
Case Prep: Endoscopic Third Ventriculostomy (ETV)
Case / Approach Snapshot
- Anatomy at risk: entry point, ventricular target, choroid plexus and deep veins, cortical vessels, eloquent cortex/tracts, catheter path, and distal hardware route.
- Operative steps: confirm indication and side, plan trajectory, prepare hardware, access ventricle or cistern safely, confirm flow/position, tunnel/connect devices when needed, and define infection/obstruction surveillance; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: malposition, hemorrhage, poor CSF return, overdrainage/underdrainage, obstruction, infection, abdominal/pleural complication, slit ventricles, and revision algorithm.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with obstructive (non-communicating) hydrocephalus due to [aqueductal stenosis / tectal or pineal tumor / posterior fossa mass] planned for endoscopic third ventriculostomy [± endoscopic biopsy].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Failure of Endoscopic Third Ventriculostomy — Lane J. Cureus 2022. PubMed
- Endoscopic Third Ventriculostomy - A Review — Yadav YR. Neurology India 2021. PubMed
- [Neuroendoscopic Third Ventriculostomy] — Shimoji K. No shinkei geka. Neurological surgery 2022. PubMed
- Third ventriculostomy — Siomin V. Journal of neurosurgery 2003. PubMed
- Third ventriculostomy in shunt malfunction — Spennato P. World neurosurgery 2013. PubMed
- Endoscopic Third Ventriculostomy: Success and Failure — Deopujari CE. Journal of Korean Neurosurgical Society 2017. PubMed
- Endoscopic third ventriculostomy for shunt malfunction in children: A review — Waqar M. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia 2018. PubMed
- Endoscopic third ventriculostomy — Jallo GI. Neurosurgical focus 2005. PubMed
- Endoscopic Third Ventriculostomy And Choroid Plexus Coagulation in Infants: Current Concepts and Illustrative Cases — Baticulon RE. Neurology India 2021. PubMed
- Third ventriculostomy: a review — Grant JA. Surgical neurology 1997. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
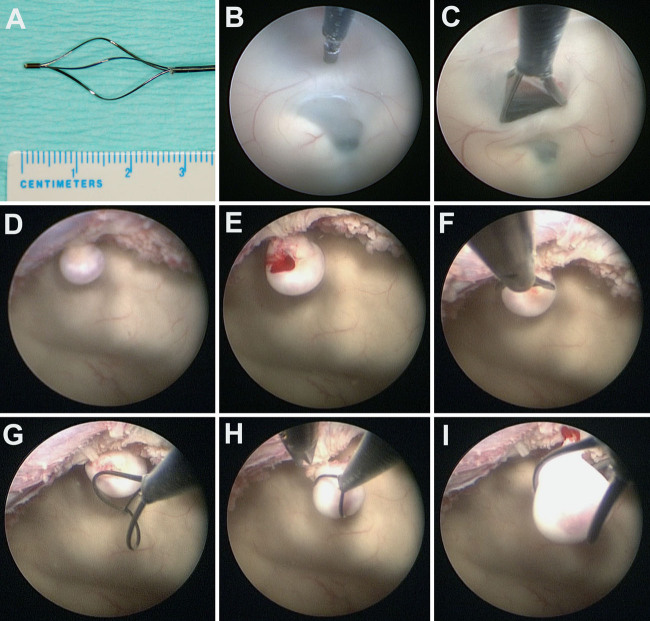 FIG. 2.. NSB-assisted ETV and removal of the intraventricular tumor. A: Expanded tip of the NSB. B: The floor of the third ventricle was penetrated with the blunt tip of the NSB. C: The stoma of… Source: Pure ventriculoscopic resection of an intraventricular meningioma with a basket retriever through a single burr hole: illustrative case — Journal of Neurosurgery: Case Lessons 2026; CC BY-NC-ND.
FIG. 2.. NSB-assisted ETV and removal of the intraventricular tumor. A: Expanded tip of the NSB. B: The floor of the third ventricle was penetrated with the blunt tip of the NSB. C: The stoma of… Source: Pure ventriculoscopic resection of an intraventricular meningioma with a basket retriever through a single burr hole: illustrative case — Journal of Neurosurgery: Case Lessons 2026; CC BY-NC-ND.
