
Case Prep: Open Brain Biopsy (Craniotomy/Burr-Hole Open Biopsy)
Case / Approach Snapshot
- Anatomy at risk: target margins, vascular/necrotic zones, entry cortex, sulci/vessels, ventricles, deep nuclei, and eloquent tracts along the trajectory.
- Operative steps: choose the safest diagnostic target, plan trajectory, verify registration or frame coordinates, obtain staged samples, confirm hemostasis/trajectory imaging, and coordinate pathology/molecular testing; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: nondiagnostic tissue, hemorrhage, seizure, edema, neurologic change, target shift, infection, and open biopsy or repeat sampling plan.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [superficial/accessible / large] [location] brain lesion of uncertain diagnosis planned for open biopsy via [mini-craniotomy / burr hole] [± limited resection/decompression].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Open brain biopsy for nonneoplastic undiagnosed neurological conditions: diagnostic yield, clinical impact, and contemporary role — Greeneway GP. Irish journal of medical science 2026. PubMed
- Diagnostic open brain biopsy following initial negative results of cerebrospinal fluid assessment for Toxoplasma — Senoo Y. Transplant infectious disease : an official journal of the Transplantation Society 2017. PubMed
- Angiography-negative childhood primary angiitis of the central nervous system diagnosed by open brain biopsy: a case report — Kang D. Encephalitis (Seoul, Korea) 2022. PubMed
- Open biopsy in patients with acute progressive neurologic decline and absence of mass lesion — Schuette AJ. Neurology 2010. PubMed
- Intravascular Large B-Cell Lymphoma Diagnosed by Open Brain Biopsy and Achievement of Remission After Early Initiation of Chemotherapy: Case Report — Tsukamoto E. Cureus 2022. PubMed
- Primary diffuse large B-cell lymphoma of the central nervous system identified with CSF biomarkers — Loser V. BMC neurology 2024. PubMed
- Impact of brain biopsy on the management of patients with nonneoplastic undiagnosed neurological disorders — Pulhorn H. Neurosurgery 2008. PubMed
- Incidentalomas to glioblastoma multiforme — Sachdev B. Oxford medical case reports 2014. PubMed
- Long-term utility and complication profile of open craniotomy for biopsy in patients with idiopathic encephalitis — Abdullah KG. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia 2017. PubMed
- [A case of intracranial tuberculoma early diagnosed by open brain biopsy] — Nakamura H. No to shinkei = Brain and nerve 2001. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
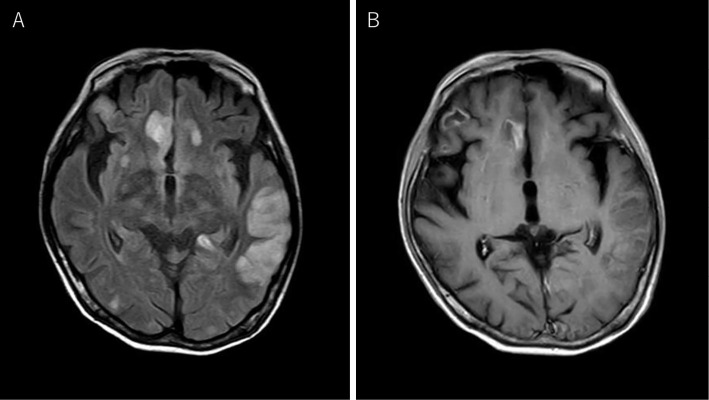 Figure 1.. Brain MRI images on admission. Multiple high-intensity lesions on FLAIR images were observed above the tent (A). Gadolinium-enhanced T1-weighted imaging showed a contrast effect in part… Source: Varicella Zoster Virus Encephalitis with Advanced Human Immunodeficiency Virus Disease Diagnosed by Brain Biopsy — Internal Medicine 2024; CC BY-NC-ND.
