
Case Prep: Lumbar Drain Placement
Case / Approach Snapshot
- Anatomy at risk: entry point, ventricular target, choroid plexus and deep veins, cortical vessels, eloquent cortex/tracts, catheter path, and distal hardware route.
- Operative steps: confirm indication and side, plan trajectory, prepare hardware, access ventricle or cistern safely, confirm flow/position, tunnel/connect devices when needed, and define infection/obstruction surveillance; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: malposition, hemorrhage, poor CSF return, overdrainage/underdrainage, obstruction, infection, abdominal/pleural complication, slit ventricles, and revision algorithm.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] requiring lumbar CSF drainage for [CSF leak / skull base surgery / NPH trial / TAAA spinal cord protection / pseudomeningocele] planned for lumbar drain placement.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Letter: Lumbar Drain Placement in Acute Spinal Cord Injury is Safe: A Review of Available Evidence — Kolcun JPG. Operative neurosurgery (Hagerstown, Md.) 2023. PubMed
- Tunneled lumbar drain. Technical note — Hahn M. Journal of neurosurgery 2002. PubMed
- Lumbar drain — Shimizu S. Journal of neurosurgery 2003. PubMed
- External lumbar drain for fistula leakage in posterior fossa and spinal surgery: a systematic review with meta-analysis — Falcão L. Neurosurgical review 2025. PubMed
- Efficacy and Safety of Intraoperative Lumbar Drain in Endoscopic Skull Base Tumor Resection: A Meta-Analysis — Guo X. Frontiers in oncology 2020. PubMed
- Fluoroscopic-guided Lumbar Subarachnoid Drain Placement: A Technical Report — Lloyd JT. Journal of cardiothoracic and vascular anesthesia 2025. PubMed
- Lumbar drain trial outcomes of normal pressure hydrocephalus: a single-center experience of 254 patients — El Ahmadieh TY. Journal of neurosurgery 2020. PubMed
- Development of a Lumbar Drain Simulator for Instructional Technique and Skill Assessment — Clifton WE. Neurocritical care 2020. PubMed
- Brainstem Hemorrhage Following Lumbar Drain for Post-traumatic Hydrocephalus — Carr MT. Cureus 2022. PubMed
- Lumbar Drain Use during Middle Fossa Approaches for Nonneoplastic Pathology of the Skull Base — Dambrino RJ. Journal of neurological surgery. Part B, Skull base 2024. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
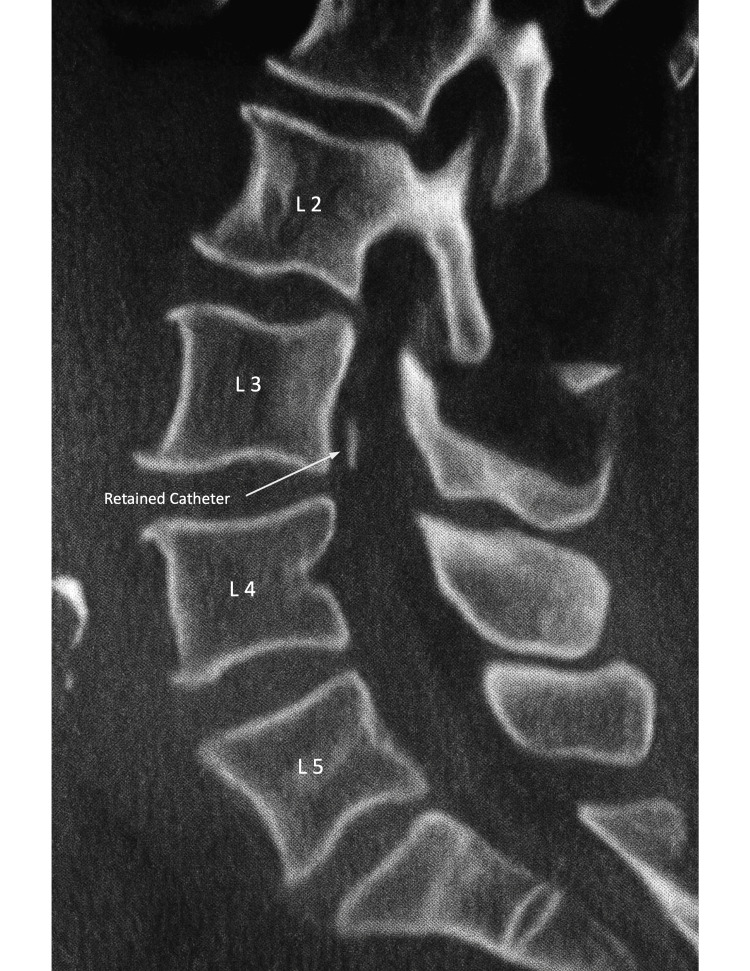 Figure 1. Lumbar spine CTSagittal (lateral) view. Vertebral levels are labeled for orientation. The arrow indicates the retained catheter fragment within the intrathecal space. Source: Retained Lumbar Drain Tip Leading to Intrathecal Hematoma: A Case Report on Perioperative Risks and Management — Cureus 2025; CC BY.
