
Case Prep: Frame-Based Stereotactic Brain Biopsy (Leksell / CRW)
Case / Approach Snapshot
- Anatomy at risk: target margins, vascular/necrotic zones, entry cortex, sulci/vessels, ventricles, deep nuclei, and eloquent tracts along the trajectory.
- Operative steps: choose the safest diagnostic target, plan trajectory, verify registration or frame coordinates, obtain staged samples, confirm hemostasis/trajectory imaging, and coordinate pathology/molecular testing; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: nondiagnostic tissue, hemorrhage, seizure, edema, neurologic change, target shift, infection, and open biopsy or repeat sampling plan.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [deep / eloquent / multifocal] [location] brain lesion of uncertain diagnosis planned for frame-based stereotactic needle biopsy ([Leksell / CRW]) for tissue diagnosis.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Complications after frame-based stereotactic brain biopsy: a systematic review — Riche M. Neurosurgical review 2021. PubMed
- Frame-based versus frameless stereotactic brain biopsies: A systematic review and meta-analysis — Kesserwan MA. Surgical neurology international 2021. PubMed
- Comparison of Frame-Based Versus Frameless Image-Guided Intracranial Stereotactic Brain Biopsy: A Retrospective Analysis of Safety and Efficacy — Ungar L. World neurosurgery 2022. PubMed
- Blurring the boundaries between frame-based and frameless stereotaxy: feasibility study for brain biopsies performed with the use of a head-mounted robot — Grimm F. Journal of neurosurgery 2015. PubMed
- Comparison of Frame-Based Versus Frameless Intracranial Stereotactic Biopsy: Systematic Review and Meta-Analysis — Dhawan S. World neurosurgery 2019. PubMed
- Frame-Based Stereotactic Biopsy - A Single Neurosurgeon Experience of 604 Diagnostic Procedures and Literature Review — Samanci Y. Turkish neurosurgery 2022. PubMed
- Surgical technique — Guénot M. Neurophysiologie clinique = Clinical neurophysiology 2018. PubMed
- Related factors with diagnostic yield and intracranial hemorrhagic complications in frame-based stereotactic biopsy. Review — Lara-Almunia M. Neurocirugia 2021. PubMed
- Related factors with diagnostic yield and intracranial hemorrhagic complications in frame-based stereotactic biopsy. Review — Lara-Almunia M. Neurocirugia 2021. PubMed
- Comparative Analysis of Efficacy and Safety of Frame-Based, Frameless, and Robot-Assisted Stereotactic Brain Biopsies: A Systematic Review and Meta-Analysis — Gecici NN. Operative neurosurgery (Hagerstown, Md.) 2025. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
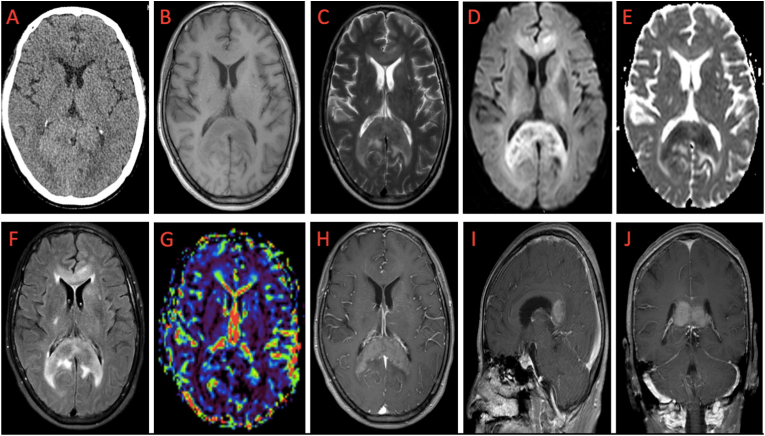 Figure 1. Multimodal imaging findings of a patient with primary CNS lymphoma in the splenium of the corpus callosum: A: slightly higher CT plain scan density; B: hypointense in T1; C: hypointense… Source: Preliminary clinical application of multimodal imaging combined with frameless robotic stereotactic biopsy in the diagnosis of primary central nervous system lymphoma — Heliyon 2022; CC BY.
Figure 1. Multimodal imaging findings of a patient with primary CNS lymphoma in the splenium of the corpus callosum: A: slightly higher CT plain scan density; B: hypointense in T1; C: hypointense… Source: Preliminary clinical application of multimodal imaging combined with frameless robotic stereotactic biopsy in the diagnosis of primary central nervous system lymphoma — Heliyon 2022; CC BY.
