
Case Prep: Lumboperitoneal (LP) Shunt Placement
Case / Approach Snapshot
- Anatomy at risk: entry point, ventricular target, choroid plexus and deep veins, cortical vessels, eloquent cortex/tracts, catheter path, and distal hardware route.
- Operative steps: confirm indication and side, plan trajectory, prepare hardware, access ventricle or cistern safely, confirm flow/position, tunnel/connect devices when needed, and define infection/obstruction surveillance; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: malposition, hemorrhage, poor CSF return, overdrainage/underdrainage, obstruction, infection, abdominal/pleural complication, slit ventricles, and revision algorithm.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [idiopathic intracranial hypertension (IIH/pseudotumor) / communicating hydrocephalus / CSF leak / NPH] planned for lumboperitoneal shunt placement [with horizontal-vertical or programmable valve].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Incidence of radiculopathy following lumboperitoneal shunt placement without fluoroscopy for normal pressure hydrocephalus — Tanaka T. Surgical neurology international 2022. PubMed
- Early postoperative lumbar catheter severing in a lumboperitoneal shunt due to bite-off by the spinous processes following a fall on the buttocks: illustrative case — Munakata R. Journal of neurosurgery. Case lessons 2024. PubMed
- Rare complication of lumboperitoneal shunt with distal catheter migration into the inguinal hernia sac in two adults: A case report — Tanaka T. Surgical neurology international 2023. PubMed
- Laparoscopic transabdominal lumboperitoneal shunt — Huie F. Surgical endoscopy 1999. PubMed
