
Case Prep: Shunt Revision / Exploration
Case / Approach Snapshot
- Anatomy at risk: entry point, ventricular target, choroid plexus and deep veins, cortical vessels, eloquent cortex/tracts, catheter path, and distal hardware route.
- Operative steps: confirm indication and side, plan trajectory, prepare hardware, access ventricle or cistern safely, confirm flow/position, tunnel/connect devices when needed, and define infection/obstruction surveillance; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: malposition, hemorrhage, poor CSF return, overdrainage/underdrainage, obstruction, infection, abdominal/pleural complication, slit ventricles, and revision algorithm.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with an existing [VP/VA/VPL/LP] shunt presenting with [shunt malfunction (raised ICP) / infection / overdrainage / distal failure] planned for shunt exploration and revision.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Distal ventriculoperitoneal shunt catheter tightly coiled around the valve in the absence of a subgaleal cerebrospinal fluid collection: illustrative case — Tamura G. Journal of neurosurgery. Case lessons 2021. PubMed
- Seizures as presentation of shunt malfunction: tertiary paediatric neurosurgery experience — Goel A. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2024. PubMed
- Diagnosis of Ventriculoperitoneal Shunt Malfunction: A Practical Algorithm — Broggi M. World neurosurgery 2020. PubMed
- Lumboperitoneal Shunt Malfunction Due to Misplacement of the Lumbar Catheter Into the Spinal Subdural Extra-arachnoid Space: A Case Report — Hashida K. Cureus 2025. PubMed
- Cerebrospinal Fluid Shunts to Treat Hydrocephalus and Idiopathic Intracranial Hypertension: Shunt Catheters and Valves — D’Antona L. Neurosurgery clinics of North America 2025. PubMed
- Ventriculopleural shunts in a pediatric population: a review of 170 consecutive patients — Christian EA. Journal of neurosurgery. Pediatrics 2021. PubMed
- Risk factors for shunt malfunction in pediatric hydrocephalus: a multicenter prospective cohort study — Riva-Cambrin J. Journal of neurosurgery. Pediatrics 2016. PubMed
- The role of lumboperitoneal shunts in managing chronic hydrocephalus with slit ventricles — Marupudi NI. Journal of neurosurgery. Pediatrics 2018. PubMed
- Mechanical complications of cerebrospinal fluid shunt. Differences between adult and pediatric populations: myths or reality? — Coll G. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2021. PubMed
- Impact of Early Intervention for Idiopathic Normal Pressure Hydrocephalus on Long-Term Prognosis in Prodromal Phase — Kajimoto Y. Frontiers in neurology 2022. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
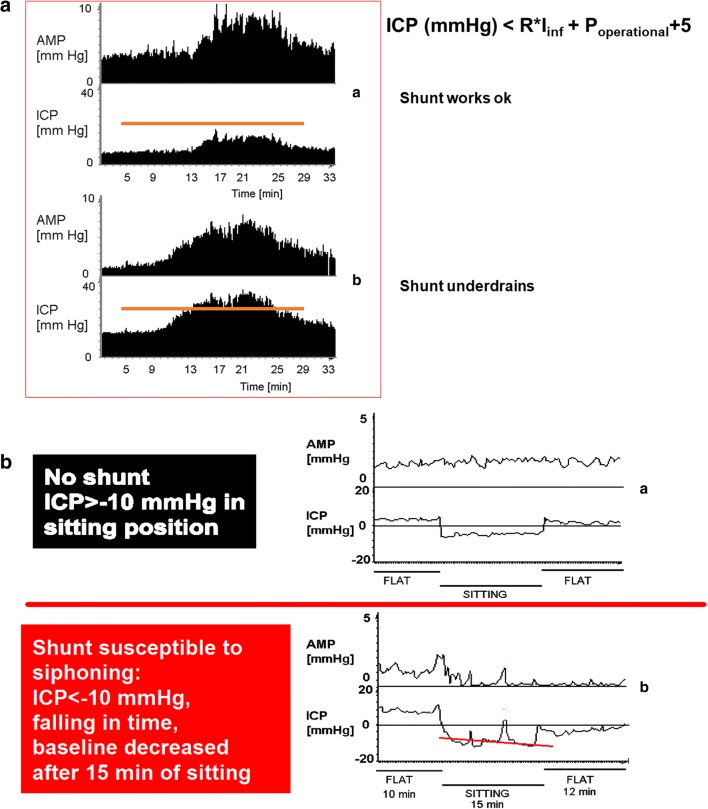 Fig. 1. Shunt testing results of under- and overdrainage. a Top: Normally functioning shunt, with the plateau (steady-state) pressure after infusion of Hartmann’s not exceeding the shunt’s… Source: Shunt infusion studies: impact on patient outcome, including health economics — Acta Neurochirurgica 2020; CC BY.
