
Case Prep: Robot-Assisted Stereotactic Brain Biopsy (ROSA / Mazor / Neuromate)
Case / Approach Snapshot
- Anatomy at risk: target margins, vascular/necrotic zones, entry cortex, sulci/vessels, ventricles, deep nuclei, and eloquent tracts along the trajectory.
- Operative steps: choose the safest diagnostic target, plan trajectory, verify registration or frame coordinates, obtain staged samples, confirm hemostasis/trajectory imaging, and coordinate pathology/molecular testing; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: nondiagnostic tissue, hemorrhage, seizure, edema, neurologic change, target shift, infection, and open biopsy or repeat sampling plan.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [single/multiple] [deep/eloquent] brain lesion(s) of uncertain diagnosis planned for robot-assisted stereotactic needle biopsy ([ROSA / Mazor / Neuromate]).
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Frameless robotic stereotactic brain biopsy workflow with CT-MRI fusion and CT-to-fluoroscopy registration: Step-by-step technical note and early experience — Taravilla-Loma M. Brain & spine 2026. PubMed
- Robot-assisted stereotactic brain biopsy: A systematic review and meta-analysis — Porto Junior S. Neurosurgical review 2024. PubMed
- Robot-assisted stereotactic brain biopsy: systematic review and bibliometric analysis — Marcus HJ. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2018. PubMed
- Robot-assisted versus manually guided stereotactic biopsy for intracranial lesions - a systematic review and meta-analysis — Gomes FC. Neurosurgical review 2024. PubMed
- Frameless Robotic-Assisted Biopsy of Pediatric Brainstem Lesions: A Systematic Review and Meta-Analysis of Efficacy and Safety — Lu VM. World neurosurgery 2023. PubMed
- Comparative Analysis of Efficacy and Safety of Frame-Based, Frameless, and Robot-Assisted Stereotactic Brain Biopsies: A Systematic Review and Meta-Analysis — Gecici NN. Operative neurosurgery (Hagerstown, Md.) 2025. PubMed
- The Feasibility of Robot-assisted Laser Interstitial Thermal Therapy (LITT) for Brain Tumors in Octogenarians — Lu VM. World neurosurgery 2024. PubMed
- Robotic-assisted foot and ankle surgery: a review of the present status and the future — Yoon YK. Biomedical engineering letters 2023. PubMed
- Stereoelectroencephalography: Indication and Efficacy — Iida K. Neurologia medico-chirurgica 2017. PubMed