- Creating of “fascial sheath” around subcutaneous lumboperitoneal shunt catheters largely prevents postoperative subcutaneous shunt catheter migration — Tanaka T. Surgical neurology international 2022. PubMed
- Minimizing complications in lumboperitoneal shunt for normal pressure hydrocephalus: Technical note and case series — Pisano P. Surgical neurology international 2026. PubMed
- Intra-bronchial migration of peritoneal catheter of lumboperitoneal shunt — Kawahara T. Surgical neurology international 2015. PubMed
- New lumboperitoneal shunt catheter — Selman WR. Surgical neurology 1984. PubMed
- Late intrathecal retraction of a lumboperitoneal shunt — Kim YJ. Surgical neurology international 2023. PubMed
- Use of Pneumoperitoneal Puncture for Peritoneal Catheter Placement in Lumboperitoneal Shunt Surgery: Technical Note — He J. World neurosurgery 2017. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
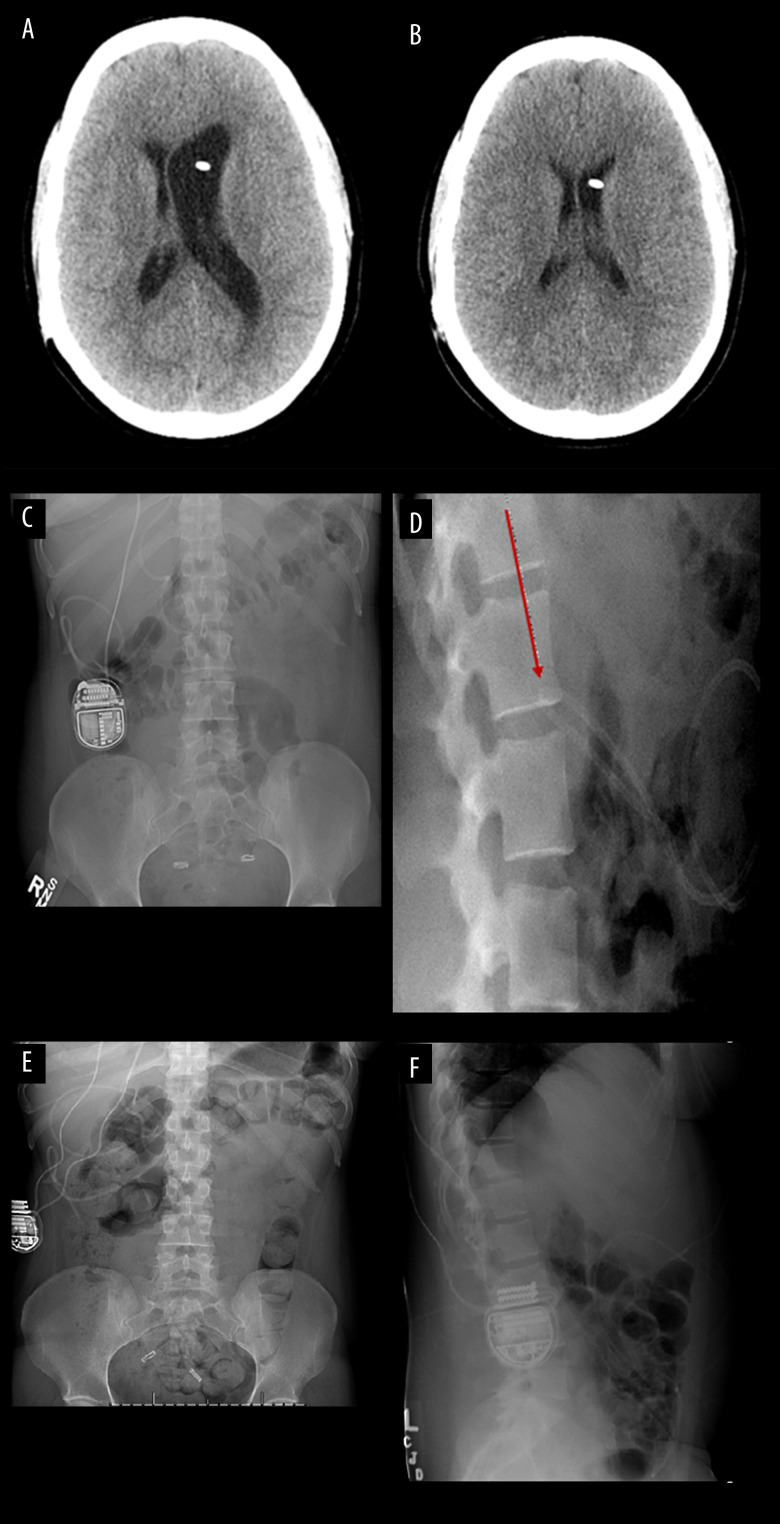 Figure 1.. Axial computed tomography (CT) scan depicting enlarged ventricles. (A) compared to prior CT scan (B) concerning for shunt failure. Anteroposterior (C) and lateral (D) shunt series X-rays… Source: Ventriculoperitoneal Shunt Failure Due to Distal Peritoneal Catheter Kinking — The American Journal of Case Reports 2022; CC BY-NC-ND.
Figure 1.. Axial computed tomography (CT) scan depicting enlarged ventricles. (A) compared to prior CT scan (B) concerning for shunt failure. Anteroposterior (C) and lateral (D) shunt series X-rays… Source: Ventriculoperitoneal Shunt Failure Due to Distal Peritoneal Catheter Kinking — The American Journal of Case Reports 2022; CC BY-NC-ND.