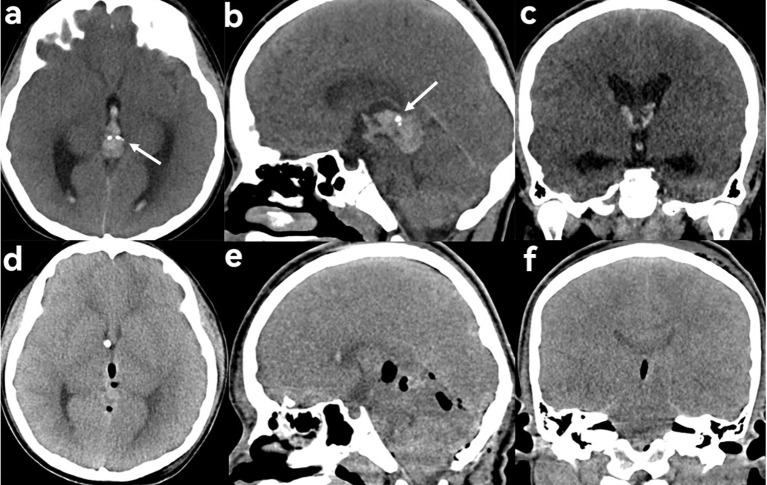 Figure 1. Choriocarcinoma of the pineal body in a 9-year-old male patient presenting with dizziness and headache. (a–c) Preoperative CT showed a patchy hyperdense, slightly inhomogeneous lesion in… Source: Case Report: Primary choriocarcinoma of the pineal region — Frontiers in Oncology 2026; CC BY.
Figure 1. Choriocarcinoma of the pineal body in a 9-year-old male patient presenting with dizziness and headache. (a–c) Preoperative CT showed a patchy hyperdense, slightly inhomogeneous lesion in… Source: Case Report: Primary choriocarcinoma of the pineal region — Frontiers in Oncology 2026; CC BY.
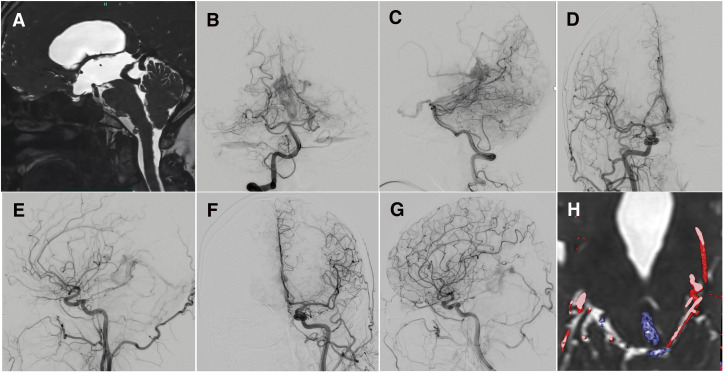 Fig. 1. Heavily T2-weighted CISS MRI demonstrates obstruction of the cerebral aqueduct caused by a dilated draining vein (A). Right VA angiography shows a falcotentorial dAVF supplied by… Source: Falcotentorial dAVF with Unusual Venous Drainage Presenting with Obstructive Hydrocephalus: A Case Report and Literature Review of Endoscopic Third Ventriculostomy Followed by Staged Transarterial Embolization — JNET Journal of Neuroendovascular Therapy 2026; CC BY-NC.
Fig. 1. Heavily T2-weighted CISS MRI demonstrates obstruction of the cerebral aqueduct caused by a dilated draining vein (A). Right VA angiography shows a falcotentorial dAVF supplied by… Source: Falcotentorial dAVF with Unusual Venous Drainage Presenting with Obstructive Hydrocephalus: A Case Report and Literature Review of Endoscopic Third Ventriculostomy Followed by Staged Transarterial Embolization — JNET Journal of Neuroendovascular Therapy 2026; CC BY-NC.