Figure 1. Lumbar spine CTSagittal (lateral) view. Vertebral levels are labeled for orientation. The arrow indicates the retained catheter fragment within the intrathecal space. Source: Retained Lumbar Drain Tip Leading to Intrathecal Hematoma: A Case Report on Perioperative Risks and Management — Cureus 2025; CC BY.
 Figure 2. Lumbar spine CT Coronal view. The arrow indicates the retained catheter fragment. Source: Retained Lumbar Drain Tip Leading to Intrathecal Hematoma: A Case Report on Perioperative Risks and Management — Cureus 2025; CC BY.
Figure 2. Lumbar spine CT Coronal view. The arrow indicates the retained catheter fragment. Source: Retained Lumbar Drain Tip Leading to Intrathecal Hematoma: A Case Report on Perioperative Risks and Management — Cureus 2025; CC BY.
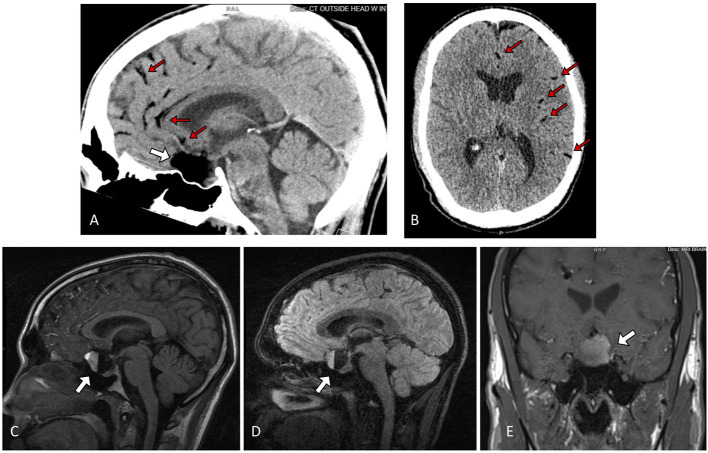 Figure 1. Sagittal (A) and Axial (B) non contrast Head CT showing a hypodense lesion in the sella/suprasellar region (white arrow), with associated scattered hypodense globules along the… Source: Ruptured Suprasellar Dermoid Cyst Treated With Lumbar Drain to Prevent Postoperative Hydrocephalus: Case Report and Focused Review of Literature — Frontiers in Surgery 2021; CC BY.
Figure 1. Sagittal (A) and Axial (B) non contrast Head CT showing a hypodense lesion in the sella/suprasellar region (white arrow), with associated scattered hypodense globules along the… Source: Ruptured Suprasellar Dermoid Cyst Treated With Lumbar Drain to Prevent Postoperative Hydrocephalus: Case Report and Focused Review of Literature — Frontiers in Surgery 2021; CC BY.
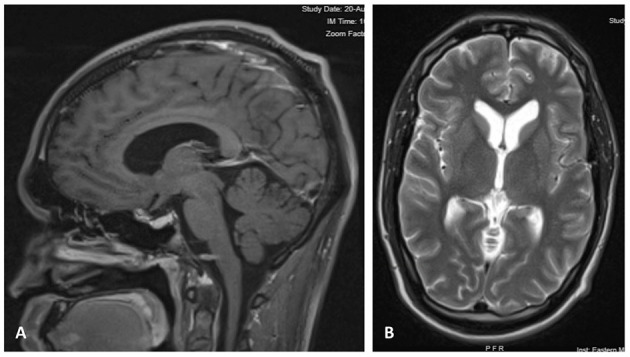 Figure 2. (A) Contrast-enhanced Sagittal T1 image 6 months after craniotomy, showing decompression of the sellar region with resolved mass effect over the optic pathway. (B) Axial T2 MRI at 6… Source: Ruptured Suprasellar Dermoid Cyst Treated With Lumbar Drain to Prevent Postoperative Hydrocephalus: Case Report and Focused Review of Literature — Frontiers in Surgery 2021; CC BY.
Figure 2. (A) Contrast-enhanced Sagittal T1 image 6 months after craniotomy, showing decompression of the sellar region with resolved mass effect over the optic pathway. (B) Axial T2 MRI at 6… Source: Ruptured Suprasellar Dermoid Cyst Treated With Lumbar Drain to Prevent Postoperative Hydrocephalus: Case Report and Focused Review of Literature — Frontiers in Surgery 2021; CC BY.