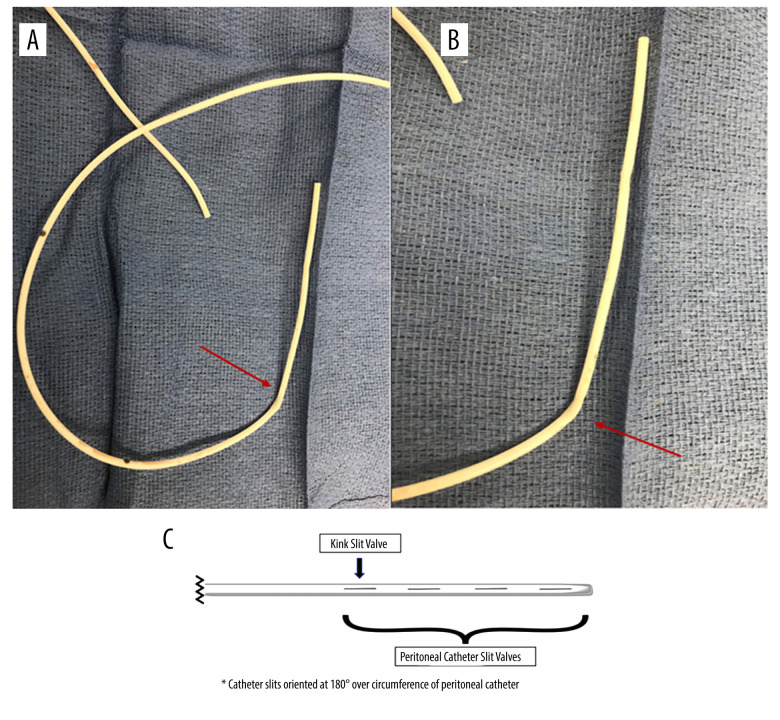 Figure 2.. Intraoperative images (A, B) demonstrating kinking of the distal catheter at the site of the distal peritoneal slit valves (arrow). Illustration (C) depicting the location of the… Source: Ventriculoperitoneal Shunt Failure Due to Distal Peritoneal Catheter Kinking — The American Journal of Case Reports 2022; CC BY-NC-ND.
Figure 2.. Intraoperative images (A, B) demonstrating kinking of the distal catheter at the site of the distal peritoneal slit valves (arrow). Illustration (C) depicting the location of the… Source: Ventriculoperitoneal Shunt Failure Due to Distal Peritoneal Catheter Kinking — The American Journal of Case Reports 2022; CC BY-NC-ND.
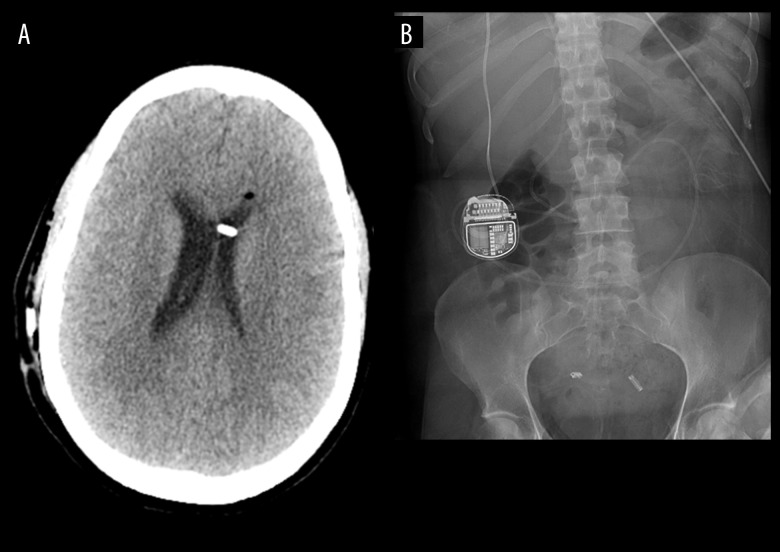 Figure 3.. Axial postoperative computed tomography (CT) scan depicting interval decrease in the size of the ventricles (A). Shunt series X-rays demonstrating intact shunt system with no kinking or… Source: Ventriculoperitoneal Shunt Failure Due to Distal Peritoneal Catheter Kinking — The American Journal of Case Reports 2022; CC BY-NC-ND.
Figure 3.. Axial postoperative computed tomography (CT) scan depicting interval decrease in the size of the ventricles (A). Shunt series X-rays demonstrating intact shunt system with no kinking or… Source: Ventriculoperitoneal Shunt Failure Due to Distal Peritoneal Catheter Kinking — The American Journal of Case Reports 2022; CC BY-NC-ND.
