
Case Prep: Subduroperitoneal (Subdural-Peritoneal) Shunt Placement
Case / Approach Snapshot
- Anatomy at risk: thin cortex under a chronic collection, bridging veins, subdural membranes, superior sagittal sinus, burr-hole edge, catheter side holes, scalp/valve pocket, tunneling tract, and peritoneal entry.
- Operative steps: confirm the collection is a persistent symptomatic subdural compartment rather than hydrocephalus or atrophy, choose a safe burr-hole site, enter subdural space tangentially, confirm fluid egress, secure a low-pressure drainage system, tunnel to the peritoneum, and plan removal/revision once the collection resolves.
- Rescue plans: cortical injury, catheter migration into subdural space or peritoneum, overdrainage with rebleeding/collapse, underdrainage/loculation, infection, peritoneal failure, nonaccidental trauma workup, and planned explantation in infants/children.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age — often pediatric] [M/F] with a [chronic subdural hygroma / effusion / refractory subdural collection] planned for subduroperitoneal shunt placement.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Complications of subduroperitoneal shunting — Ersahin Y. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2000. PubMed
- A new catheter for subduro-peritoneal shunting — Erşahin Y. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2002. PubMed
- Minicraniotomy with a subgaleal pocket for the treatment of subdural fluid collections in infants — Palmer AW. Journal of neurosurgery. Pediatrics 2019. PubMed
- Managing subdural fluid collection in infants — Miyake H. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2002. PubMed
- Subdural-atrial and subdural-peritoneal shunting in infants with chronic subdural fluid collections — Korinth MC. Journal of pediatric surgery 2000. PubMed
- Rectal dural metastasis masquerading as chronic subdural hematoma: illustrative case — Siy HFC. Journal of neurosurgery. Case lessons 2023. PubMed
- Subdural hygroma: results of treatment by ventriculo-abdominal shunt — Njiokiktjien CJ. Child’s brain 1980. PubMed
- A Rare Complication of Subdural-peritoneal Shunt: Migration of Catheter Components through the Pelvic Inlet into the Subdural Space — Çakir M. Journal of pediatric neurosciences 2017. PubMed
- Ruptured intracranial arachnoid cysts in the subdural space: evaluation of subduro-peritoneal shunts in a pediatric population — Tinois J. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2020. PubMed
- Management of symptomatic chronic extra-axial fluid collections in pediatric patients — Litofsky NS. Neurosurgery 1992. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
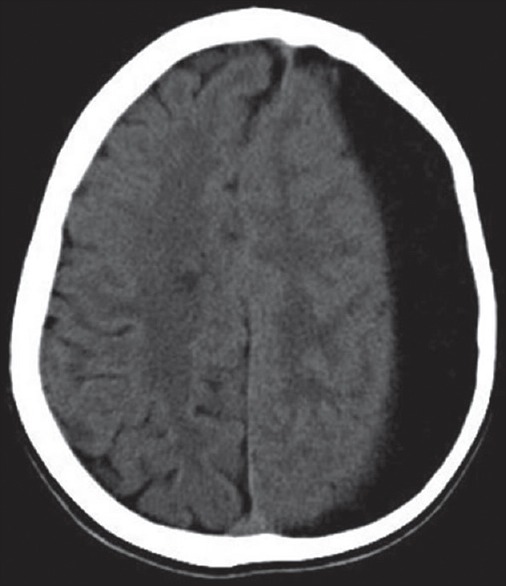 Figure 1. First admission image with left chronic subdural effusion Source: A Rare Complication of Subdural-peritoneal Shunt: Migration of Catheter Components through the Pelvic Inlet into the Subdural Space — Journal of Pediatric Neurosciences 2017; CC BY-NC-SA.
Figure 1. First admission image with left chronic subdural effusion Source: A Rare Complication of Subdural-peritoneal Shunt: Migration of Catheter Components through the Pelvic Inlet into the Subdural Space — Journal of Pediatric Neurosciences 2017; CC BY-NC-SA.