Figure 1.. Brain MRI images on admission. Multiple high-intensity lesions on FLAIR images were observed above the tent (A). Gadolinium-enhanced T1-weighted imaging showed a contrast effect in part… Source: Varicella Zoster Virus Encephalitis with Advanced Human Immunodeficiency Virus Disease Diagnosed by Brain Biopsy — Internal Medicine 2024; CC BY-NC-ND.
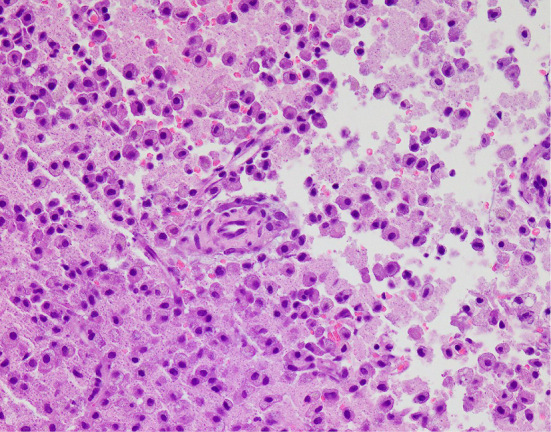 Figure 2.. Pathological findings of a brain biopsy specimen (Hematoxylin and Eosin staining). Necrotic tissue with abundant foam cells is surrounded by degenerative tissue and proliferating blood… Source: Varicella Zoster Virus Encephalitis with Advanced Human Immunodeficiency Virus Disease Diagnosed by Brain Biopsy — Internal Medicine 2024; CC BY-NC-ND.
Figure 2.. Pathological findings of a brain biopsy specimen (Hematoxylin and Eosin staining). Necrotic tissue with abundant foam cells is surrounded by degenerative tissue and proliferating blood… Source: Varicella Zoster Virus Encephalitis with Advanced Human Immunodeficiency Virus Disease Diagnosed by Brain Biopsy — Internal Medicine 2024; CC BY-NC-ND.
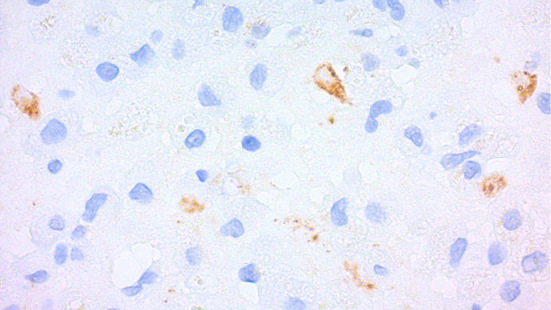 Figure 3.. Immunohistochemistry findings for VZV of a brain biopsy specimen. Immunohistochemistry with a monoclonal antibody for the VZV glycoprotein showed positive signals (brown area) in the… Source: Varicella Zoster Virus Encephalitis with Advanced Human Immunodeficiency Virus Disease Diagnosed by Brain Biopsy — Internal Medicine 2024; CC BY-NC-ND.
Figure 3.. Immunohistochemistry findings for VZV of a brain biopsy specimen. Immunohistochemistry with a monoclonal antibody for the VZV glycoprotein showed positive signals (brown area) in the… Source: Varicella Zoster Virus Encephalitis with Advanced Human Immunodeficiency Virus Disease Diagnosed by Brain Biopsy — Internal Medicine 2024; CC BY-NC-ND.