- How I do it: sequential robot-assisted stereotactic biopsy and laser interstitial thermal therapy for epilepsy associated with brain tumors — Aboubakr O. Acta neurochirurgica 2025. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
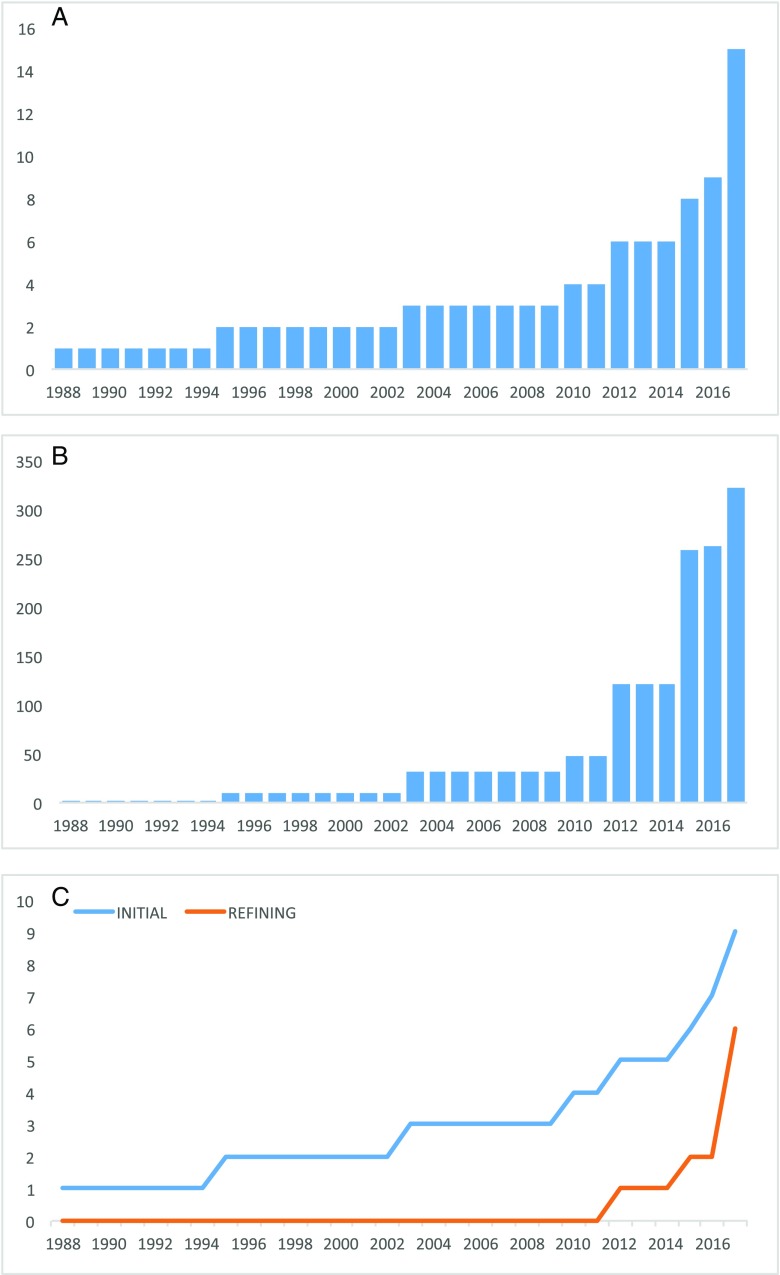 Fig. 2. Graphs demonstrating a the number of overall publications per annum, b the number of patients reported undergoing robot-assisted biopsy per annum, and c the number of initial and… Source: Robot-assisted stereotactic brain biopsy: systematic review and bibliometric analysis — Child’s Nervous System 2018; CC BY.
Fig. 2. Graphs demonstrating a the number of overall publications per annum, b the number of patients reported undergoing robot-assisted biopsy per annum, and c the number of initial and… Source: Robot-assisted stereotactic brain biopsy: systematic review and bibliometric analysis — Child’s Nervous System 2018; CC BY.
 Figure 10. Source: Robot-assisted frameless brain biopsy with computed tomography-to-fluoroscopy registration: Step-by-step surgical video — Surg Neurol Int. 2026 May 15;17:284. doi: 10.25259/SNI_158_2026; CC BY-NC-SA.
Figure 10. Source: Robot-assisted frameless brain biopsy with computed tomography-to-fluoroscopy registration: Step-by-step surgical video — Surg Neurol Int. 2026 May 15;17:284. doi: 10.25259/SNI_158_2026; CC BY-NC-SA.
History of Present Illness
- Chief complaint: Lesion(s) requiring tissue diagnosis, not safely resectable
- Robotic platform chosen for accuracy, efficiency, and especially multiple targets/trajectories (also used for SEEG, laser ablation)
- Same diagnostic considerations (lymphoma — avoid pre-biopsy steroids if feasible; infection; unresectable glioma; deep/eloquent)
Past Medical History
- Anticoagulant/antiplatelet (stop/correct), bleeding disorder, immunocompromise, prior malignancy
- Standard PMH
Imaging Review
MRI (thin-cut navigation protocol, T1±Gad, T2, FLAIR) + vascular imaging (CTA/MRA or gad MRI)
- Target(s) (enhancing/representative), avascular trajectories (robot executes exactly what is planned — vascular planning is critical)
- Plan each trajectory (entry, target, angle) on the robotic planning software
- Registration plan: frame, frameless/surface, skull fiducials, or intraoperative CT (O-arm) registration
Robotic Planning Checks
- Confirm the MRI sequence used for targeting is geometrically reliable and fused to CT without scalp/brain mismatch; inspect fusion at skull, ventricles, falx, and lesion margins.
- Choose an entry that avoids sulci, cortical vessels, venous lakes, ventricle, deep perforator territory, and eloquent cortex/tracts.