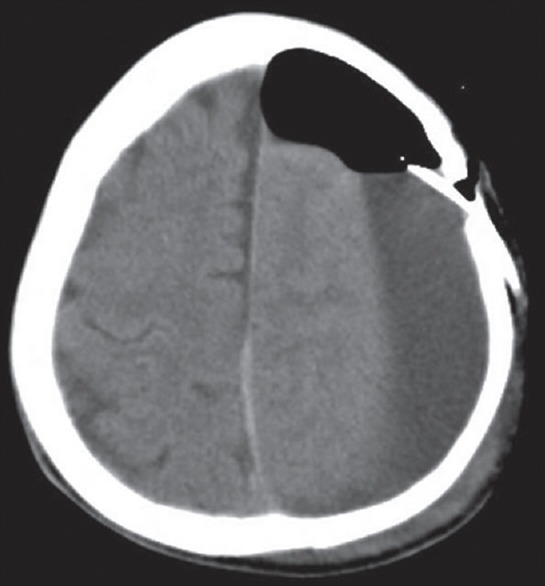 Figure 2. After the subduroperitoneal shunt placement surgery Source: A Rare Complication of Subdural-peritoneal Shunt: Migration of Catheter Components through the Pelvic Inlet into the Subdural Space — Journal of Pediatric Neurosciences 2017; CC BY-NC-SA.
Figure 2. After the subduroperitoneal shunt placement surgery Source: A Rare Complication of Subdural-peritoneal Shunt: Migration of Catheter Components through the Pelvic Inlet into the Subdural Space — Journal of Pediatric Neurosciences 2017; CC BY-NC-SA.
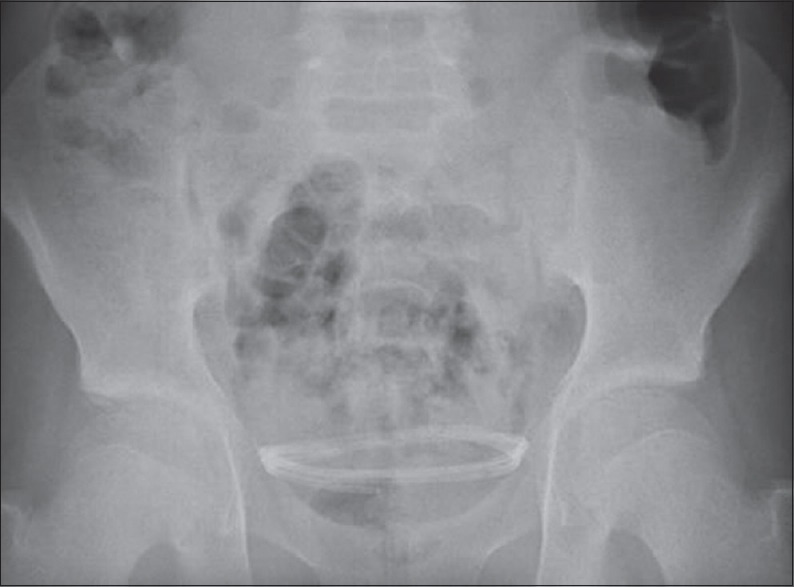 Figure 3. Control abdominal X-ray showing that the shunt material completely migrated into the pelvic inlet Source: A Rare Complication of Subdural-peritoneal Shunt: Migration of Catheter Components through the Pelvic Inlet into the Subdural Space — Journal of Pediatric Neurosciences 2017; CC BY-NC-SA.
Figure 3. Control abdominal X-ray showing that the shunt material completely migrated into the pelvic inlet Source: A Rare Complication of Subdural-peritoneal Shunt: Migration of Catheter Components through the Pelvic Inlet into the Subdural Space — Journal of Pediatric Neurosciences 2017; CC BY-NC-SA.
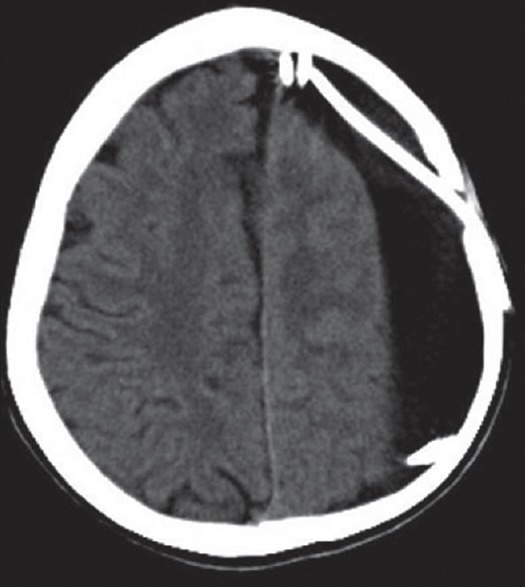 Figure 4. Control brain computed tomography scan showing that the shunt material completely migrated into the cranium Source: A Rare Complication of Subdural-peritoneal Shunt: Migration of Catheter Components through the Pelvic Inlet into the Subdural Space — Journal of Pediatric Neurosciences 2017; CC BY-NC-SA.