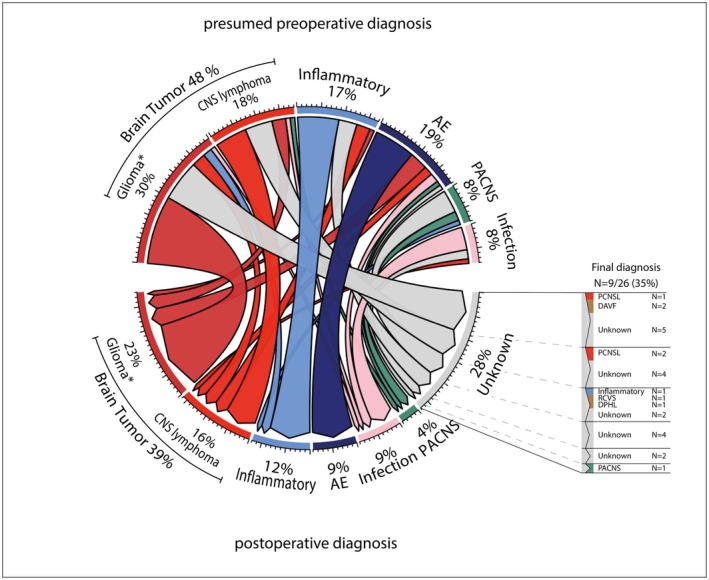 Figure 2. Chord diagram demonstrating change of diagnosis before and after brain biopsy. AE, autoimmune encephalitis; CNS, central nervous system; DAVF, dural arteriovenous fistulas; DPHL, delayed… Source: Clinical impact and safety of brain biopsy in unexplained central nervous system disorders: a real‐world cohort study — Annals of Clinical and Translational Neurology 2025; CC BY.
Figure 2. Chord diagram demonstrating change of diagnosis before and after brain biopsy. AE, autoimmune encephalitis; CNS, central nervous system; DAVF, dural arteriovenous fistulas; DPHL, delayed… Source: Clinical impact and safety of brain biopsy in unexplained central nervous system disorders: a real‐world cohort study — Annals of Clinical and Translational Neurology 2025; CC BY.
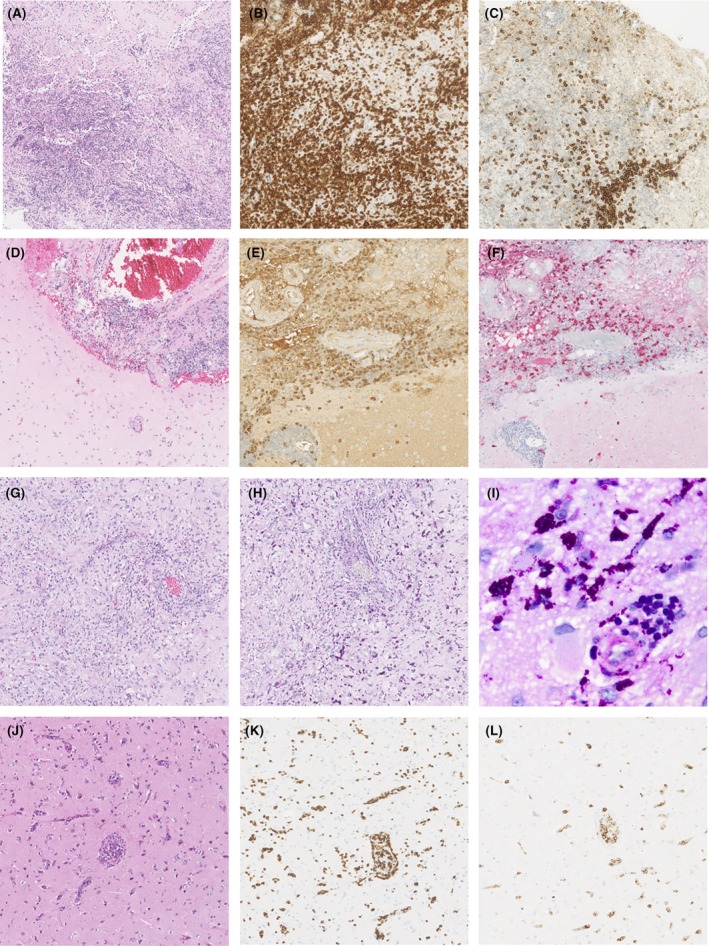 Figure 3. Neuropathological findings of brain biopsy in unexplained CNS disorders. (A–C) Chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroids (CLIPPERS);… Source: Clinical impact and safety of brain biopsy in unexplained central nervous system disorders: a real‐world cohort study — Annals of Clinical and Translational Neurology 2025; CC BY.