- Make the skull entry as close to perpendicular as feasible so the drill/bolt does not skid; very oblique skull entry undermines robotic precision.
- Confirm robot-arm clearance before prepping: microscope, C-arm/O-arm, anesthesia circuit, Mayfield pins, drapes, and surgeon access can all collide with the planned trajectory.
- For multiple trajectories, order them by risk and diagnostic priority; sample the most important target before swelling or hemorrhage can abort the case.
- Build a specimen plan with pathology before incision: frozen/smear, permanent, flow cytometry, culture, methylation/NGS, and which samples stay fresh.
Labs
- CBC (Plt), Coags, BMP, type and screen
Neurological Examination
- Baseline focal exam
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: frame/robot/navigation system registered and independently checked, biopsy needle and specimen cups/media ready, frozen/smear pathology available, trajectory images displayed, and immediate CT access planned.
- Special needs: coagulopathy/antiplatelet correction, steroids held when lymphoma is suspected and clinically safe, seizure prophylaxis by lesion/location, BP control, and specimen handling for flow cytometry, cultures, and molecular testing.
- Immediate postop orders: neuro checks, CT head to exclude hemorrhage, BP parameters, dexamethasone only if clinically indicated, antiepileptic plan, pathology follow-up, and escalation plan for tract hemorrhage or nondiagnostic result.
Position
- Supine/per target; head fixed (Mayfield or robot-specific clamp) and rigidly coupled to the robot reference; register and verify accuracy before drilling
Key Surgical Steps
- Plan trajectory(ies) on robotic workstation (entry, target, avascular path)
- Register patient to the robot (frame/fiducials/surface/intraop CT), confirm accuracy (sub-mm goal)
- Robot arm automatically aligns to the planned trajectory and locks (rigid guide tube)
- For each target: stab incision, twist-drill through skull along the robot-defined trajectory, coagulate/open dura
- Pass the biopsy needle through the robotic guide to the planned depth
- Serial biopsies at staged depths/orientations (side-cutting needle)
- Frozen section/smear confirmation of diagnostic tissue
- Hemostasis (observe tract); repeat for additional targets (efficient — robot repositions)
- Closure; postop/intraoperative CT to confirm and exclude hemorrhage
Registration and Accuracy Pitfalls
- Recheck accuracy after draping and after any table/head/robot movement. A perfect plan becomes unsafe if the reference array moves.
- Do not accept a registration that is “close enough” for a deep nucleus, brainstem, pineal, or small enhancing rim target; the error budget is smaller than the lesion.
- Verify the actual instrument length, stopper depth, guide-tube offset, and needle side-window orientation against the planned target depth.
- If using skull fiducials, confirm each fiducial is rigid; a loose fiducial poisons the whole registration.
- If intraoperative CT/O-arm is used, check that the reference frame is visible and rigid throughout acquisition and biopsy.
Sampling Strategy
- Take diagnostic tissue from enhancing/solid/restricting margins first; avoid necrotic center as the first pass.
- Rotate the side-cutting window deliberately and record orientation/depth if the specimen is scant.
- If frozen is nondiagnostic, use the same safe trajectory to sample adjacent viable target before planning a second trajectory.
- For suspected lymphoma, minimize steroid exposure when clinically safe and prioritize fresh tissue for flow cytometry/molecular diagnosis.
- For infection, send culture before placing all tissue in formalin.
Critical Anatomy & Structures at Risk
- Trajectory vessels — hemorrhage (robot executes the plan precisely, so vascular planning is paramount)
- Registration error (verify), eloquent structures, ventricles
- Deep targets — robot rigidity is advantageous
Equipment
- Robotic stereotactic platform (ROSA / Mazor / Neuromate / Cirq) + planning software
- Registration tools (fiducials / O-arm / surface), Mayfield/robot clamp
- Twist drill, biopsy needle (Sedan side-cutting), bipolar
- Intraoperative/postop CT, frozen-section pathology
Anesthesia
- GA (common); BP control; cefazolin
Potential Complications
- Hemorrhage (~1-3%), non-diagnostic sample
- Registration/coupling error → off-target (verify accuracy), seizure, infection, deficit
- Technical/robot setup issues
Rescue Plans
- Bloody return: keep the cannula/needle in place briefly for tamponade, stop sampling, control BP/coagulation, obtain immediate CT if persistent or symptomatic, and keep the patient intubated for imaging/ICU if needed.
