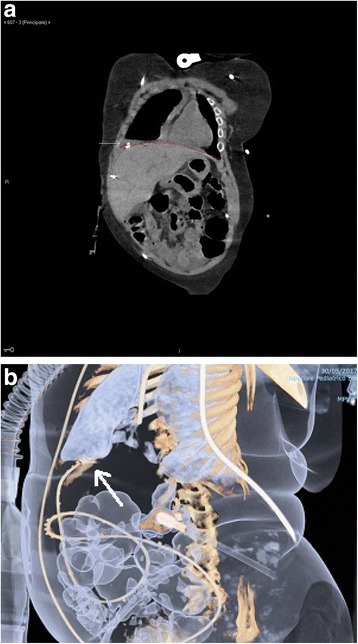 Fig. 2. a Coronal plane of chest and abdomen CT scan demonstrating the dislocation of the distal end of VP shunt situated over the diaphragmatic cupola and within the pleural cavity. b Abdomen… Source: Pleural effusion from intrathoracic migration of a ventriculo-peritoneal shunt catheter: pediatric case report and review of the literature — Italian Journal of Pediatrics 2018; CC BY.
Fig. 2. a Coronal plane of chest and abdomen CT scan demonstrating the dislocation of the distal end of VP shunt situated over the diaphragmatic cupola and within the pleural cavity. b Abdomen… Source: Pleural effusion from intrathoracic migration of a ventriculo-peritoneal shunt catheter: pediatric case report and review of the literature — Italian Journal of Pediatrics 2018; CC BY.
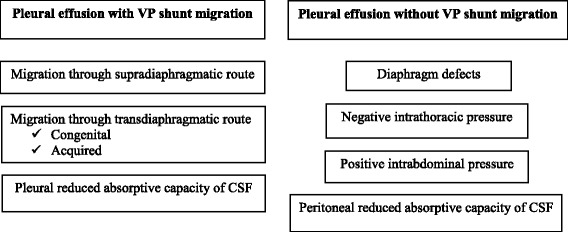 Fig. 3. Factors contributing to CSF hydrothorax with or without intrathoracic VP migration Source: Pleural effusion from intrathoracic migration of a ventriculo-peritoneal shunt catheter: pediatric case report and review of the literature — Italian Journal of Pediatrics 2018; CC BY.
Fig. 3. Factors contributing to CSF hydrothorax with or without intrathoracic VP migration Source: Pleural effusion from intrathoracic migration of a ventriculo-peritoneal shunt catheter: pediatric case report and review of the literature — Italian Journal of Pediatrics 2018; CC BY.
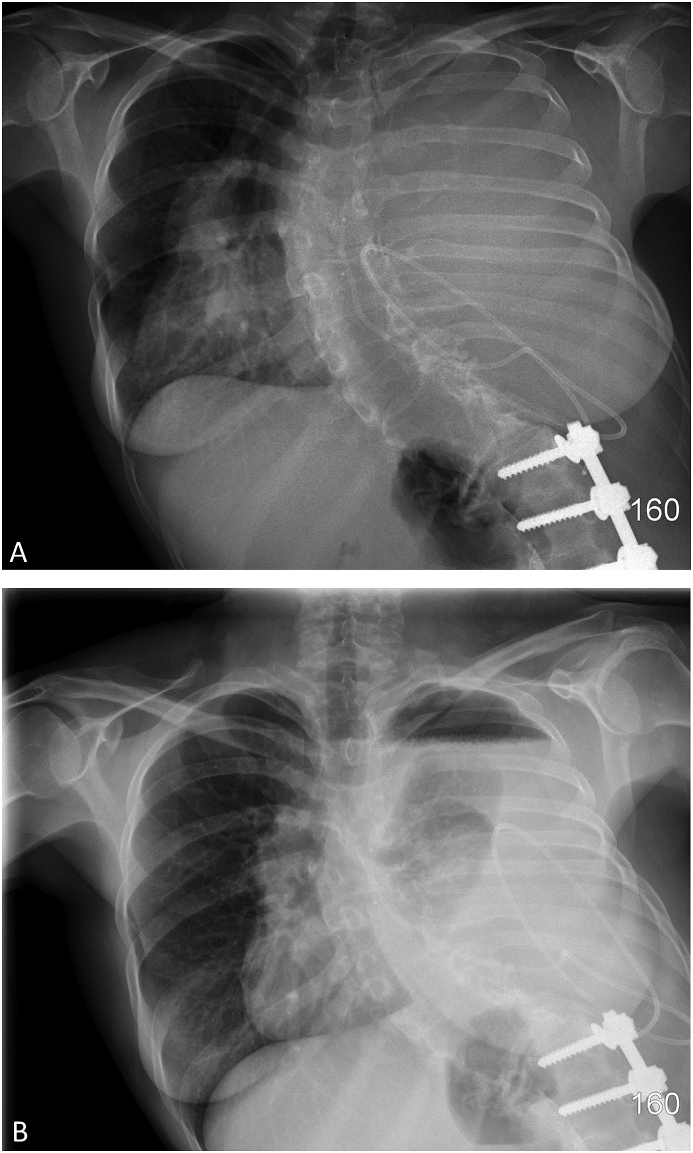 Fig. 1. (A) Chest radiograph taken before thoracentesis demonstrating a large left-sided pleural effusion. (B) Post-thoracentesis chest radiograph demonstrating an air-fluid level over the left… Source: Pleural cerebrospinal fluid shunting causing trapped lung: A respiratory physician’s approach to management and prevention — Respiratory Medicine Case Reports 2018; CC BY-NC-ND.