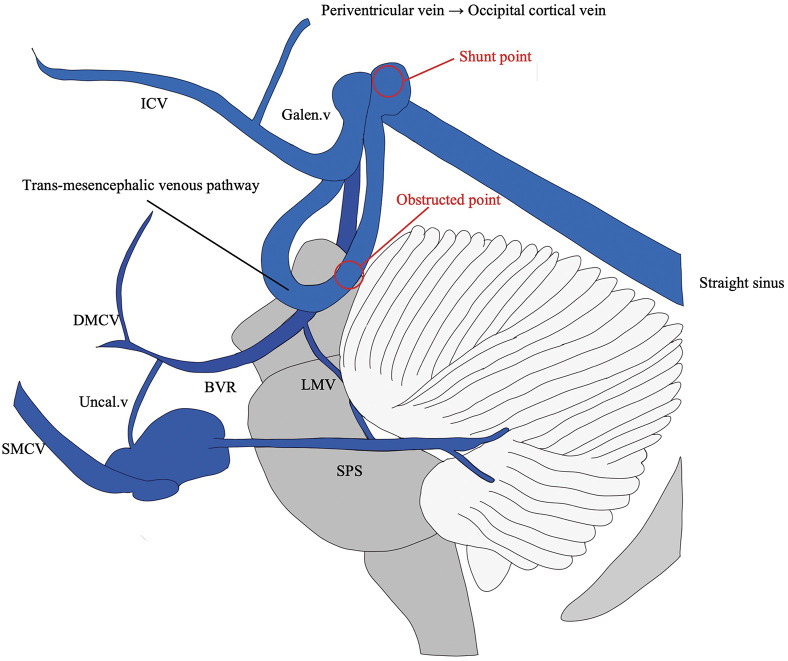 Fig. 2. A schematic illustration depicts the venous anatomy of the falcotentorial dAVF. In association with an occluded straight sinus, the draining vein from the shunt point initially descends… Source: Falcotentorial dAVF with Unusual Venous Drainage Presenting with Obstructive Hydrocephalus: A Case Report and Literature Review of Endoscopic Third Ventriculostomy Followed by Staged Transarterial Embolization — JNET Journal of Neuroendovascular Therapy 2026; CC BY-NC.
Fig. 2. A schematic illustration depicts the venous anatomy of the falcotentorial dAVF. In association with an occluded straight sinus, the draining vein from the shunt point initially descends… Source: Falcotentorial dAVF with Unusual Venous Drainage Presenting with Obstructive Hydrocephalus: A Case Report and Literature Review of Endoscopic Third Ventriculostomy Followed by Staged Transarterial Embolization — JNET Journal of Neuroendovascular Therapy 2026; CC BY-NC.
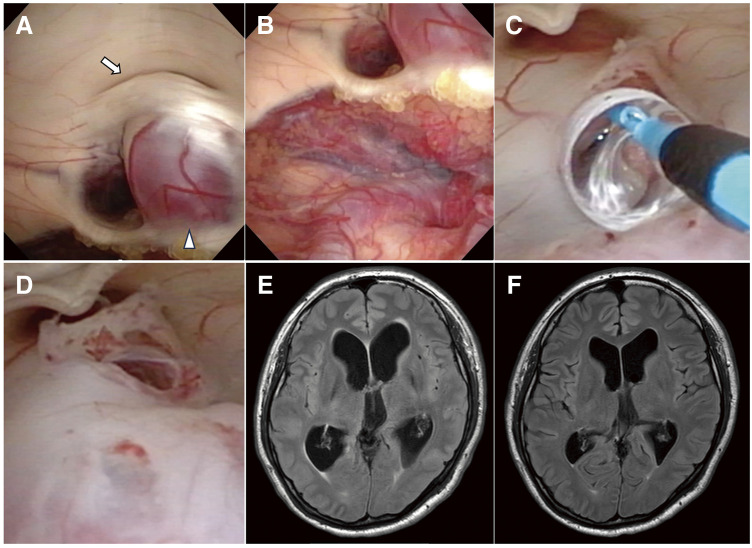 Fig. 3. Endoscopic views obtained during ETV demonstrate an obstructed cerebral aqueduct (arrow) compressed by a dilated trans-mesencephalic venous pathway (arrowhead) (A). An additional… Source: Falcotentorial dAVF with Unusual Venous Drainage Presenting with Obstructive Hydrocephalus: A Case Report and Literature Review of Endoscopic Third Ventriculostomy Followed by Staged Transarterial Embolization — JNET Journal of Neuroendovascular Therapy 2026; CC BY-NC.
Fig. 3. Endoscopic views obtained during ETV demonstrate an obstructed cerebral aqueduct (arrow) compressed by a dilated trans-mesencephalic venous pathway (arrowhead) (A). An additional… Source: Falcotentorial dAVF with Unusual Venous Drainage Presenting with Obstructive Hydrocephalus: A Case Report and Literature Review of Endoscopic Third Ventriculostomy Followed by Staged Transarterial Embolization — JNET Journal of Neuroendovascular Therapy 2026; CC BY-NC.