Fig. 1. Shunt testing results of under- and overdrainage. a Top: Normally functioning shunt, with the plateau (steady-state) pressure after infusion of Hartmann’s not exceeding the shunt’s… Source: Shunt infusion studies: impact on patient outcome, including health economics — Acta Neurochirurgica 2020; CC BY.
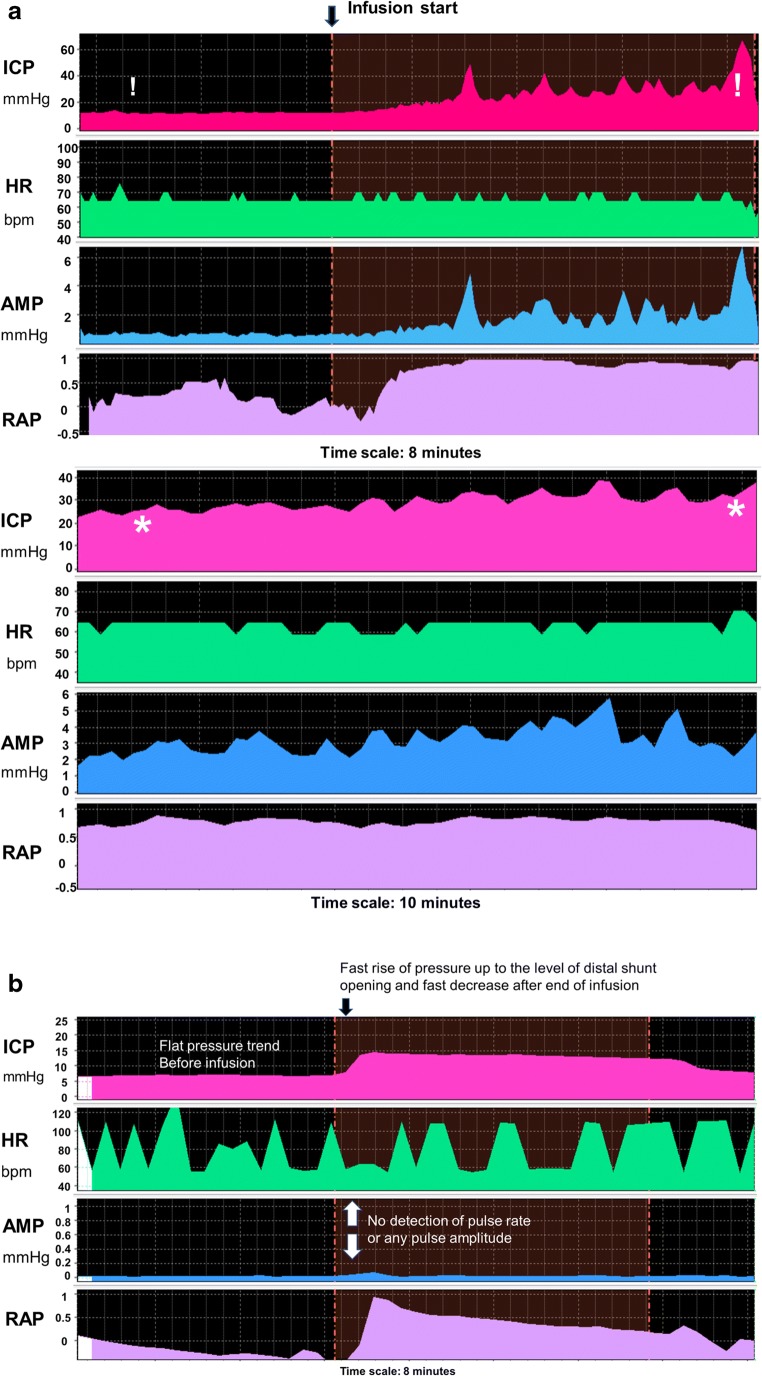 Fig. 2. Shunt testing results of proximal and distal obstruction. a Distal obstruction. Upper panel: distal obstruction detected after infusion of fluid. Initial baseline ICP appears normal (c…. Source: Shunt infusion studies: impact on patient outcome, including health economics — Acta Neurochirurgica 2020; CC BY.