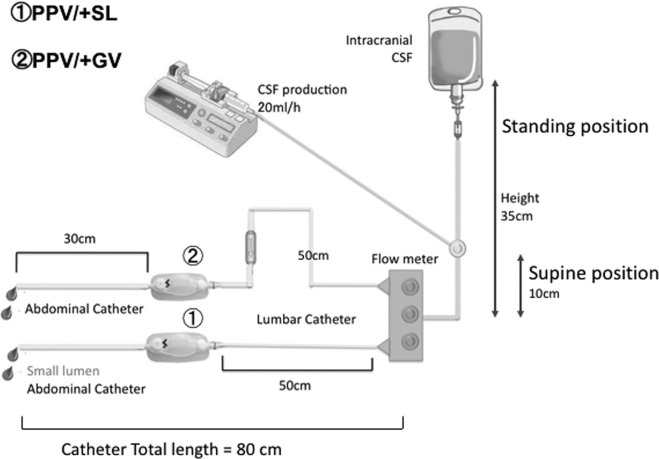 FIGURE 1.. Shunt system experiments. Based on previous studies, we set the standing (vertical) pressure at 35 cmH2O and the supine (horizontal) position pressure at 10 cmH2O. We simulated CSF… Source: Lumboperitoneal Shunts for the Treatment of Idiopathic Normal Pressure Hydrocephalus: A Comparison of Small-Lumen Abdominal Catheters to Gravitational Add-On Valves in a Single Center — Operative Neurosurgery 2018; CC BY.
FIGURE 1.. Shunt system experiments. Based on previous studies, we set the standing (vertical) pressure at 35 cmH2O and the supine (horizontal) position pressure at 10 cmH2O. We simulated CSF… Source: Lumboperitoneal Shunts for the Treatment of Idiopathic Normal Pressure Hydrocephalus: A Comparison of Small-Lumen Abdominal Catheters to Gravitational Add-On Valves in a Single Center — Operative Neurosurgery 2018; CC BY.
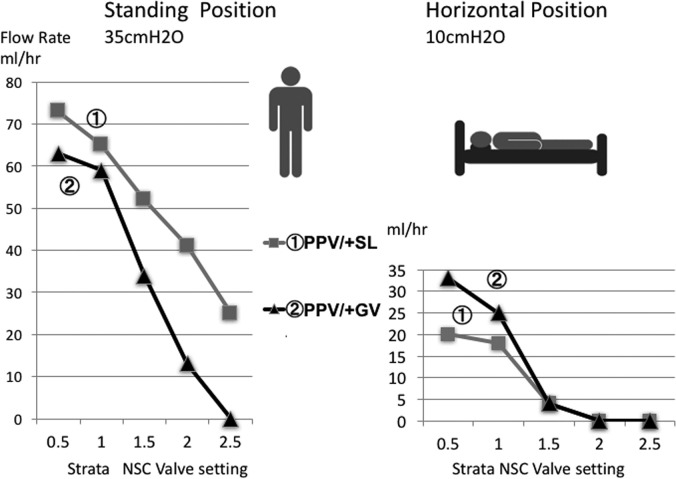 FIGURE 2.. Comparison between the small-lumen abdominal catheter and gravitational add-on valve. We measured the flow rate (mL/h) at simulated standing (35 cmH2O) and supine (10 cmH2O) positions… Source: Lumboperitoneal Shunts for the Treatment of Idiopathic Normal Pressure Hydrocephalus: A Comparison of Small-Lumen Abdominal Catheters to Gravitational Add-On Valves in a Single Center — Operative Neurosurgery 2018; CC BY.
FIGURE 2.. Comparison between the small-lumen abdominal catheter and gravitational add-on valve. We measured the flow rate (mL/h) at simulated standing (35 cmH2O) and supine (10 cmH2O) positions… Source: Lumboperitoneal Shunts for the Treatment of Idiopathic Normal Pressure Hydrocephalus: A Comparison of Small-Lumen Abdominal Catheters to Gravitational Add-On Valves in a Single Center — Operative Neurosurgery 2018; CC BY.