Figure 3. Neuropathological findings of brain biopsy in unexplained CNS disorders. (A–C) Chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroids (CLIPPERS);… Source: Clinical impact and safety of brain biopsy in unexplained central nervous system disorders: a real‐world cohort study — Annals of Clinical and Translational Neurology 2025; CC BY.
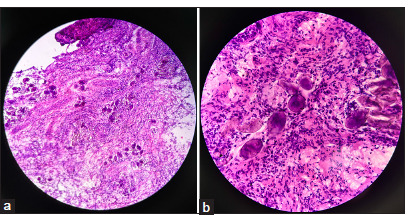 Figure 2:. Biopsy demonstrating scattered perivascular aggregates of schistosoma eggs with surrounding gliosis. (a) Low-power field. (b) High-power field. Stain used: Hematoxylin and eosin. Source: Neuroschistosomiasis presenting as recurrent seizures: A case report — Surgical Neurology International 2025; CC BY-NC-SA.
Figure 2:. Biopsy demonstrating scattered perivascular aggregates of schistosoma eggs with surrounding gliosis. (a) Low-power field. (b) High-power field. Stain used: Hematoxylin and eosin. Source: Neuroschistosomiasis presenting as recurrent seizures: A case report — Surgical Neurology International 2025; CC BY-NC-SA.
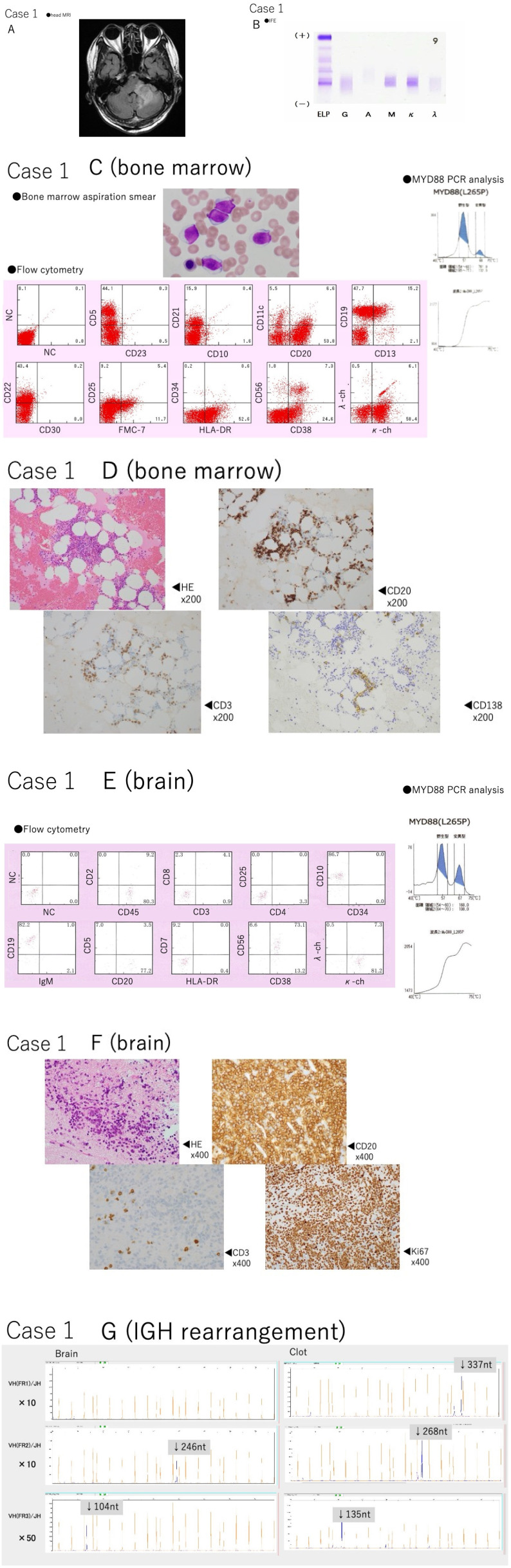 Fig. 1. Case details of Case 1.(A) Magnetic resonance imaging was performed, revealing a single mass in the left cerebellar peduncle. It was hypointense on T1- and T2-weighted imaging. The mass… Source: MYD88 mutation-positive indolent B-cell lymphoma with CNS involvement: Bing–Neel syndrome mimickers — Journal of Clinical and Experimental Hematopathology : JCEH 2024; CC BY-NC-SA.