Fig. 2. Shunt testing results of proximal and distal obstruction. a Distal obstruction. Upper panel: distal obstruction detected after infusion of fluid. Initial baseline ICP appears normal (c…. Source: Shunt infusion studies: impact on patient outcome, including health economics — Acta Neurochirurgica 2020; CC BY.
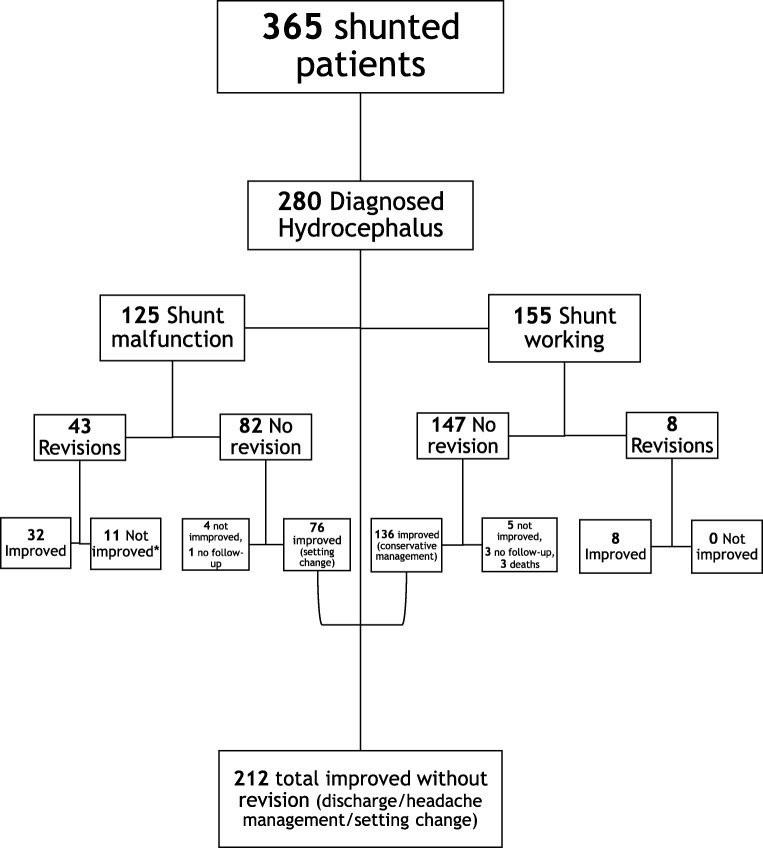 Fig. 3. 1-year outcome of patients with diagnosed hydrocephalus of multiple aetiologies undergoing CSF infusion studies for shunt function assessment in vivo. *1: Not improved after revision:… Source: Shunt infusion studies: impact on patient outcome, including health economics — Acta Neurochirurgica 2020; CC BY.
Fig. 3. 1-year outcome of patients with diagnosed hydrocephalus of multiple aetiologies undergoing CSF infusion studies for shunt function assessment in vivo. *1: Not improved after revision:… Source: Shunt infusion studies: impact on patient outcome, including health economics — Acta Neurochirurgica 2020; CC BY.