 FIGURE 4.. A lumbar 3-dimensional image obtained after LPS implantation with a gravity add-on valve and a Strata NSC programmable pressure valve. Source: Lumboperitoneal Shunts for the Treatment of Idiopathic Normal Pressure Hydrocephalus: A Comparison of Small-Lumen Abdominal Catheters to Gravitational Add-On Valves in a Single Center — Operative Neurosurgery 2018; CC BY.
FIGURE 4.. A lumbar 3-dimensional image obtained after LPS implantation with a gravity add-on valve and a Strata NSC programmable pressure valve. Source: Lumboperitoneal Shunts for the Treatment of Idiopathic Normal Pressure Hydrocephalus: A Comparison of Small-Lumen Abdominal Catheters to Gravitational Add-On Valves in a Single Center — Operative Neurosurgery 2018; CC BY.
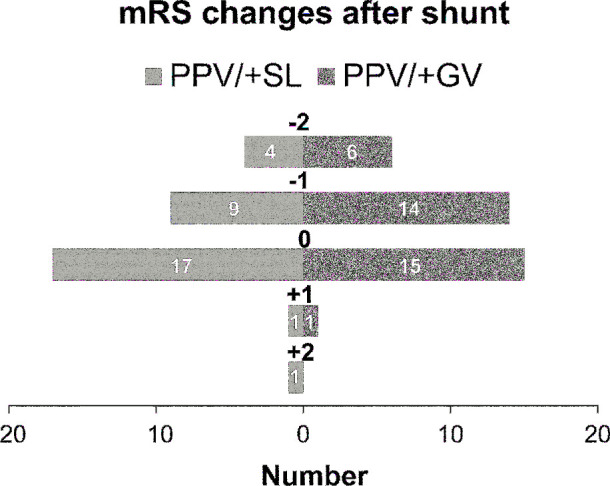 FIGURE 5.. mRS score changes after LPS implantation. Source: Lumboperitoneal Shunts for the Treatment of Idiopathic Normal Pressure Hydrocephalus: A Comparison of Small-Lumen Abdominal Catheters to Gravitational Add-On Valves in a Single Center — Operative Neurosurgery 2018; CC BY.
FIGURE 5.. mRS score changes after LPS implantation. Source: Lumboperitoneal Shunts for the Treatment of Idiopathic Normal Pressure Hydrocephalus: A Comparison of Small-Lumen Abdominal Catheters to Gravitational Add-On Valves in a Single Center — Operative Neurosurgery 2018; CC BY.
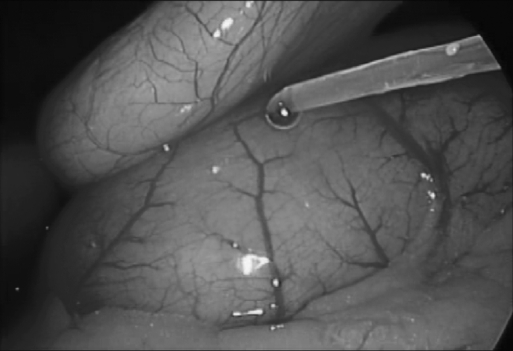 Figure 1.. Flow of cerebrospinal fluid is confirmed visually after lumboperitoneal shunt placement. Source: Laparoscopic Management of Ventriculoperitoneal and Lumboperitoneal Shunt Complications — JSLS : Journal of the Society of Laparoendoscopic Surgeons 2007; CC BY-NC-ND.
Figure 1.. Flow of cerebrospinal fluid is confirmed visually after lumboperitoneal shunt placement. Source: Laparoscopic Management of Ventriculoperitoneal and Lumboperitoneal Shunt Complications — JSLS : Journal of the Society of Laparoendoscopic Surgeons 2007; CC BY-NC-ND.
 Figure 2.. Foreign body-detached prior shunt is visualized and retrieved. Source: Laparoscopic Management of Ventriculoperitoneal and Lumboperitoneal Shunt Complications — JSLS : Journal of the Society of Laparoendoscopic Surgeons 2007; CC BY-NC-ND.