History of Present Illness / Indication
- Indications:
- CSF leak (spontaneous, post-op, post-traumatic rhinorrhea/otorrhea) — divert CSF to allow healing
- Skull base/posterior fossa surgery (brain relaxation, post-op leak prevention)
- NPH evaluation (lumbar drain trial — sustained drainage to predict shunt response)
- Thoracoabdominal aortic aneurysm repair (spinal cord perfusion protection)
- Pseudomeningocele, post-dural puncture management
- Intrathecal access/pressure monitoring
Imaging Review
MRI/CT Lumbar Spine (if anatomy concern)
- Lumbar level patency, spinal canal, no mass/Chiari (contraindicated if obstructive hydrocephalus or posterior fossa mass with downward pressure gradient → herniation risk)
- Rule out elevated ICP from mass lesion before lumbar drainage
Labs
- CBC (Plt > 50-100K), Coags (INR < 1.4) — correct before placement
Neurological Examination
- Baseline; document for NPH trial (gait, cognition)
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: sterile lumbar-drain kit, fluoroscopy if difficult anatomy, collection system, and clear labeling of catheter depth/entry level.
- Special needs: anticoagulation/coagulopathy plan, antibiotics per protocol, strict drainage maximum per hour, headache/overdrainage monitoring, and clamp parameters for ambulation or neurologic change.
- Immediate postop orders: drain height/rate/maximum output, neuro checks, bedrest/ambulation rules, headache/nausea management, daily need review, CSF sampling only if indicated, and removal timing.
Contraindications
- Obstructive hydrocephalus / posterior fossa mass / large supratentorial mass with shift (herniation risk)
- Coagulopathy, infection at site, blocked spinal CSF spaces
Indication-Specific Drainage Goals
| Indication | Typical goal | Practical endpoint |
|---|---|---|
| Skull-base CSF leak | Lower CSF pressure across repair without overdrainage | Dry nose/ear/wound, stable neuro exam, no pneumocephalus expansion |
| Endoscopic skull-base surgery adjunct | Protect high-flow repair in selected cases | No leak with mobilization/Valsalva challenge per team protocol |
| Posterior fossa wound leak or pseudomeningocele | Divert CSF from wound while soft tissues seal | Flattening collection, dry incision, no meningitis |
| NPH lumbar drain trial | Sustained drainage to test shunt responsiveness | Objective gait/cognition improvement compared with baseline |
| Thoracoabdominal aortic repair | Maintain spinal cord perfusion pressure | Protocolized CSF pressure/output with MAP augmentation |
Pre-Placement Safety Read
- Review head imaging for mass lesion, obstructive hydrocephalus, posterior fossa crowding, Chiari, or cisternal effacement before draining lumbar CSF.
- Review spine imaging if prior lumbar surgery, scoliosis, severe stenosis, infection, or unclear level anatomy.
- Correct anticoagulation/antiplatelet effect using neuraxial-procedure standards and local anesthesia guidelines.
- Clarify the order set before placement: drain height or hourly volume cap, clamp rules, maximum daily output, sampling frequency, and escalation triggers.
Position
- Lateral decubitus (knees-to-chest, flexed) or sitting; standard LP positioning
Key Steps
- Identify level — L3-4 or L4-5 (below conus, ~L1-2); palpate iliac crests (intercristal line ~ L4)
- Sterile prep and drape, local anesthesia
- Insert Tuohy needle (14g) into subarachnoid space, confirm CSF flow
- Thread the lumbar catheter through the needle (cephalad), advance ~5-8 cm into the intrathecal space
- Remove needle over catheter (do not withdraw catheter through needle — shears it)
- Confirm CSF flow through catheter
- Secure/tunnel catheter, apply occlusive dressing, connect to closed drainage system
- Set drainage level/rate (e.g., 10-15 mL/hr, or to a pressure level)
Critical Considerations
- Over-drainage — most dangerous; can cause tonsillar herniation, subdural hematoma, tension pneumocephalus, abducens palsy. Strict rate control, never open to gravity uncontrolled
- Conus medullaris — stay below L2
- Nerve roots (radicular pain on threading — reposition)
Troubleshooting During Placement
- No CSF return: confirm level and midline, rotate bevel, advance in tiny increments, reassess patient flexion, use ultrasound/fluoroscopy if anatomy is difficult, and do not repeatedly traumatize a bloody tap.
- Bloody CSF: distinguish traumatic tap from subarachnoid blood by clearing trend and clinical context; avoid advancing a catheter through persistently bloody return unless the indication justifies it and the team accepts hemorrhage risk.
- Radicular pain while threading: stop advancing, withdraw slightly, rotate/reposition, and retry; persistent pain means the catheter is irritating a root.
- Catheter will not thread: ensure free CSF flow, reduce needle angle, avoid forcing, and consider a different level or fluoroscopic guidance.