Figure 4. Control brain computed tomography scan showing that the shunt material completely migrated into the cranium Source: A Rare Complication of Subdural-peritoneal Shunt: Migration of Catheter Components through the Pelvic Inlet into the Subdural Space — Journal of Pediatric Neurosciences 2017; CC BY-NC-SA.
 Figure 5. Control plane anterior-posterior X-ray of the skull showing that the shunt material completely migrated into the cranium Source: A Rare Complication of Subdural-peritoneal Shunt: Migration of Catheter Components through the Pelvic Inlet into the Subdural Space — Journal of Pediatric Neurosciences 2017; CC BY-NC-SA.
Figure 5. Control plane anterior-posterior X-ray of the skull showing that the shunt material completely migrated into the cranium Source: A Rare Complication of Subdural-peritoneal Shunt: Migration of Catheter Components through the Pelvic Inlet into the Subdural Space — Journal of Pediatric Neurosciences 2017; CC BY-NC-SA.
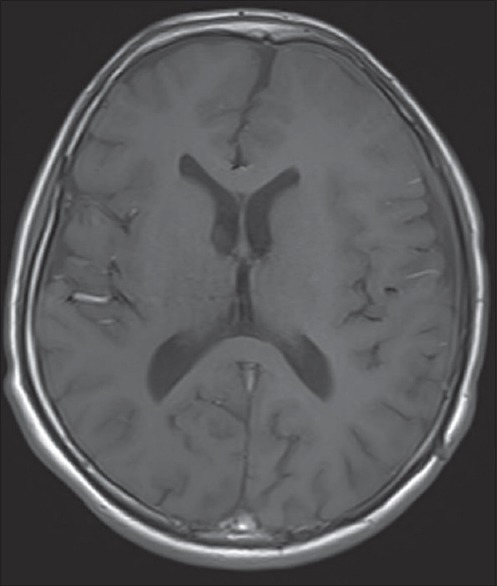 Figure 6. Three months later, control magnetic resonance imaging. After the surgical evacuation Source: A Rare Complication of Subdural-peritoneal Shunt: Migration of Catheter Components through the Pelvic Inlet into the Subdural Space — Journal of Pediatric Neurosciences 2017; CC BY-NC-SA.
Figure 6. Three months later, control magnetic resonance imaging. After the surgical evacuation Source: A Rare Complication of Subdural-peritoneal Shunt: Migration of Catheter Components through the Pelvic Inlet into the Subdural Space — Journal of Pediatric Neurosciences 2017; CC BY-NC-SA.
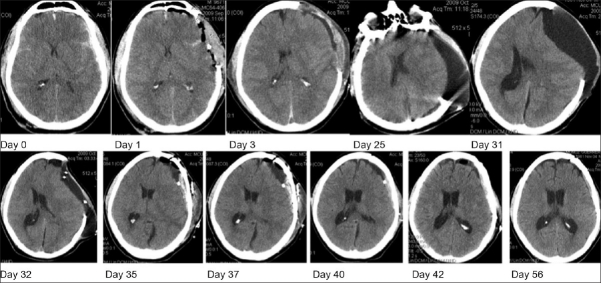 Figure 1. Evolution of Subdural Collection through sequential computed tomography scans. The collection reaches its peak volume by day 31, then, a subdural catheter is placed by day 32. By day 35,… Source: Normal pressure subdural hygroma with mass effect as a complication of decompressive craniectomy — Surgical Neurology International 2011; CC BY-NC-SA.
Figure 1. Evolution of Subdural Collection through sequential computed tomography scans. The collection reaches its peak volume by day 31, then, a subdural catheter is placed by day 32. By day 35,… Source: Normal pressure subdural hygroma with mass effect as a complication of decompressive craniectomy — Surgical Neurology International 2011; CC BY-NC-SA.