Figure 2.. Foreign body-detached prior shunt is visualized and retrieved. Source: Laparoscopic Management of Ventriculoperitoneal and Lumboperitoneal Shunt Complications — JSLS : Journal of the Society of Laparoendoscopic Surgeons 2007; CC BY-NC-ND.
History of Present Illness
- Chief complaint: IIH (headache, papilledema, visual loss, pulsatile tinnitus, diplopia/CN VI), communicating hydrocephalus, or persistent CSF leak
- LP requires communicating CSF spaces (CSF must flow from cranial to lumbar — NOT for obstructive hydrocephalus)
- IIH: failed medical therapy (acetazolamide, weight loss), progressive visual loss; LP shunt or VP shunt or venous sinus stenting options
- LP function harder to assess clinically (no easily tappable reservoir)
Past Medical History
- Obesity (IIH association; also affects peritoneal catheter, abdominal pressure)
- Chiari/tonsillar position (LP overdrainage can cause acquired tonsillar herniation), prior lumbar surgery/arthritis, scoliosis
- Standard PMH
Imaging Review
MRI brain
- Exclude obstructive hydrocephalus and mass (LP only for communicating), signs of IIH (empty sella, flattened globes, optic nerve tortuosity, slit ventricles), tonsillar position (baseline — overdrainage risk)
MRV
- Venous sinus stenosis (IIH — consider stenting alternative)
Lumbar imaging
- Anatomy for catheter placement
LP/opening pressure
- Elevated OP confirms IIH; CSF studies
Labs
- CBC, BMP, Coags, type and screen
Neurological Examination
- Visual acuity, fields, fundoscopy (papilledema), CN VI, headache; baseline for IIH
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: navigation or endoscope as indicated, shunt hardware/valve setting verified, distal-access tools or general surgery help when needed, antibiotic-impregnated catheter availability, and postop imaging plan.
- Special needs: antibiotic timing, programmable valve documentation, abdominal/chest/vascular distal-site plan, CSF culture plan for revision/infection, anticoagulation plan, and EVD backup if access fails.
- Immediate postop orders: neuro checks, CT or shunt-series timing, valve setting documentation and MRI precautions, wound/abdominal/distal-site checks, infection watch, DVT timing, and follow-up for setting adjustment.
Valve / Overdrainage Consideration
- Overdrainage is the central challenge (siphoning when upright); use horizontal-vertical valve, gravitational, or programmable valve to reduce postural overdrainage and low-pressure headaches
Position
- Lateral decubitus (lumbar puncture position), flexed; then access abdomen (may reposition)
Key Surgical Steps
- Lumbar (proximal) catheter: Tuohy needle into the L3-4 or L4-5 subarachnoid space (paramedian), confirm CSF flow, thread the lumbar catheter cephalad into the thecal sac several cm; remove needle over catheter (never withdraw catheter through needle — shears)
- Anchor at the lumbar fascia (avoid kinking; some tunnel through a small fascial incision)
- Tunnel the catheter subcutaneously around the flank to the abdomen
- Peritoneal (distal) catheter: small abdominal incision (as VP), enter peritoneum, insert distal catheter
- Interpose valve (horizontal-vertical/programmable/anti-siphon) along the system (often at the flank)
- Confirm CSF flow through the system; closure
- (Some use fluoroscopy to confirm lumbar catheter position)
Critical Anatomy & Structures at Risk
- Lumbar nerve roots / cauda equina (catheter — radicular pain)
- Conus medullaris (stay below L2)
- Peritoneum/bowel (abdominal entry)
- Overdrainage → acquired Chiari/tonsillar herniation, low-pressure headaches
Equipment
- LP shunt kit (Tuohy needle, lumbar catheter), horizontal-vertical/programmable valve, peritoneal catheter
- Fluoroscopy (optional), antibiotic-impregnated catheter, tunneler
Anesthesia
- General (or local/sedation for parts); cefazolin
Potential Complications
- Overdrainage — low-pressure/postural headache, acquired Chiari I / tonsillar herniation, slit ventricles