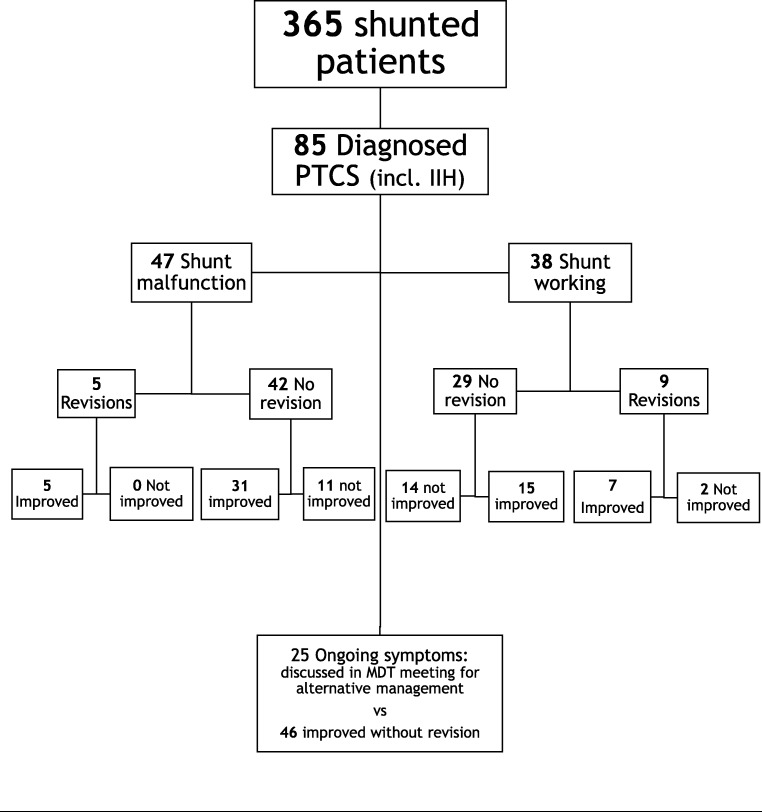 Fig. 4. 1-year outcome of patients with diagnosed pseudotumour cerebri syndrome undergoing CSF infusion studies for shunt function assessment in vivo Source: Shunt infusion studies: impact on patient outcome, including health economics — Acta Neurochirurgica 2020; CC BY.
Fig. 4. 1-year outcome of patients with diagnosed pseudotumour cerebri syndrome undergoing CSF infusion studies for shunt function assessment in vivo Source: Shunt infusion studies: impact on patient outcome, including health economics — Acta Neurochirurgica 2020; CC BY.
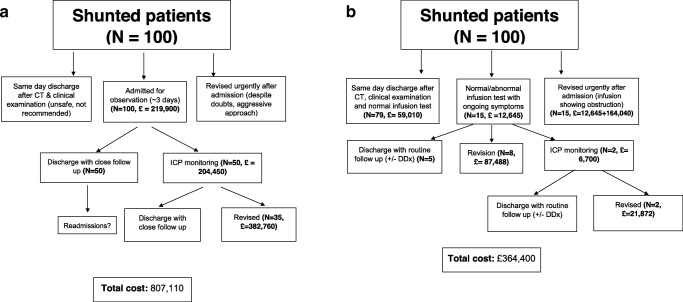 Fig. 5. Elementary decision tree analysis of a costs of shunt malfunction management without infusion studies, b costs of shunt malfunction management as derived from our infusion study… Source: Shunt infusion studies: impact on patient outcome, including health economics — Acta Neurochirurgica 2020; CC BY.
Fig. 5. Elementary decision tree analysis of a costs of shunt malfunction management without infusion studies, b costs of shunt malfunction management as derived from our infusion study… Source: Shunt infusion studies: impact on patient outcome, including health economics — Acta Neurochirurgica 2020; CC BY.
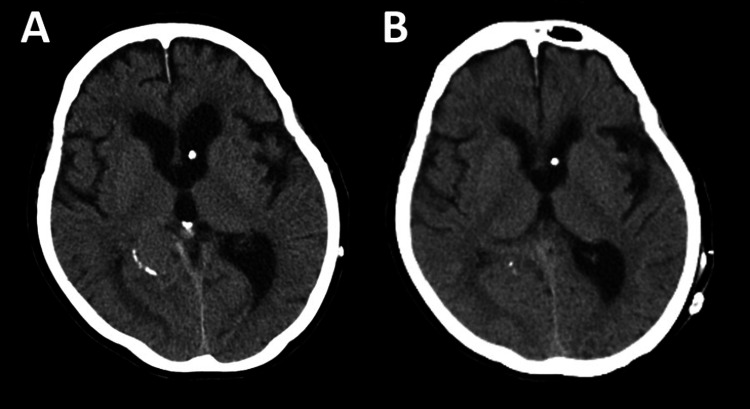 Figure 1. CT images(A) Preoperative CT. (B) Postoperative CT. Source: Accurate Preoperative and Intraoperative Evaluation Reduces Surgical Costs and Patient Invasiveness in Ventriculoperitoneal Shunt Revision — Cureus 2024; CC BY.