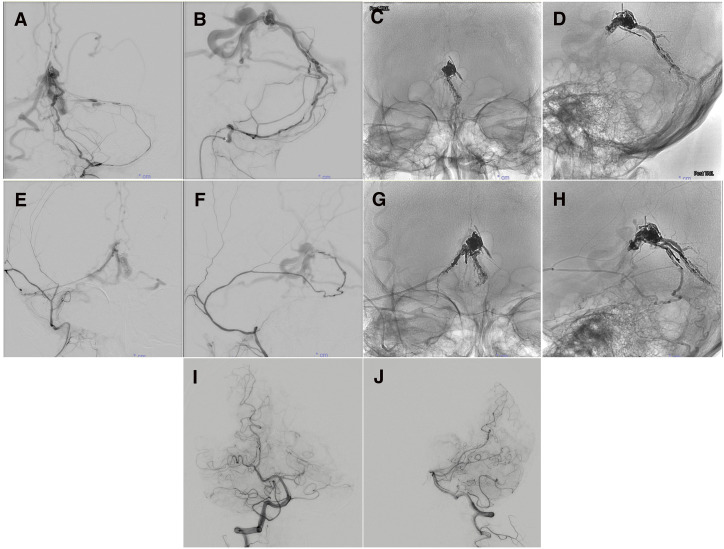 Fig. 4. Preoperative left APA angiography shows arterial supply to the shunt point via the hypoglossal branch (A, B). Left APA angiography after TAE with Onyx via the hypoglossal branch shows… Source: Falcotentorial dAVF with Unusual Venous Drainage Presenting with Obstructive Hydrocephalus: A Case Report and Literature Review of Endoscopic Third Ventriculostomy Followed by Staged Transarterial Embolization — JNET Journal of Neuroendovascular Therapy 2026; CC BY-NC.
Fig. 4. Preoperative left APA angiography shows arterial supply to the shunt point via the hypoglossal branch (A, B). Left APA angiography after TAE with Onyx via the hypoglossal branch shows… Source: Falcotentorial dAVF with Unusual Venous Drainage Presenting with Obstructive Hydrocephalus: A Case Report and Literature Review of Endoscopic Third Ventriculostomy Followed by Staged Transarterial Embolization — JNET Journal of Neuroendovascular Therapy 2026; CC BY-NC.
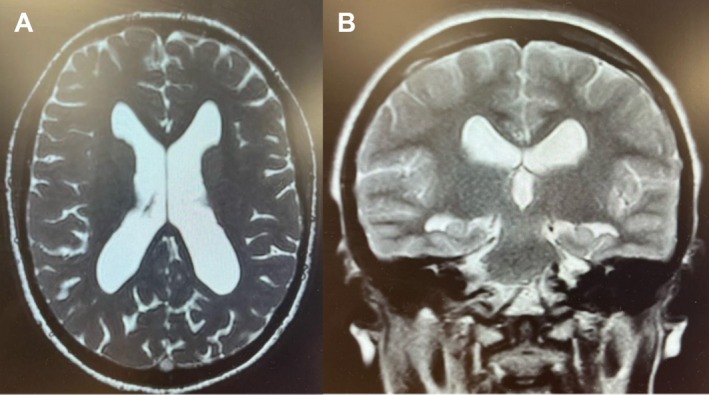 FIGURE 3. Postoperative axial (A) and coronal (B) MRI slices demonstrating reduced ventricular size following endoscopic third ventriculostomy. Source: A Case of Noncommunicating Hydrocephalus Presenting as Isolated Hyposmia — Clinical Case Reports 2026; CC BY.
FIGURE 3. Postoperative axial (A) and coronal (B) MRI slices demonstrating reduced ventricular size following endoscopic third ventriculostomy. Source: A Case of Noncommunicating Hydrocephalus Presenting as Isolated Hyposmia — Clinical Case Reports 2026; CC BY.
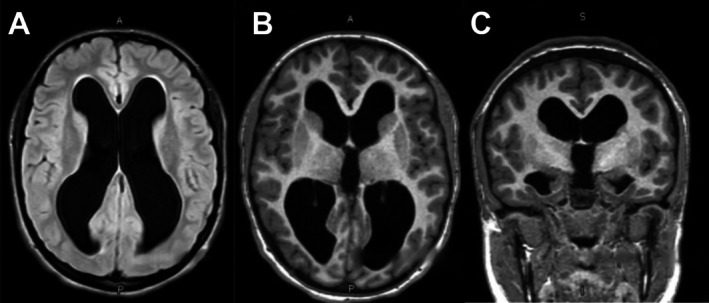 FIGURE 2. Preoperative axial (A and B) and coronal (C) MRI slices showing symmetrical dilation of the lateral and third ventricles with associated parenchymal thinning, consistent with… Source: A Case of Noncommunicating Hydrocephalus Presenting as Isolated Hyposmia — Clinical Case Reports 2026; CC BY.