Fig. 1. (A) Chest radiograph taken before thoracentesis demonstrating a large left-sided pleural effusion. (B) Post-thoracentesis chest radiograph demonstrating an air-fluid level over the left… Source: Pleural cerebrospinal fluid shunting causing trapped lung: A respiratory physician’s approach to management and prevention — Respiratory Medicine Case Reports 2018; CC BY-NC-ND.
 Fig. 2. (A) Post-thoracentesis computed tomography scan showing left hydropneumothorax, left lung collapse, and rightwards mediastinum shift. Source: Pleural cerebrospinal fluid shunting causing trapped lung: A respiratory physician’s approach to management and prevention — Respiratory Medicine Case Reports 2018; CC BY-NC-ND.
Fig. 2. (A) Post-thoracentesis computed tomography scan showing left hydropneumothorax, left lung collapse, and rightwards mediastinum shift. Source: Pleural cerebrospinal fluid shunting causing trapped lung: A respiratory physician’s approach to management and prevention — Respiratory Medicine Case Reports 2018; CC BY-NC-ND.
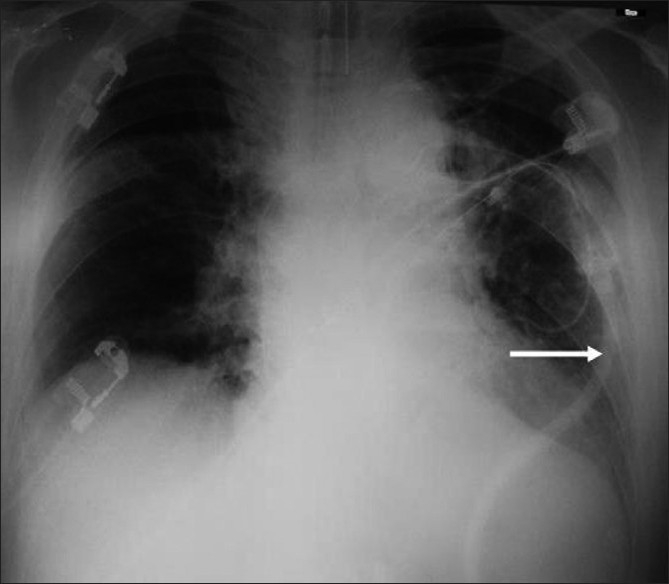 Figure 1. Chest X-ray of case 2 after the VPLS placement. Arrow shows the ventriculo-pleural shunt Source: Pleural effusion following ventriculopleural shunt: Case reports and review of the literature — Annals of Thoracic Medicine 2010; CC BY.
Figure 1. Chest X-ray of case 2 after the VPLS placement. Arrow shows the ventriculo-pleural shunt Source: Pleural effusion following ventriculopleural shunt: Case reports and review of the literature — Annals of Thoracic Medicine 2010; CC BY.