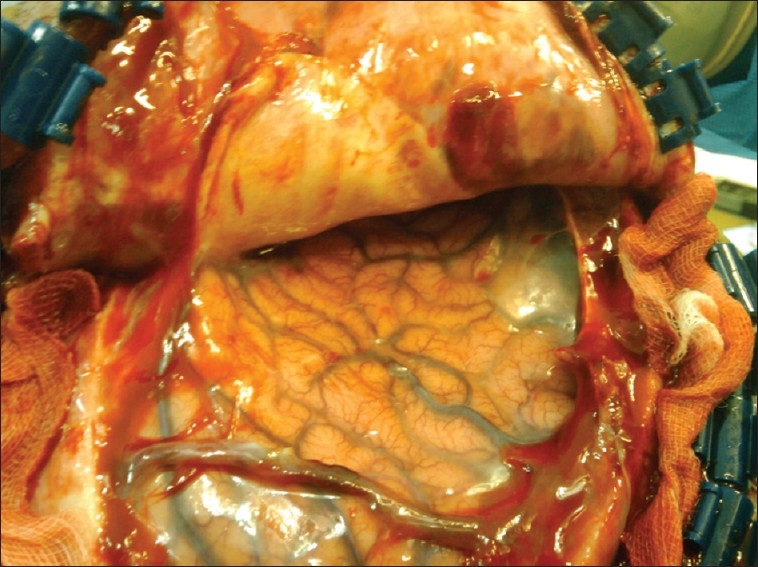 Figure 2. Surgical view: Brain parenchyma is depressed, and neomembranes are seeing in the operative field with thick vessels Source: Normal pressure subdural hygroma with mass effect as a complication of decompressive craniectomy — Surgical Neurology International 2011; CC BY-NC-SA.
Figure 2. Surgical view: Brain parenchyma is depressed, and neomembranes are seeing in the operative field with thick vessels Source: Normal pressure subdural hygroma with mass effect as a complication of decompressive craniectomy — Surgical Neurology International 2011; CC BY-NC-SA.
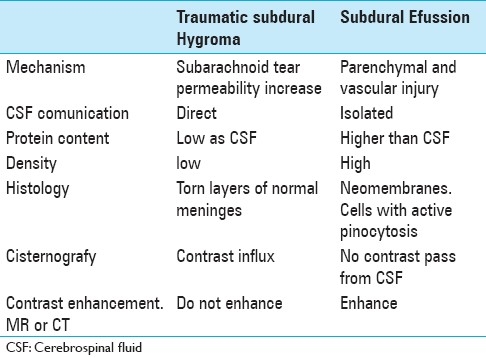 Figure 9. Source: Normal pressure subdural hygroma with mass effect as a complication of decompressive craniectomy — Surg Neurol Int. 2011 Jun 30;2:88. doi: 10.4103/2152-7806.82370; CC BY-NC-SA.
Figure 9. Source: Normal pressure subdural hygroma with mass effect as a complication of decompressive craniectomy — Surg Neurol Int. 2011 Jun 30;2:88. doi: 10.4103/2152-7806.82370; CC BY-NC-SA.
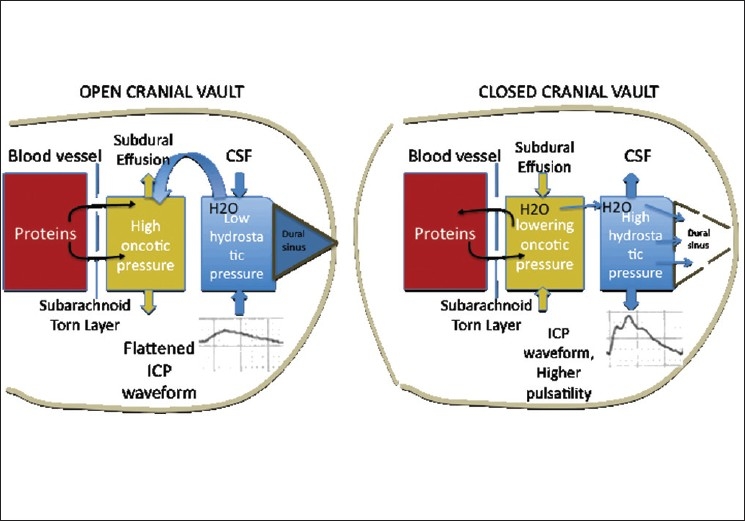 Figure 3. Open cranial Vault: the abnormal permeability allows the protein leakage, thus increasing the oncotic pressure of the subdural effusion, and drawing water. With the decompressive… Source: Normal pressure subdural hygroma with mass effect as a complication of decompressive craniectomy — Surgical Neurology International 2011; CC BY-NC-SA.