FIGURE 2. Preoperative axial (A and B) and coronal (C) MRI slices showing symmetrical dilation of the lateral and third ventricles with associated parenchymal thinning, consistent with… Source: A Case of Noncommunicating Hydrocephalus Presenting as Isolated Hyposmia — Clinical Case Reports 2026; CC BY.
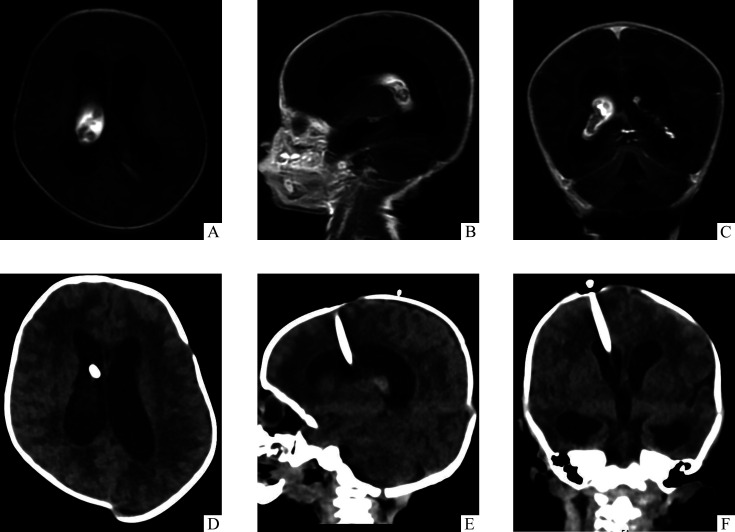 图1. 儿童复杂性脑积水女婴(22 d)的头颅影像学表现Figure 1 Cranial imaging findings in a 22-day-old female infant with complex hydrocephalusA-C: Preoperative MRI of axial (A), sagittal (B), and coronal planes (C)… Source: 儿童复杂性脑积水的诊治新策略:阶段性手术管理流程 — Journal of Central South University Medical Sciences 2026; CC BY-NC-ND.
图1. 儿童复杂性脑积水女婴(22 d)的头颅影像学表现Figure 1 Cranial imaging findings in a 22-day-old female infant with complex hydrocephalusA-C: Preoperative MRI of axial (A), sagittal (B), and coronal planes (C)… Source: 儿童复杂性脑积水的诊治新策略:阶段性手术管理流程 — Journal of Central South University Medical Sciences 2026; CC BY-NC-ND.
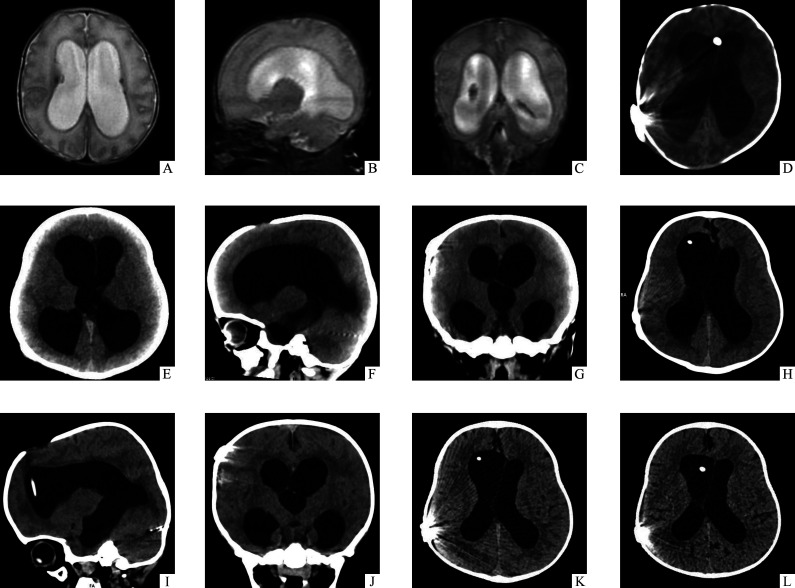 图2. 儿童复杂性脑积水男婴(1月龄)的头颅影像学表现Figure 2 Cranial imaging findings in a 1-month-old male infant with complex hydrocephalusA-C: Preoperative MRI in the axial (A), sagittal (B), and coronal (C)… Source: 儿童复杂性脑积水的诊治新策略:阶段性手术管理流程 — Journal of Central South University Medical Sciences 2026; CC BY-NC-ND.