Figure 1. CT images(A) Preoperative CT. (B) Postoperative CT. Source: Accurate Preoperative and Intraoperative Evaluation Reduces Surgical Costs and Patient Invasiveness in Ventriculoperitoneal Shunt Revision — Cureus 2024; CC BY.
 Figure 2. Preoperative shuntogram(Left) Schematic diagram showing the smooth flow of the contrast agent into the ventricles, but no progression toward the abdominal cavity. (Middle) Fluoroscopic… Source: Accurate Preoperative and Intraoperative Evaluation Reduces Surgical Costs and Patient Invasiveness in Ventriculoperitoneal Shunt Revision — Cureus 2024; CC BY.
Figure 2. Preoperative shuntogram(Left) Schematic diagram showing the smooth flow of the contrast agent into the ventricles, but no progression toward the abdominal cavity. (Middle) Fluoroscopic… Source: Accurate Preoperative and Intraoperative Evaluation Reduces Surgical Costs and Patient Invasiveness in Ventriculoperitoneal Shunt Revision — Cureus 2024; CC BY.
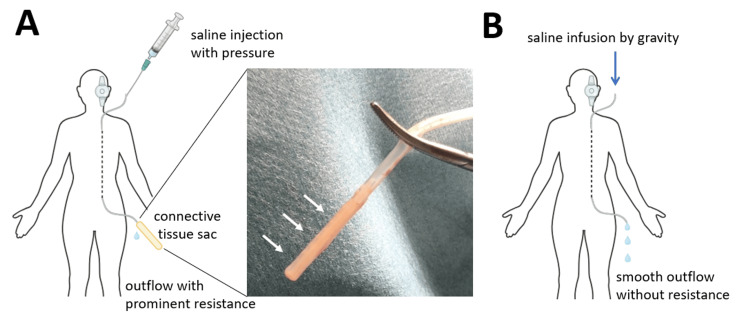 Figure 3. Schematic diagram of cerebrospinal fluid flow changes during surgery(A) The peritoneal catheter’s tip was obstructed by a connective tissue sac (arrows), blocking saline outflow. (B)… Source: Accurate Preoperative and Intraoperative Evaluation Reduces Surgical Costs and Patient Invasiveness in Ventriculoperitoneal Shunt Revision — Cureus 2024; CC BY.
Figure 3. Schematic diagram of cerebrospinal fluid flow changes during surgery(A) The peritoneal catheter’s tip was obstructed by a connective tissue sac (arrows), blocking saline outflow. (B)… Source: Accurate Preoperative and Intraoperative Evaluation Reduces Surgical Costs and Patient Invasiveness in Ventriculoperitoneal Shunt Revision — Cureus 2024; CC BY.
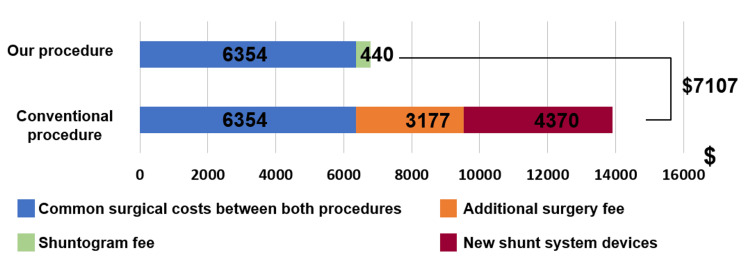 Figure 4. The cost differences between the conventional procedure and the procedure used in this caseConventional shunt revision takes about 135 minutes, whereas our method shortens the process by… Source: Accurate Preoperative and Intraoperative Evaluation Reduces Surgical Costs and Patient Invasiveness in Ventriculoperitoneal Shunt Revision — Cureus 2024; CC BY.
Figure 4. The cost differences between the conventional procedure and the procedure used in this caseConventional shunt revision takes about 135 minutes, whereas our method shortens the process by… Source: Accurate Preoperative and Intraoperative Evaluation Reduces Surgical Costs and Patient Invasiveness in Ventriculoperitoneal Shunt Revision — Cureus 2024; CC BY.