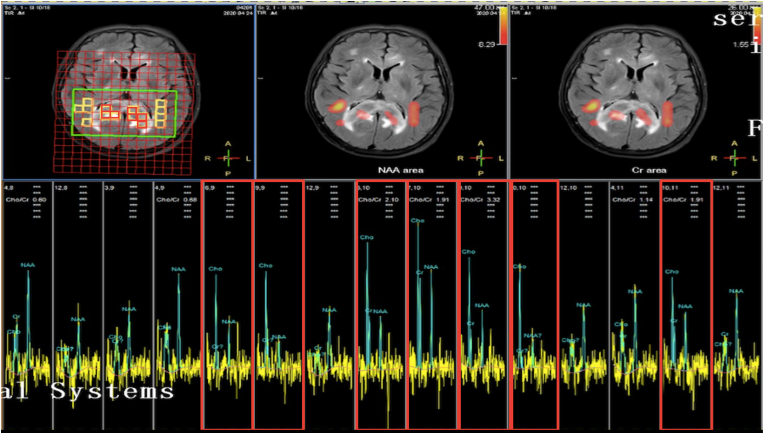 Figure 2. The spectra showed an obvious increase in CHO, a decrease in NAA, and an increase in CHO/Cr and Cho/NAA ratios in the lesion (in the red boxes) compared with the normal brain (in the… Source: Preliminary clinical application of multimodal imaging combined with frameless robotic stereotactic biopsy in the diagnosis of primary central nervous system lymphoma — Heliyon 2022; CC BY.
Figure 2. The spectra showed an obvious increase in CHO, a decrease in NAA, and an increase in CHO/Cr and Cho/NAA ratios in the lesion (in the red boxes) compared with the normal brain (in the… Source: Preliminary clinical application of multimodal imaging combined with frameless robotic stereotactic biopsy in the diagnosis of primary central nervous system lymphoma — Heliyon 2022; CC BY.
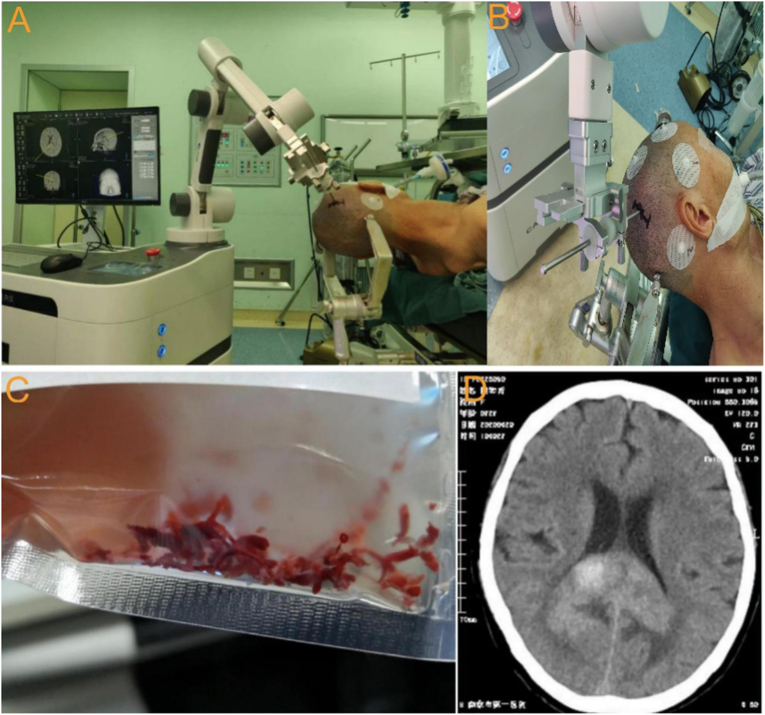 Figure 3. Procedure of frameless stereotactic robotic needle biopsy in the patient with PCNSL: A: the puncture trajectory was determined according to the puncture target; B: Four spherical… Source: Preliminary clinical application of multimodal imaging combined with frameless robotic stereotactic biopsy in the diagnosis of primary central nervous system lymphoma — Heliyon 2022; CC BY.
Figure 3. Procedure of frameless stereotactic robotic needle biopsy in the patient with PCNSL: A: the puncture trajectory was determined according to the puncture target; B: Four spherical… Source: Preliminary clinical application of multimodal imaging combined with frameless robotic stereotactic biopsy in the diagnosis of primary central nervous system lymphoma — Heliyon 2022; CC BY.