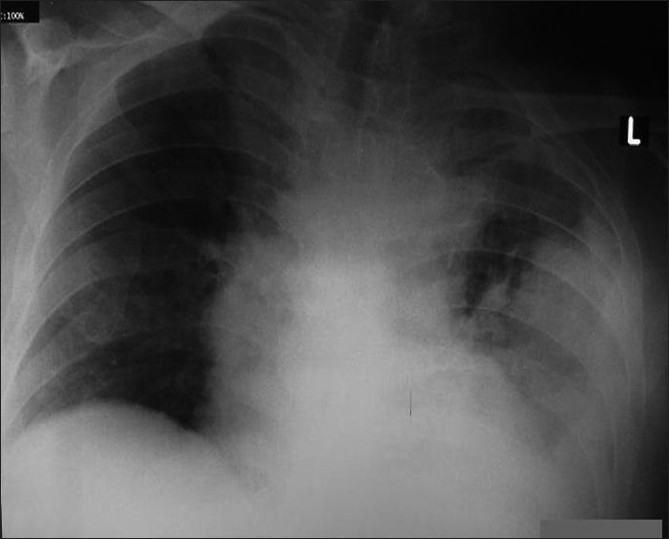 Figure 2. Chest X-ray of the case 2. left-sided large pleural effusion after the VPLS. Source: Pleural effusion following ventriculopleural shunt: Case reports and review of the literature — Annals of Thoracic Medicine 2010; CC BY.
Figure 2. Chest X-ray of the case 2. left-sided large pleural effusion after the VPLS. Source: Pleural effusion following ventriculopleural shunt: Case reports and review of the literature — Annals of Thoracic Medicine 2010; CC BY.
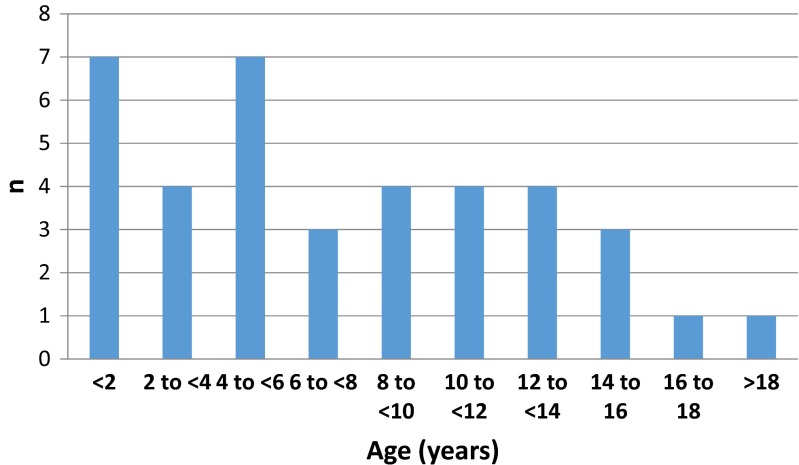 Fig. 1. Range of ages at which the primary VA shunt was inserted Source: Ultrasound guided placement of the distal catheter in paediatric ventriculoatrial shunts—an appraisal of efficacy and complications — Child’s Nervous System 2016; CC BY.
Fig. 1. Range of ages at which the primary VA shunt was inserted Source: Ultrasound guided placement of the distal catheter in paediatric ventriculoatrial shunts—an appraisal of efficacy and complications — Child’s Nervous System 2016; CC BY.
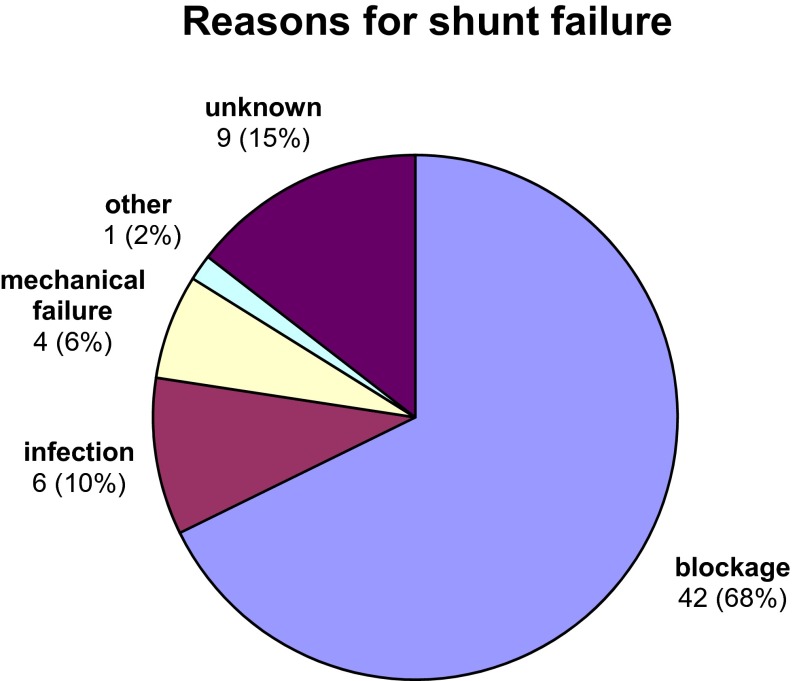 Fig. 3. Reasons for shunt failure Source: Ultrasound guided placement of the distal catheter in paediatric ventriculoatrial shunts—an appraisal of efficacy and complications — Child’s Nervous System 2016; CC BY.