Figure 3. Open cranial Vault: the abnormal permeability allows the protein leakage, thus increasing the oncotic pressure of the subdural effusion, and drawing water. With the decompressive… Source: Normal pressure subdural hygroma with mass effect as a complication of decompressive craniectomy — Surgical Neurology International 2011; CC BY-NC-SA.
History of Present Illness
- Chief complaint: Persistent/symptomatic subdural fluid collection (hygroma/effusion) refractory to drainage
- Common scenarios: pediatric subdural hygromas/effusions (post-meningitis, post-trauma, benign external hydrocephalus complications), chronic subdural collections that re-accumulate after burr-hole drainage, post-craniotomy subdural collections
- Prior drainage attempts, macrocephaly (infants), bulging fontanelle
Past Medical History
- Prior subdural drainage, meningitis/infection, trauma (consider NAT in infants — work up appropriately), coagulopathy
- Etiology of collection
- Standard PMH
Imaging Review
CT/MRI head
- Subdural collection (size, chronicity, density/signal — hygroma vs chronic SDH vs effusion), bilateral?, mass effect, membranes, ventricle size (distinguish from hydrocephalus)
- Underlying brain (atrophy, parenchymal injury)
Decision Check: Is This Really a Shunt Problem?
- Confirm symptoms or growth: enlarging head circumference, bulging fontanelle, irritability, seizures, developmental regression, focal deficit, or persistent mass effect.
- Distinguish a drainable subdural compartment from benign enlarged subarachnoid spaces, cortical atrophy, communicating hydrocephalus, and recurrent chronic subdural hematoma better treated by burr holes/membrane strategy.
- In infants, evaluate for trauma/nonaccidental trauma, coagulopathy, infection, metabolic disease, and retinal/skull/skeletal findings as clinically appropriate.
- If the collection is bilateral, decide whether unilateral drainage will equilibrate through membranes or whether bilateral catheters/burr holes are needed.
- If membranes or chronic blood dominate, shunt alone may underperform; consider burr-hole evacuation, minicraniotomy, membranectomy, or temporary drainage strategy.
Labs
- CBC, Coags (correct), BMP, type and screen
- Infection workup if indicated
Examination
- Head circumference/fontanelle (infants), neuro exam, signs of raised ICP
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: navigation or endoscope as indicated, shunt hardware/valve setting verified, distal-access tools or general surgery help when needed, antibiotic-impregnated catheter availability, and postop imaging plan.
- Special needs: antibiotic timing, programmable valve documentation, abdominal/chest/vascular distal-site plan, CSF culture plan for revision/infection, anticoagulation plan, and EVD backup if access fails.
- Immediate postop orders: neuro checks, CT or shunt-series timing, valve setting documentation and MRI precautions, wound/abdominal/distal-site checks, infection watch, DVT timing, and follow-up for setting adjustment.
Position
- Supine, head turned (collection side up), neck/chest/abdomen prepped in continuity (as for VP)
Key Surgical Steps
- Proximal (subdural) catheter: burr hole over the collection (or via existing burr hole); open dura; insert the catheter into the subdural space (tangential, low-profile — avoid cortical injury; do not advance like a ventricular catheter)
- Confirm fluid egress
- Connect to a low-pressure valve (subdural collections are low pressure; valve choice to avoid overdrainage but allow drainage) — or sometimes valveless/low-pressure system per surgeon
- Tunnel to the abdomen, peritoneal distal catheter (as VP)
- Confirm flow through system; closure
- Often temporary — many are removed/converted once the collection resolves (esp. pediatric)
Technical Nuances
- Choose a burr hole where the collection is thick enough that catheter side holes sit fully in the subdural compartment without resting on cortex.
- Insert the catheter tangentially along the inner table/subdural plane; a perpendicular trajectory can spear cortex as the collection decompresses.
- Trim side holes so they do not straddle scalp/subgaleal tissue or cortex; all functional holes should live within the subdural collection.
- Anchor the proximal catheter/valve carefully; migration is a distinctive complication in small children with low-resistance systems.
- Avoid rapid decompression if there is chronic membrane vascularity or fragile bridging veins; sudden collapse can promote rebleeding.
- Set expectations that this is often a temporizing device rather than lifelong hardware.