 Figure 1. All patients underwent robot-assisted stereotactic brain biopsy using one of three systems: a ROSA robotic system (Zimmer Biomet Robotics, Montpellier, France), the CAS-R-2 (Tianjin… Source: Novel application of robot-guided stereotactic technique on biopsy diagnosis of intracranial lesions — Frontiers in Neurology 2023; CC BY.
Figure 1. All patients underwent robot-assisted stereotactic brain biopsy using one of three systems: a ROSA robotic system (Zimmer Biomet Robotics, Montpellier, France), the CAS-R-2 (Tianjin… Source: Novel application of robot-guided stereotactic technique on biopsy diagnosis of intracranial lesions — Frontiers in Neurology 2023; CC BY.
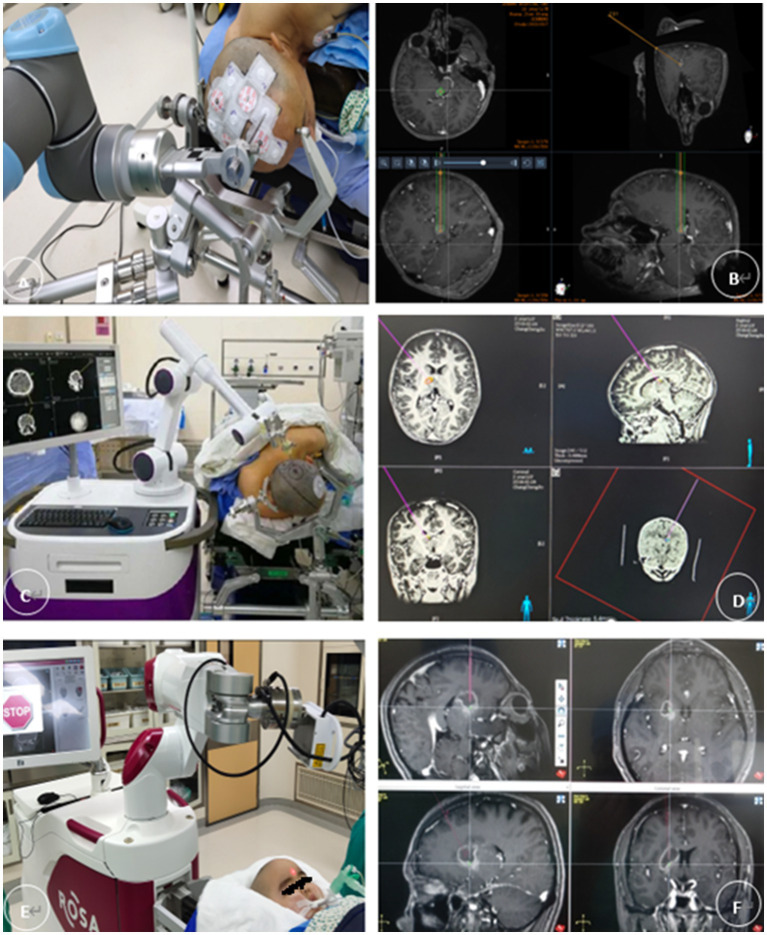 Figure 2. (A,B) The REMEBOT and (C,D) the CAS-R-2 use scalp markers for registration. The patient’s head is prepared for skin adhesion to the scalp markers before surgery (E,F). The ROSA robot… Source: Novel application of robot-guided stereotactic technique on biopsy diagnosis of intracranial lesions — Frontiers in Neurology 2023; CC BY.
Figure 2. (A,B) The REMEBOT and (C,D) the CAS-R-2 use scalp markers for registration. The patient’s head is prepared for skin adhesion to the scalp markers before surgery (E,F). The ROSA robot… Source: Novel application of robot-guided stereotactic technique on biopsy diagnosis of intracranial lesions — Frontiers in Neurology 2023; CC BY.