- Catheter shearing risk: never pull the catheter back through the Tuohy needle; remove needle and catheter together if repositioning is required.
Equipment
- Lumbar drain kit (Tuohy needle, catheter, closed drainage system with graduated chamber)
- Sterile prep, local anesthetic
Potential Complications
- Over-drainage → herniation, subdural hematoma, pneumocephalus, CN VI palsy, severe positional headache
- Infection (meningitis) — sterile technique, limit duration
- Catheter retention/shearing/fracture, nerve root irritation
- Failure/dislodgement, CSF leak at site
Operative/Procedure Note Template
Preoperative Diagnosis: [CSF leak / skull-base surgery adjunct / NPH trial / spinal cord protection]
Postoperative Diagnosis: Same
Procedure: Lumbar drain placement
Performed by: Anesthesia: [Local ± sedation / general] Adjuncts: Lumbar drain kit (Tuohy needle, catheter, closed graduated drainage system) Complications: None
Indications: [Age]yo [M/F] requiring controlled lumbar CSF drainage for [indication]. Obstructive hydrocephalus/posterior fossa mass excluded (herniation risk). Coagulation parameters corrected. Risks (overdrainage/herniation, infection, headache) discussed.
Description of Procedure: With the patient in [lateral decubitus/sitting] and sterile prep/drape, local anesthesia was infiltrated at [L3-4 / L4-5] (below the conus). A Tuohy needle was advanced into the subarachnoid space with CSF flow confirmed, and the lumbar catheter threaded cephalad ~5–8 cm; the needle was removed over the catheter (never withdrawing the catheter through the needle). CSF flow through the catheter was reconfirmed, the catheter secured with an occlusive dressing, and connected to a closed graduated drainage system set to [10–15 mL/hr / a pressure level].
The patient was transferred with a strict controlled-drainage nursing protocol (clamp for transfers/position changes) and neuro monitoring for overdrainage.
Postoperative / Management Plan
- Controlled drainage — specify rate (e.g., 10-15 mL/hr) or pressure level; never uncontrolled gravity drainage
- Strict nursing protocol: clamp during position changes/transport; monitor hourly output
- Neuro checks q1-2h; watch for over-drainage (severe headache, decreased consciousness, new CN VI palsy → clamp drain, CT)
- Flat or low HOB initially per indication
- CSF sampling for infection surveillance per protocol; limit duration (infection risk rises after ~5 days)
- NPH trial: assess gait/cognition before and during drainage (response predicts shunt benefit)
- Removal: clamp trial, then remove; check site
Drain Management Pearls
- Treat the drain as a medication: the ordered drainage rate/height is the dose, and nursing handoff should include the current level, hourly output, clamp status, and neurologic exam.
- Clamp for transport, bed-height changes, ambulation, coughing fits, and any acute headache or neurologic change until the team reassesses.
- If output suddenly stops, inspect for kinks, closed stopcocks, dependent loops, clot/debris, and patient position before flushing; preserve sterility and avoid injecting unless protocol allows it.
- If output suddenly increases, clamp immediately, assess exam/headache, check for bed-height error or chamber malposition, and image if symptoms suggest subdural, herniation, or pneumocephalus.
- Remove as soon as the indication is met; prolonged dwell time increases infection and dislodgement risk.
Chief-Level Case Review
Use these as the senior-level mental model for Lumbar Drain Placement:
- Decision point: Trajectory and hardware choice should follow the failure mode: obstruction, infection, overdrainage, loculation, slit ventricle, distal failure, or wrong pressure setting.
- Technical lever: Document the system: entry point, catheter target/depth, valve type and setting, distal site, antibiotic-impregnated hardware, and what imaging confirms placement.
- Bailout: Rescue plan is practical: poor CSF return, bloody CSF, malposition, distal access failure, abdominal/pleural complication, or inability to safely pass the catheter.
- Postop watch: Postop orders must be unambiguous: drain height/rate/max output, valve setting, clamp parameters, imaging, antibiotics, ICP/neuro checks, and overdrainage precautions.
Common Pimp Questions
Use these to pressure-test preparation for Lumbar Drain Placement:
- What is the working CSF physiology problem: obstruction, absorption failure, overdrainage, infection, or catheter failure?
- Where exactly is the entry point, target, and backup trajectory?
- What valve, catheter, endoscope, or navigation preference does the attending use?
- What is the infection-prevention plan and what cultures/CSF studies are needed?
- What postop imaging, valve setting, drainage level, and neuro-check plan should be written?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Valve brand/setting, antibiotic catheter use, and tunneling side: [attending-specific]
- Navigation/endoscope/stylet preference and ventricular target: [attending-specific]
- CSF culture/lab routine and perioperative antibiotic duration: [attending-specific]
- Postop scan timing, EVD height or valve verification, and activity restrictions: [attending-specific]