History of Present Illness
- Chief complaint: Return of hydrocephalus symptoms (headache, vomiting, lethargy, decreased consciousness, irritability/bulging fontanelle in infants), OR fever/abdominal pain (infection/pseudocyst), OR positional headache (overdrainage)
- Existing shunt details: type, valve (programmable? setting?), date placed, prior revisions, manufacturer
- Time course (acute deterioration = emergency)
Past Medical History
- Original etiology of hydrocephalus, number/dates of prior revisions, prior infections, peritoneal/distal site history, allergies
- Standard PMH; obtain prior operative notes and shunt cards
Imaging Review
CT/MRI head
- Ventricle size vs the patient’s known baseline (may be unchanged in slit-ventricle malfunction — clinical correlation key), catheter position
Shunt series X-rays (skull, neck, chest, abdomen)
- Disconnection, fracture, migration, kinking, catheter tip position (distal tip out of peritoneum/atrium/pleura)
Abdominal US/CT (if distal failure)
- Pseudocyst, distal catheter position, ascites
Programmable valve
- Recheck/confirm setting (esp. after recent MRI — may have changed)
Labs
- CBC, BMP, Coags, type and screen
- Shunt tap (reservoir, sterile): opening pressure, function (proximal/distal patency), CSF cell count, glucose, protein, Gram stain, culture (infection)
- Inflammatory markers (CRP), blood cultures (if febrile)
Neurological Examination
- Mental status, signs of raised ICP, fontanelle (infants), compare to baseline; abdominal exam (distal)
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: navigation or endoscope as indicated, shunt hardware/valve setting verified, distal-access tools or general surgery help when needed, antibiotic-impregnated catheter availability, and postop imaging plan.
- Special needs: antibiotic timing, programmable valve documentation, abdominal/chest/vascular distal-site plan, CSF culture plan for revision/infection, anticoagulation plan, and EVD backup if access fails.
- Immediate postop orders: neuro checks, CT or shunt-series timing, valve setting documentation and MRI precautions, wound/abdominal/distal-site checks, infection watch, DVT timing, and follow-up for setting adjustment.
Identify the Failure Point (Systematic)
- Proximal obstruction (most common — choroid plexus/debris/ependyma into ventricular catheter)
- Valve malfunction/blockage
- Distal obstruction (pseudocyst, fibrosis, disconnection, migration out of cavity, tip in subcutaneous tissue)
- Disconnection/fracture (shunt series)
- Infection (different pathway — usually externalize/remove)
- Over- vs under-drainage (valve adjustment vs revision)
Position
- Per shunt type (supine, head turned for VP/VA/VPL; lateral for LP); prep entire shunt track if exploring multiple components
Key Surgical Steps (Exploration/Revision)
- Confirm setting (programmable valve) — sometimes “malfunction” is an MRI-altered setting (non-invasive fix)
- Open at the valve/reservoir; assess proximal flow (CSF from ventricular catheter — brisk = proximal patent; none/sluggish = proximal obstruction)
- Assess distal flow (manometer/observe runoff)
- Proximal obstruction: replace ventricular catheter (may use endoscope/navigation; careful — adherent choroid plexus, avoid hemorrhage when removing stuck catheter; may leave a retained fragment if densely adherent rather than avulse vessels)
- Distal obstruction: replace/reposition distal catheter; for pseudocyst — relocate distal catheter to a new site (laparoscopy/new quadrant) or convert to VA/VPL; treat infection if present
- Disconnection/fracture: reconnect/replace the fractured component
- Valve failure: replace valve
- Infection: remove entire shunt, place EVD (externalize), treat with IV antibiotics until CSF sterile, then re-implant new shunt at a new site
- Confirm whole-system flow, document new components/setting
Critical Anatomy & Structures at Risk
- Choroid plexus / ependyma / cortex (removing adherent ventricular catheter — hemorrhage)
- Distal site structures (bowel — pseudocyst/peritoneal; vessels — atrial; lung — pleural)
- Retained/avulsed catheter fragments
Equipment
- Replacement shunt components (catheters, valve — match or upgrade system), connectors
- Endoscope/navigation (proximal revision), manometer
- EVD kit (if infection → externalize), laparoscopy (pseudocyst/distal), antibiotic-impregnated catheters
- Prior op notes / shunt card for component compatibility