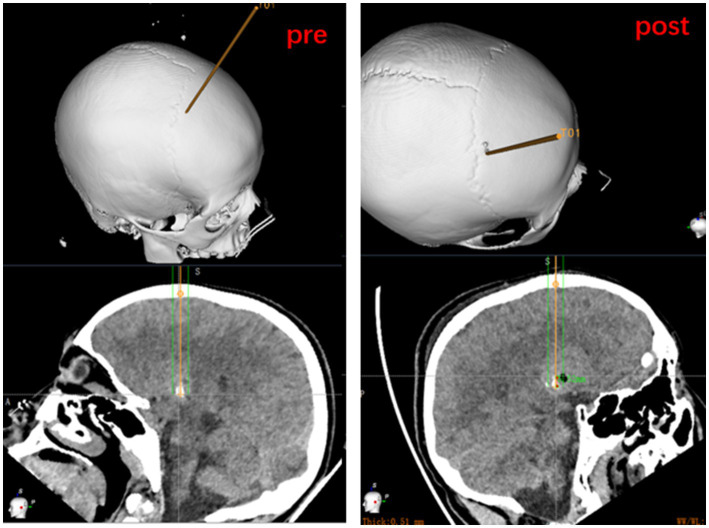 Figure 3. Measurement of entry point and target point error based on preoperatively planned target and on the fusion of postoperative CT to the preoperative dataset. Source: Novel application of robot-guided stereotactic technique on biopsy diagnosis of intracranial lesions — Frontiers in Neurology 2023; CC BY.
Figure 3. Measurement of entry point and target point error based on preoperatively planned target and on the fusion of postoperative CT to the preoperative dataset. Source: Novel application of robot-guided stereotactic technique on biopsy diagnosis of intracranial lesions — Frontiers in Neurology 2023; CC BY.
History of Present Illness
- Chief complaint: New neurological deficit / seizure / lesion(s) on imaging requiring diagnosis
- Lesion not safely resectable, or diagnosis would change management (lymphoma, infection, unresectable glioma, deep/eloquent location)
- If lymphoma suspected: avoid steroids pre-biopsy (if clinically tolerable) — steroids can make lymphoma non-diagnostic
- Immune status (toxoplasmosis vs lymphoma in HIV), prior cancer
Past Medical History
- Anticoagulant/antiplatelet (stop/correct — hemorrhage risk), bleeding disorder
- HIV/immunocompromise, prior malignancy, prior radiation
- Standard PMH
Imaging Review
MRI (T1±Gad, T2, FLAIR, DWI) ± CTA
- Lesion location, enhancing/representative target (avoid necrotic core), size
- Plan avascular trajectory (avoid sulci, vessels, ventricles, eloquent cortex)
- Multifocality (choose safest/most diagnostic target)
Stereotactic planning imaging
- Stereotactic CT or MRI with the frame applied (frame fiducials) → merge with diagnostic MRI → calculate target and entry coordinates
Labs
- CBC (Plt), Coags (INR < 1.4), BMP, type and screen
- HIV/toxoplasma serology if relevant
Neurological Examination
- Baseline focal exam; document for comparison
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: frame/robot/navigation system registered and independently checked, biopsy needle and specimen cups/media ready, frozen/smear pathology available, trajectory images displayed, and immediate CT access planned.
- Special needs: coagulopathy/antiplatelet correction, steroids held when lymphoma is suspected and clinically safe, seizure prophylaxis by lesion/location, BP control, and specimen handling for flow cytometry, cultures, and molecular testing.
- Immediate postop orders: neuro checks, CT head to exclude hemorrhage, BP parameters, dexamethasone only if clinically indicated, antiepileptic plan, pathology follow-up, and escalation plan for tract hemorrhage or nondiagnostic result.
Workflow
- Apply stereotactic frame (Leksell/CRW) under local anesthesia ± sedation (4 pins to skull) — keep frame aligned to anatomy
- Stereotactic imaging (CT, or MRI) with frame/fiducial box
- Plan on workstation: select target (enhancing tissue), entry point, trajectory avoiding vessels/sulci/ventricles; compute frame coordinates (x, y, z) and arc/ring angles
- Transfer to OR
Position
- Supine (or per target), frame fixed to the OR table adapter; HOB per trajectory; usually local + sedation (can be GA)
Key Surgical Steps
- Set the frame coordinates and arc/ring angles per plan; mount the arc
- Confirm entry point on the scalp; small incision and twist-drill burr hole at the planned entry
- Coagulate and open the dura (and pia) at entry
- Advance the biopsy needle (Sedan side-cutting cannula) along the frame-defined trajectory to target depth
- Take serial biopsies: obtain specimens at staged depths through the lesion and from multiple radial orientations (rotate the side-cutting window)
- Frozen section / smear confirmation that diagnostic tissue is present before finishing (re-sample if non-diagnostic/necrotic)
- Hemostasis: observe the cannula for bleeding; if bleeding, leave cannula, irrigate, wait; persistent → manage/re-image
- Withdraw needle, closure of the small incision
- Remove frame
Critical Anatomy & Structures at Risk
- Vessels along the trajectory (sulcal/cortical, deep) — hemorrhage is the main risk
- Ventricles (CSF egress, deviation), eloquent cortex/tracts
- Deep structures (thalamus/brainstem targets — narrow margins)
Equipment
- Stereotactic frame (Leksell/CRW) + arc + table adapter
- Planning workstation, stereotactic CT/MRI