Fig. 3. Reasons for shunt failure Source: Ultrasound guided placement of the distal catheter in paediatric ventriculoatrial shunts—an appraisal of efficacy and complications — Child’s Nervous System 2016; CC BY.
History of Present Illness
- Chief complaint: Hydrocephalus requiring CSF diversion when peritoneal and atrial sites are exhausted/contraindicated
- VPL indications: multiple failed VP shunts, peritoneal contraindication, plus atrial contraindication/exhaustion
- Avoid in young children/infants (limited respiratory reserve — pleural effusion poorly tolerated)
- Prior shunt history
Past Medical History
- Pulmonary disease, limited respiratory reserve (relative contraindication — effusion), pleural pathology, prior thoracic surgery
- Age (avoid in small children)
- Standard PMH
Imaging Review
CT/MRI head
- Ventricle size, catheter target, baseline
Chest imaging
- Baseline lungs/pleura, exclude effusion/pleural disease
Labs
- CBC, BMP, Coags, type and screen
Neurological Examination
- Baseline; hydrocephalus signs; respiratory status
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: navigation or endoscope as indicated, shunt hardware/valve setting verified, distal-access tools or general surgery help when needed, antibiotic-impregnated catheter availability, and postop imaging plan.
- Special needs: antibiotic timing, programmable valve documentation, abdominal/chest/vascular distal-site plan, CSF culture plan for revision/infection, anticoagulation plan, and EVD backup if access fails.
- Immediate postop orders: neuro checks, CT or shunt-series timing, valve setting documentation and MRI precautions, wound/abdominal/distal-site checks, infection watch, DVT timing, and follow-up for setting adjustment.
Distal-Site Selection
- Ventriculopleural shunting is usually a salvage distal site when the peritoneum is hostile and atrial placement is undesirable or unavailable.
- Favor in older children/adults with adequate pulmonary reserve, no active pleural disease, and a clear reason the abdomen is unsuitable.
- Avoid or reconsider in infants/small children, severe restrictive/obstructive lung disease, prior pleurodesis/empyema, recurrent effusions, pulmonary hypertension, or inability to tolerate even a moderate CSF pleural collection.
- Compare against VA shunt, endoscopic options, laparoscopic-assisted peritoneal revision, and ETV/CPC before committing to the pleura.
Valve and Drainage Strategy
- Use a programmable valve and strongly consider anti-siphon/gravitational control because negative intrathoracic pressure can turn ordinary drainage into overdrainage.
- If the patient already overdrains, start with a higher opening pressure and document the rationale; pleural shunts can make slit-ventricle symptoms worse.
- If pleural effusion develops with controlled ventricles, first ask whether the valve is too low, absorption is inadequate, or infection/empyema is present.
Position
- Supine (slight lateral tilt/roll for chest access), head turned, right neck/chest exposed
Key Surgical Steps
- Proximal (ventricular) catheter — as VP (frontal/occipital), CSF flow, connect to valve
- Pleural distal catheter placement:
- Small incision over the anterior/lateral chest (e.g., 4th-5th intercostal space, mid-axillary or anterior)
- Dissect to the intercostal space (over the rib to avoid the neurovascular bundle under the rib)
- Enter the pleural space carefully under controlled ventilation (brief hold) — avoid lung injury
- Insert the distal catheter into the pleural space (several cm)
- Tunnel catheter from cranial/neck to chest incision, connect valve to pleural catheter, confirm flow
- Purse-string / layered closure around the pleural entry to prevent air leak; consider valsalva to check for air leak
- A valve with anti-siphon/appropriate pressure is important (negative intrapleural pressure can promote overdrainage/siphoning)
- Postop CXR — confirm catheter position, rule out pneumothorax
Critical Anatomy & Structures at Risk
- Lung — pneumothorax during pleural entry
- Intercostal neurovascular bundle (under the rib — go over the rib)
- Pleura — effusion (CSF accumulation), empyema
- Overdrainage (negative intrapleural pressure siphons CSF)
Equipment
- Shunt system with valve (anti-siphon/gravitational recommended), distal catheter
- Chest entry/thoracic instruments, antibiotic-impregnated catheter
- CXR capability
Anesthesia
- General; brief ventilation hold during pleural entry; cefazolin; monitor for pneumothorax
Potential Complications
- Pneumothorax (entry), symptomatic pleural effusion / hydrothorax (CSF — may need higher-pressure/anti-siphon valve, or conversion), empyema
- Overdrainage (negative intrapleural pressure) — anti-siphon valve mitigates
- Catheter migration, obstruction, infection
- Respiratory compromise (esp. children/limited reserve)
Rescue and Revision Logic
- Pneumothorax: obtain immediate CXR for dyspnea, desaturation, or difficult ventilation; small stable pneumothorax may observe, but tension physiology needs urgent decompression/chest tube.