Anesthesia
- General; cefazolin (± vancomycin if infection); per shunt type
Potential Complications
- Hemorrhage (removing adherent proximal catheter), recurrent obstruction
- Infection (revision raises infection risk), incomplete correction
- Retained catheter fragment, over/under-drainage after revision
- Distal site complications
Operative Note Template
Preoperative Diagnosis: [VP/VA/LP] shunt malfunction ([obstruction / disconnection / infection / overdrainage])
Postoperative Diagnosis: Same [+ identified failure point]
Procedure: [VP/VA/LP] shunt exploration and revision — [proximal catheter replacement / distal revision / valve replacement / full system removal with EVD for infection]
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Adjuncts: Replacement components, [endoscope/navigation], manometer, [EVD kit / laparoscopy] Implants: [Components replaced — specify] Complications: None
Indications: [Age]yo [M/F] with an existing [VP] shunt presenting with [recurrent hydrocephalus symptoms / fever / overdrainage]. Workup ([CT, shunt series, tap]) suggested [failure point]. Prior op notes/shunt card reviewed. Risks (hemorrhage, infection, recurrent obstruction) discussed.
Description of Procedure: After consent and time-out, [the programmable valve setting was first confirmed]. The shunt was opened at the valve/reservoir and proximal flow assessed (CSF return = patent; none/sluggish = proximal obstruction) and distal flow assessed (manometer/runoff). The failure point was identified as [proximal catheter obstruction / distal obstruction or pseudocyst / disconnection / valve failure / infection].
[Proximal: the ventricular catheter was replaced (endoscope/navigation-assisted; densely adherent choroid plexus managed without avulsion).] [Distal: the peritoneal catheter was repositioned/replaced (or relocated for pseudocyst).] [Valve: replaced.] [Disconnection: reconnected/replaced.] [Infection: the entire shunt was removed, an EVD placed, and re-implantation deferred until CSF sterile.] Whole-system flow was confirmed and the new components/valve setting documented.
The patient was transferred [to the floor / ICU if EVD]; the shunt card/records were updated.
Postoperative Plan
- Floor/step-down (ICU if infected/EVD), neuro checks, compare to baseline
- CT head (ventricles), shunt series baseline (new configuration), document new valve/setting
- If infection: EVD management, IV antibiotics per culture, re-shunt when CSF sterile
- Monitor for recurrent malfunction; update shunt card/records
- Follow-up imaging; educate family on malfunction signs
Chief-Level Case Review
Use these as the senior-level mental model for Shunt Revision / Exploration:
- Decision point: Trajectory and hardware choice should follow the failure mode: obstruction, infection, overdrainage, loculation, slit ventricle, distal failure, or wrong pressure setting.
- Technical lever: Document the system: entry point, catheter target/depth, valve type and setting, distal site, antibiotic-impregnated hardware, and what imaging confirms placement.
- Bailout: Rescue plan is practical: poor CSF return, bloody CSF, malposition, distal access failure, abdominal/pleural complication, or inability to safely pass the catheter.
- Postop watch: Postop orders must be unambiguous: drain height/rate/max output, valve setting, clamp parameters, imaging, antibiotics, ICP/neuro checks, and overdrainage precautions.
Common Pimp Questions
Use these to pressure-test preparation for Shunt Revision / Exploration:
- What is the working CSF physiology problem: obstruction, absorption failure, overdrainage, infection, or catheter failure?
- Where exactly is the entry point, target, and backup trajectory?
- What valve, catheter, endoscope, or navigation preference does the attending use?
- What is the infection-prevention plan and what cultures/CSF studies are needed?
- What postop imaging, valve setting, drainage level, and neuro-check plan should be written?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Valve brand/setting, antibiotic catheter use, and tunneling side: [attending-specific]
- Navigation/endoscope/stylet preference and ventricular target: [attending-specific]
- CSF culture/lab routine and perioperative antibiotic duration: [attending-specific]
- Postop scan timing, EVD height or valve verification, and activity restrictions: [attending-specific]