- Twist drill, biopsy needle (Sedan side-cutting), bipolar
- Frozen section / smear pathology available intraoperatively
Anesthesia
- Local + sedation (awake — allows neuro monitoring) or GA; BP control (hemorrhage); cefazolin
Potential Complications
- Hemorrhage (~1-3% symptomatic — into tract/lesion) — deficit, rarely catastrophic
- Non-diagnostic sample (necrosis/sampling error) — frozen confirmation reduces; may need repeat
- Seizure, infection, neurological deficit (eloquent trajectory), transient worsening
Operative Note Template
Preoperative Diagnosis: [Location] brain lesion of uncertain diagnosis ([deep/eloquent/multifocal])
Postoperative Diagnosis: Same (pending pathology)
Procedure: Frame-based ([Leksell/CRW]) stereotactic biopsy of [location] lesion
Surgeon / Assistant: Anesthesia: [Local + sedation / general] EBL / Fluids: Minimal Adjuncts: Stereotactic frame + arc, planning workstation, stereotactic CT/MRI, Sedan side-cutting needle; intraoperative frozen section Specimens: Brain lesion (multiple cores) for permanent ± flow cytometry/microbiology Complications: None
Indications: [Age]yo [M/F] with a [deep/eloquent] [location] lesion where resection is not indicated and tissue diagnosis will guide management. [Steroids were withheld given lymphoma suspicion.] Coagulopathy corrected. Risks (hemorrhage, non-diagnostic sample) discussed.
Description of Procedure: After consent and time-out, the stereotactic frame was applied under local anesthesia, a stereotactic CT obtained and merged with the planning MRI, and the target (enhancing tissue), entry, and an avascular trajectory computed. In the OR, the arc was set to the calculated coordinates and a small incision and twist-drill burr hole made at the entry; the dura/pia were coagulated and opened.
The Sedan side-cutting biopsy needle was advanced along the frame-defined trajectory to the target, and serial specimens taken at staged depths and radial orientations. Frozen section confirmed diagnostic tissue. The tract was observed for bleeding and hemostasis confirmed, the needle withdrawn, the incision closed, and the frame removed.
A postoperative CT was obtained to exclude hemorrhage. The patient was transferred to the floor.
Postoperative Plan
- Postop CT head (rule out hemorrhage) — routine
- Floor/observation, neuro checks q1-2h initially
- Resume meds per bleeding risk; hold steroids if lymphoma pending (per team)
- Pathology (permanent + molecular — IDH, etc.; flow cytometry if lymphoma; cultures if infection)
- Tumor board / management per diagnosis; follow-up
Chief-Level Case Review
Use these as the senior-level mental model for Frame-Based Stereotactic Brain Biopsy (Leksell / CRW):
- Decision point: The target must answer the question: choose tissue/trajectory/dose based on diagnostic yield, molecular testing, treatment impact, and safest corridor.
- Technical lever: Risk lives along the path: vessels, sulci, ventricles, necrotic center, eloquent tracts, prior radiation, and anticoagulation decide whether the plan is acceptable.
- Bailout: Confirm before committing: frame/robot registration, coordinates, fiducials, trajectory collision, specimen adequacy, and postop scan threshold should be explicit.
- Postop watch: Postop plan should anticipate the rare catastrophe: hemorrhage, edema, seizure, steroid need, neurologic checks, pathology handoff, and treatment-board timing.
Common Pimp Questions
Use these to pressure-test preparation for Frame-Based Stereotactic Brain Biopsy (Leksell / CRW):
- What target coordinate, trajectory, and no-fly-zone were chosen?
- What imaging confirms target accuracy and avoids vessel/ventricle/sulcus violation?
- What specimen, pathology, culture, or molecular study must be obtained?
- What hemorrhage, edema, seizure, or thermal-injury sign must be watched for tonight?
- What postop scan timing and steroid/antiepileptic plan is appropriate?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Frame versus frameless/robot platform and planning software: [attending-specific]
- Trajectory constraints, number of cores/targets, and frozen/permanent pathology plan: [attending-specific]
- Steroid/antiepileptic prophylaxis and postop scan timing: [attending-specific]
- Admit versus discharge threshold and neuro-check frequency: [attending-specific]