- Difficult to assess function/obstruction (no tappable reservoir), radiculopathy, lumbar catheter migration
- Infection, CSF leak at lumbar site, peritoneal complications
- Catheter fracture/migration, scoliosis/arthritis limiting placement (children)
Operative Note Template
Preoperative Diagnosis: [Idiopathic intracranial hypertension / communicating hydrocephalus / CSF leak]
Postoperative Diagnosis: Same
Procedure: Lumboperitoneal shunt placement with [horizontal-vertical / programmable] valve
Surgeon / Assistant: Anesthesia: General endotracheal [or local + sedation] EBL / Fluids: Adjuncts: Tuohy needle, [fluoroscopy], tunneler Implants: Lumbar (subarachnoid) catheter, horizontal-vertical/programmable valve, peritoneal catheter Complications: None
Indications: [Age]yo [M/F] with [IIH with visual symptoms / communicating hydrocephalus] and confirmed communicating CSF spaces (no obstructive lesion/mass). Risks (overdrainage, acquired Chiari, difficult function assessment) discussed.
Description of Procedure: After consent and time-out, the patient was positioned in lateral decubitus. A Tuohy needle was placed into the L3-4/L4-5 subarachnoid space (paramedian) with CSF return confirmed, and the lumbar catheter threaded cephalad several centimeters; the needle was removed over the catheter (never withdrawing the catheter through the needle). The catheter was anchored at the lumbar fascia and tunneled around the flank to a small abdominal incision, where the peritoneum was entered and the distal catheter inserted.
A horizontal-vertical/programmable valve was interposed to limit postural overdrainage, and CSF flow through the system confirmed before closure.
The patient was transferred with monitoring for overdrainage (postural headache) and visual follow-up (IIH).
Postoperative Plan
- Floor, neuro checks, visual/headache assessment (IIH), watch for overdrainage (positional headache → may need to raise programmable setting)
- Ophthalmology follow-up (papilledema/visual fields — IIH)
- Shunt series baseline (LP shunt films), document valve setting
- Monitor for acquired Chiari symptoms; counsel that LP function is harder to assess (clinical/imaging follow-up)
- Weight management/medical therapy continuation (IIH)
Chief-Level Case Review
Use these as the senior-level mental model for Lumboperitoneal (LP) Shunt Placement:
- Decision point: Trajectory and hardware choice should follow the failure mode: obstruction, infection, overdrainage, loculation, slit ventricle, distal failure, or wrong pressure setting.
- Technical lever: Document the system: entry point, catheter target/depth, valve type and setting, distal site, antibiotic-impregnated hardware, and what imaging confirms placement.
- Bailout: Rescue plan is practical: poor CSF return, bloody CSF, malposition, distal access failure, abdominal/pleural complication, or inability to safely pass the catheter.
- Postop watch: Postop orders must be unambiguous: drain height/rate/max output, valve setting, clamp parameters, imaging, antibiotics, ICP/neuro checks, and overdrainage precautions.
Common Pimp Questions
Use these to pressure-test preparation for Lumboperitoneal (LP) Shunt Placement:
- What is the working CSF physiology problem: obstruction, absorption failure, overdrainage, infection, or catheter failure?
- Where exactly is the entry point, target, and backup trajectory?
- What valve, catheter, endoscope, or navigation preference does the attending use?
- What is the infection-prevention plan and what cultures/CSF studies are needed?
- What postop imaging, valve setting, drainage level, and neuro-check plan should be written?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Valve brand/setting, antibiotic catheter use, and tunneling side: [attending-specific]
- Navigation/endoscope/stylet preference and ventricular target: [attending-specific]
- CSF culture/lab routine and perioperative antibiotic duration: [attending-specific]
- Postop scan timing, EVD height or valve verification, and activity restrictions: [attending-specific]