图2. 儿童复杂性脑积水男婴(1月龄)的头颅影像学表现Figure 2 Cranial imaging findings in a 1-month-old male infant with complex hydrocephalusA-C: Preoperative MRI in the axial (A), sagittal (B), and coronal (C)… Source: 儿童复杂性脑积水的诊治新策略:阶段性手术管理流程 — Journal of Central South University Medical Sciences 2026; CC BY-NC-ND.
History of Present Illness
- Chief complaint: Headache, nausea, gait/cognitive decline, papilledema; (infants: macrocephaly, sunsetting)
- Obstructive hydrocephalus — ETV bypasses obstruction (NOT for communicating hydrocephalus typically)
- ETV Success Score (age, etiology, prior shunt) — predicts success
- Etiology: aqueductal stenosis, tectal glioma, pineal/posterior fossa tumor
Imaging Review
MRI (T1, T2, high-resolution sagittal/CISS, cine CSF flow)
- Triventricular hydrocephalus (dilated lateral + 3rd, normal 4th) = obstructive pattern
- Third ventricle floor: thinned, bowed down; adequate space (prepontine cistern) between floor and basilar/clivus
- Basilar artery and perforators position below the floor
- Obstruction site (aqueduct, tumor)
- Anatomy: massa intermedia, mammillary bodies, infundibular recess, tuber cinereum
Labs
- CBC, BMP, Coags
Neurological Examination
- Mental status, papilledema, gait, eye movements (Parinaud if tectal)
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: navigation or endoscope as indicated, shunt hardware/valve setting verified, distal-access tools or general surgery help when needed, antibiotic-impregnated catheter availability, and postop imaging plan.
- Special needs: antibiotic timing, programmable valve documentation, abdominal/chest/vascular distal-site plan, CSF culture plan for revision/infection, anticoagulation plan, and EVD backup if access fails.
- Immediate postop orders: neuro checks, CT or shunt-series timing, valve setting documentation and MRI precautions, wound/abdominal/distal-site checks, infection watch, DVT timing, and follow-up for setting adjustment.
Diagnosis & Indication
- Indication: Obstructive hydrocephalus; avoids shunt dependence
- Contraindications/cautions: communicating hydrocephalus, distorted anatomy, very young infants (lower success), narrow prepontine cistern
Position
- Supine, head neutral, slightly flexed; navigation optional
- Right frontal entry (Kocher’s point, slightly more anterior/midline-adjusted for trajectory to foramen of Monro)
Key Surgical Steps
- Right frontal burr hole at modified Kocher’s point (trajectory aimed at foramen of Monro)
- Introduce peel-away sheath/endoscope into right frontal horn
- Navigate to foramen of Monro — identify landmarks (choroid plexus, septal vein, thalamostriate vein, fornix)
- Pass through foramen of Monro into the third ventricle
- Identify third ventricle floor landmarks: mammillary bodies (posterior), infundibular recess (anterior), tuber cinereum (between)
- Fenestrate the floor at the midline in front of the mammillary bodies, behind the dorsum sellae/infundibular recess — through the tuber cinereum
- Blunt perforation (not cautery near basilar), then dilate with Fogarty balloon
- Inspect below floor — open membrane of Liliequist; confirm patency into prepontine/interpeduncular cistern; visualize and avoid the basilar artery
- Confirm flow (floor pulsation), hemostasis
- [± Endoscopic biopsy of tumor in same session]
- Withdraw endoscope, closure (± Gelfoam in tract)
Critical Anatomy & Structures at Risk
- Basilar artery and its perforators (P1, thalamoperforators) — directly below floor; injury catastrophic (fatal hemorrhage, infarct)
- Fornix (at foramen of Monro) — memory
- Hypothalamus (floor, tuber cinereum) — endocrine/autonomic
- CN III (interpeduncular cistern)
Equipment
- Rigid neuroendoscope + working channel, peel-away sheath
- Fogarty/ETV balloon catheter, blunt fenestration probe
- Navigation (optional), irrigation (warm LR), biopsy forceps (if tumor)
- EVD kit (backup)
Monitoring
- Standard; watch for bradycardia (floor manipulation — vagal/hypothalamic)
Anesthesia
- General; warm irrigation (avoid hypothermia); watch bradycardia/asystole during floor manipulation (stop, irrigate)
Potential Complications
- Basilar artery injury — rare, catastrophic