- Registration concern after incision: stop; repeat registration or convert to frame/frameless navigation rather than chasing an uncertain trajectory.
- Robot collision or unreachable angle: replan trajectory before drilling; do not bend the workflow around an unsafe arm position.
- Nondiagnostic frozen: sample planned adjacent target/depth if safe, then decide between second trajectory, open biopsy, or staged repeat after imaging.
- Seizure/edema: abort further passes, treat medically, image, and hand off with steroid/antiepileptic plan tailored to the suspected diagnosis.
Operative Note Template
Preoperative Diagnosis: [Single/multiple] brain lesion(s) of uncertain diagnosis ([deep/eloquent])
Postoperative Diagnosis: Same (pending pathology)
Procedure: Robot-assisted ([ROSA/Mazor]) stereotactic biopsy of [location] lesion(s)
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Minimal Adjuncts: Robotic platform + planning software, registration (fiducials/surface/O-arm), Sedan side-cutting needle, intraoperative/postop CT; frozen section Specimens: Brain lesion (multiple cores per target) Complications: None
Indications: [Age]yo [M/F] with [a deep/eloquent / multiple] lesion(s) requiring tissue diagnosis; the robotic platform was chosen for accuracy/efficiency [and multiple trajectories]. [Steroids withheld if lymphoma suspected.] Coagulopathy corrected. Risks (hemorrhage, non-diagnostic) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced, the head fixed, and the patient registered to the robot with accuracy verified. For each target, the robot arm aligned to the pre-planned avascular trajectory and locked; a stab incision and twist-drill were made, the dura opened, and the Sedan side-cutting needle passed through the robotic guide to the target, taking serial specimens at staged depths. Frozen section confirmed diagnostic tissue. [Additional targets were sampled with robot repositioning.] Tracts were observed and hemostasis confirmed.
The incision(s) were closed and a CT obtained to confirm positions and exclude hemorrhage. The patient was transferred to the floor.
Postoperative Plan
- Postop CT head (hemorrhage)
- Floor/observation, neuro checks
- Pathology (permanent/molecular; flow cytometry if lymphoma; cultures if infection)
- Hold steroids if lymphoma pending; resume meds per bleeding risk
- Tumor board/management; follow-up
Chief-Level Case Review
Use these as the senior-level mental model for Robot-Assisted Stereotactic Brain Biopsy (ROSA / Mazor / Neuromate):
- Decision point: The target must answer the question: choose tissue/trajectory/dose based on diagnostic yield, molecular testing, treatment impact, and safest corridor.
- Technical lever: Risk lives along the path: vessels, sulci, ventricles, necrotic center, eloquent tracts, prior radiation, and anticoagulation decide whether the plan is acceptable.
- Bailout: Confirm before committing: frame/robot registration, coordinates, fiducials, trajectory collision, specimen adequacy, and postop scan threshold should be explicit.
- Postop watch: Postop plan should anticipate the rare catastrophe: hemorrhage, edema, seizure, steroid need, neurologic checks, pathology handoff, and treatment-board timing.
Common Pimp Questions
Use these to pressure-test preparation for Robot-Assisted Stereotactic Brain Biopsy (ROSA / Mazor / Neuromate):
- What target coordinate, trajectory, and no-fly-zone were chosen?
- What imaging confirms target accuracy and avoids vessel/ventricle/sulcus violation?
- What specimen, pathology, culture, or molecular study must be obtained?
- What hemorrhage, edema, seizure, or thermal-injury sign must be watched for tonight?
- What postop scan timing and steroid/antiepileptic plan is appropriate?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Frame versus frameless/robot platform and planning software: [attending-specific]
- Trajectory constraints, number of cores/targets, and frozen/permanent pathology plan: [attending-specific]
- Steroid/antiepileptic prophylaxis and postop scan timing: [attending-specific]
- Admit versus discharge threshold and neuro-check frequency: [attending-specific]