- Early pleural effusion: evaluate respiratory status, shunt function, valve setting, and infection markers; tap only if diagnostic or therapeutic benefit outweighs seeding risk.
- Recurrent hydrothorax with functioning proximal catheter: raise valve setting/add anti-siphon if underdrainage is not present; convert distal site if effusions recur or pulmonary reserve is marginal.
- Empyema or pleural infection: externalize/remove infected hardware, culture CSF/pleural fluid, treat with antibiotics, and delay reimplantation until infection clears.
- Persistent hydrocephalus despite pleural catheter: check proximal obstruction, valve malfunction, catheter kinking at the chest wall, and whether the pleural catheter is loculated outside the absorptive pleural space.
Operative Note Template
Preoperative Diagnosis: Hydrocephalus with peritoneal and atrial distal sites unavailable/exhausted
Postoperative Diagnosis: Same
Procedure: Right ventriculopleural shunt placement with [anti-siphon/programmable] valve
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Adjuncts: Thoracic entry set, tunneler, CXR Implants: Ventricular catheter, anti-siphon/programmable valve, pleural distal catheter Complications: None
Indications: [Age]yo [M/F] (not a young child) with hydrocephalus requiring CSF diversion where peritoneal and atrial sites are unavailable. Risks (pneumothorax, pleural effusion, overdrainage) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced. A [frontal/occipital] ventricular catheter was placed with CSF return and connected to the valve. A small incision was made over the [4th–5th] intercostal space and dissection carried to the intercostal space over the rib (avoiding the neurovascular bundle). The pleural space was entered carefully during a brief ventilation hold, and the distal catheter inserted several centimeters into the pleural space.
The catheter was tunneled and connected to the anti-siphon valve (to counter negative intrapleural pressure), CSF flow confirmed, and an air-tight purse-string/layered closure performed around the pleural entry. A postoperative CXR confirmed catheter position and excluded pneumothorax.
The patient was transferred with respiratory monitoring and serial CXR surveillance for effusion.
Postoperative Plan
- Floor/step-down, neuro and respiratory checks
- CXR (pneumothorax, catheter position; recheck for effusion)
- CT head (ventricles), shunt series baseline, document valve setting
- Monitor for pleural effusion (dyspnea, decreased breath sounds — serial CXR; large effusion may need valve adjustment or conversion)
- Follow-up imaging; counsel re: effusion risk
Chief-Level Case Review
Use these as the senior-level mental model for Ventriculopleural (VPL) Shunt Placement:
- Decision point: Trajectory and hardware choice should follow the failure mode: obstruction, infection, overdrainage, loculation, slit ventricle, distal failure, or wrong pressure setting.
- Technical lever: Document the system: entry point, catheter target/depth, valve type and setting, distal site, antibiotic-impregnated hardware, and what imaging confirms placement.
- Bailout: Rescue plan is practical: poor CSF return, bloody CSF, malposition, distal access failure, abdominal/pleural complication, or inability to safely pass the catheter.
- Postop watch: Postop orders must be unambiguous: drain height/rate/max output, valve setting, clamp parameters, imaging, antibiotics, ICP/neuro checks, and overdrainage precautions.
Common Pimp Questions
Use these to pressure-test preparation for Ventriculopleural (VPL) Shunt Placement:
- What is the working CSF physiology problem: obstruction, absorption failure, overdrainage, infection, or catheter failure?
- Where exactly is the entry point, target, and backup trajectory?
- What valve, catheter, endoscope, or navigation preference does the attending use?
- What is the infection-prevention plan and what cultures/CSF studies are needed?
- What postop imaging, valve setting, drainage level, and neuro-check plan should be written?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Valve brand/setting, antibiotic catheter use, and tunneling side: [attending-specific]
- Navigation/endoscope/stylet preference and ventricular target: [attending-specific]
- CSF culture/lab routine and perioperative antibiotic duration: [attending-specific]
- Postop scan timing, EVD height or valve verification, and activity restrictions: [attending-specific]