- Bradycardia/cardiac arrest (floor manipulation), hypothalamic injury (memory, endocrine, autonomic)
- Fornix injury (memory), CN III palsy
- ETV failure (stoma closure) → may need shunt; delayed failure possible
- CSF leak, hemorrhage (intraventricular), infection
Operative Note Template
Preoperative Diagnosis: Obstructive (non-communicating) hydrocephalus due to [aqueductal stenosis / tectal or pineal tumor]
Postoperative Diagnosis: Same
Procedure: Endoscopic third ventriculostomy [with endoscopic tumor biopsy]
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Minimal Adjuncts: Rigid neuroendoscope + working channel, Fogarty/ETV balloon, [navigation], warm irrigation, [biopsy forceps] Complications: None Note: Watch for bradycardia during floor manipulation
Indications: [Age]yo [M/F] with obstructive hydrocephalus ([etiology]) and a favorable third-ventricle floor anatomy on MRI. ETV was chosen to avoid shunt dependence. Risks (basilar injury, bradycardia, ETV failure) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced. A right frontal burr hole was made at a modified Kocher’s point along a trajectory to the foramen of Monro, and the endoscope introduced via a peel-away sheath into the right frontal horn. The foramen of Monro was identified (choroid plexus, septal/thalamostriate veins, fornix) and the third ventricle entered. The floor landmarks were identified — mammillary bodies posteriorly, infundibular recess anteriorly, tuber cinereum between.
The floor was bluntly fenestrated in the midline anterior to the mammillary bodies (not with cautery near the basilar), then dilated with a Fogarty balloon. The membrane of Liliequist was opened and patency into the prepontine cistern confirmed, with the basilar artery visualized and avoided. Floor pulsation confirmed flow. [An endoscopic tumor biopsy was obtained.] Hemostasis was confirmed and the endoscope withdrawn.
The patient was transferred to the [floor/ICU]; postoperative imaging confirmed stoma patency.
Postoperative Plan
- Floor/step-down (ICU if tumor/complex), neuro checks q1-2h
- CT/MRI postop (cine flow shows stoma patency; ventricles may not shrink immediately)
- Monitor for ETV failure (recurrent hydrocephalus symptoms — can be early or delayed → shunt)
- If biopsy: pathology, tumor board
- Follow-up MRI; counsel on signs of failure
Chief-Level Case Review
Use these as the senior-level mental model for Endoscopic Third Ventriculostomy (ETV):
- Decision point: Trajectory and hardware choice should follow the failure mode: obstruction, infection, overdrainage, loculation, slit ventricle, distal failure, or wrong pressure setting.
- Technical lever: Document the system: entry point, catheter target/depth, valve type and setting, distal site, antibiotic-impregnated hardware, and what imaging confirms placement.
- Bailout: Rescue plan is practical: poor CSF return, bloody CSF, malposition, distal access failure, abdominal/pleural complication, or inability to safely pass the catheter.
- Postop watch: Postop orders must be unambiguous: drain height/rate/max output, valve setting, clamp parameters, imaging, antibiotics, ICP/neuro checks, and overdrainage precautions.
Common Pimp Questions
Use these to pressure-test preparation for Endoscopic Third Ventriculostomy (ETV):
- What is the working CSF physiology problem: obstruction, absorption failure, overdrainage, infection, or catheter failure?
- Where exactly is the entry point, target, and backup trajectory?
- What valve, catheter, endoscope, or navigation preference does the attending use?
- What is the infection-prevention plan and what cultures/CSF studies are needed?
- What postop imaging, valve setting, drainage level, and neuro-check plan should be written?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Valve brand/setting, antibiotic catheter use, and tunneling side: [attending-specific]
- Navigation/endoscope/stylet preference and ventricular target: [attending-specific]
- CSF culture/lab routine and perioperative antibiotic duration: [attending-specific]
- Postop scan timing, EVD height or valve verification, and activity restrictions: [attending-specific]