Critical Anatomy & Structures at Risk
- Cortex / bridging veins (subdural catheter — avoid cortical injury, re-bleeding)
- Superior sagittal sinus (keep burr hole lateral)
- Overdrainage vs underdrainage balance; peritoneum/bowel (distal)
Equipment
- Shunt system with low-pressure valve, subdural (proximal) catheter, peritoneal catheter
- Burr hole set, antibiotic-impregnated catheter, tunneler
Anesthesia
- General; cefazolin; pediatric considerations (thermoregulation, blood volume)
Potential Complications
- Catheter obstruction/migration, overdrainage (re-collapse, new collection) or underdrainage
- Infection, cortical injury/hemorrhage
- Persistent collection / conversion needs, peritoneal complications
- In infants — need removal once resolved (foreign body, infection risk if left)
Intraoperative and Postoperative Rescue
- No fluid egress: confirm location with ultrasound/navigation or enlarge/open membranes; reassess whether the collection is loculated, organized, or not under pressure.
- Cortical bleeding: stop further catheter advancement, irrigate, tamponade, obtain postoperative CT, and consider ICU observation if any mass effect or neurologic concern.
- Overdrainage/new hemorrhage: raise valve resistance if possible, clamp/externalize selectively, image, and evacuate if symptomatic.
- Underdrainage: check catheter position, valve function, distal patency, loculations, and whether a second compartment needs separate drainage.
- Infection: treat like infected shunt hardware: cultures, antibiotics, externalization/removal, and delayed reimplantation only if still needed.
Operative Note Template
Preoperative Diagnosis: Symptomatic/refractory subdural [hygroma/effusion/collection]
Postoperative Diagnosis: Same
Procedure: Subduroperitoneal shunt placement with low-pressure valve
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Adjuncts: Burr-hole set, tunneler Implants: Subdural (proximal) catheter, low-pressure valve, peritoneal catheter Complications: None
Indications: [Age]yo [M/F] [often pediatric] with a persistent/symptomatic subdural collection refractory to drainage. Risks (cortical injury, over/under-drainage, infection) discussed; [NAT workup as appropriate].
Description of Procedure: After consent and time-out, general anesthesia was induced. A burr hole was made over the collection (lateral to the sagittal sinus) and the dura opened. The subdural catheter was inserted tangentially into the subdural space (cortex-sparing, not advanced like a ventricular catheter) with fluid egress confirmed, and connected to a low-pressure valve. The catheter was tunneled to a small abdominal incision and the peritoneal distal catheter placed, with flow through the system confirmed.
Closure was performed. The patient was transferred with head-circumference/imaging follow-up; removal/conversion was planned once the collection resolved (to avoid a long-term foreign body).
Postoperative Plan
- Floor, neuro checks, head circumference/fontanelle (infants)
- CT head (collection reduction, catheter position), shunt series baseline
- Monitor for re-accumulation vs overdrainage, infection
- Plan for removal/conversion once collection resolves (pediatric — avoid long-term foreign body)
- Follow-up imaging; NAT workup/social work if applicable
Chief-Level Case Review
Use these as the senior-level mental model for Subduroperitoneal (Subdural-Peritoneal) Shunt Placement:
- Decision point: Trajectory and hardware choice should follow the failure mode: obstruction, infection, overdrainage, loculation, slit ventricle, distal failure, or wrong pressure setting.
- Technical lever: Document the system: entry point, catheter target/depth, valve type and setting, distal site, antibiotic-impregnated hardware, and what imaging confirms placement.
- Bailout: Rescue plan is practical: poor CSF return, bloody CSF, malposition, distal access failure, abdominal/pleural complication, or inability to safely pass the catheter.
- Postop watch: Postop orders must be unambiguous: drain height/rate/max output, valve setting, clamp parameters, imaging, antibiotics, ICP/neuro checks, and overdrainage precautions.
Common Pimp Questions
Use these to pressure-test preparation for Subduroperitoneal (Subdural-Peritoneal) Shunt Placement:
- What is the working CSF physiology problem: obstruction, absorption failure, overdrainage, infection, or catheter failure?
- Where exactly is the entry point, target, and backup trajectory?
- What valve, catheter, endoscope, or navigation preference does the attending use?
- What is the infection-prevention plan and what cultures/CSF studies are needed?
- What postop imaging, valve setting, drainage level, and neuro-check plan should be written?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Valve brand/setting, antibiotic catheter use, and tunneling side: [attending-specific]
- Navigation/endoscope/stylet preference and ventricular target: [attending-specific]
- CSF culture/lab routine and perioperative antibiotic duration: [attending-specific]
- Postop scan timing, EVD height or valve verification, and activity restrictions: [attending-specific]