Fig. 1. Case details of Case 1.(A) Magnetic resonance imaging was performed, revealing a single mass in the left cerebellar peduncle. It was hypointense on T1- and T2-weighted imaging. The mass… Source: MYD88 mutation-positive indolent B-cell lymphoma with CNS involvement: Bing–Neel syndrome mimickers — Journal of Clinical and Experimental Hematopathology : JCEH 2024; CC BY-NC-SA.
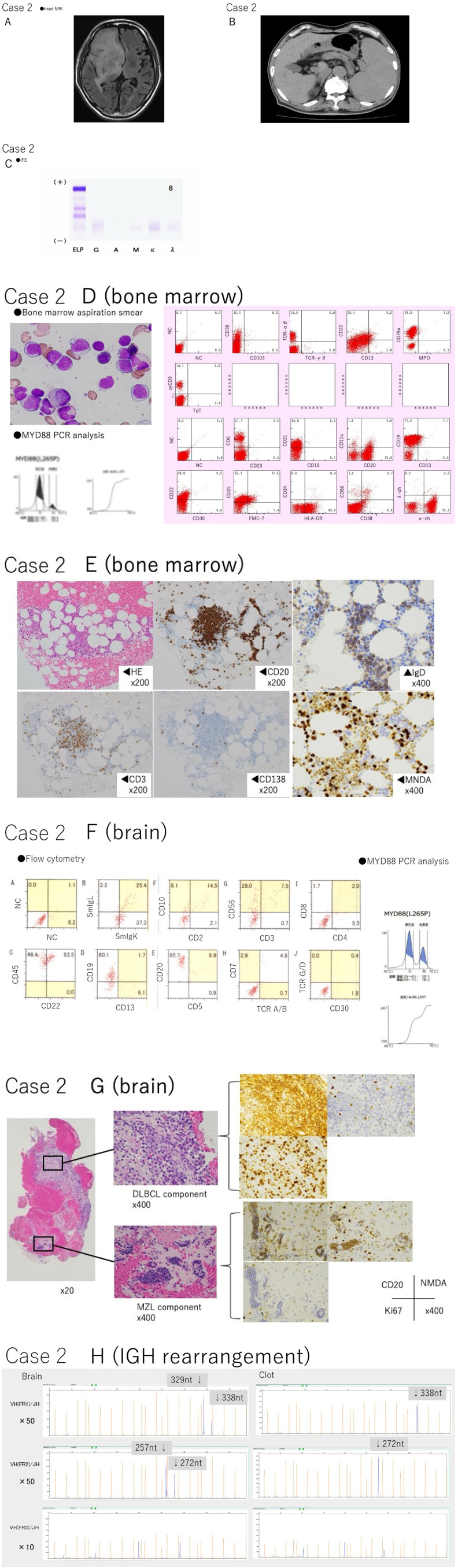 Fig. 2. Case details of Case 2.(A) Magnetic resonance imaging (MRI) showed a single mass in the right basal ganglia, which was hypointense on T1- and T2-weighted imaging. The mass was… Source: MYD88 mutation-positive indolent B-cell lymphoma with CNS involvement: Bing–Neel syndrome mimickers — Journal of Clinical and Experimental Hematopathology : JCEH 2024; CC BY-NC-SA.
Fig. 2. Case details of Case 2.(A) Magnetic resonance imaging (MRI) showed a single mass in the right basal ganglia, which was hypointense on T1- and T2-weighted imaging. The mass was… Source: MYD88 mutation-positive indolent B-cell lymphoma with CNS involvement: Bing–Neel syndrome mimickers — Journal of Clinical and Experimental Hematopathology : JCEH 2024; CC BY-NC-SA.
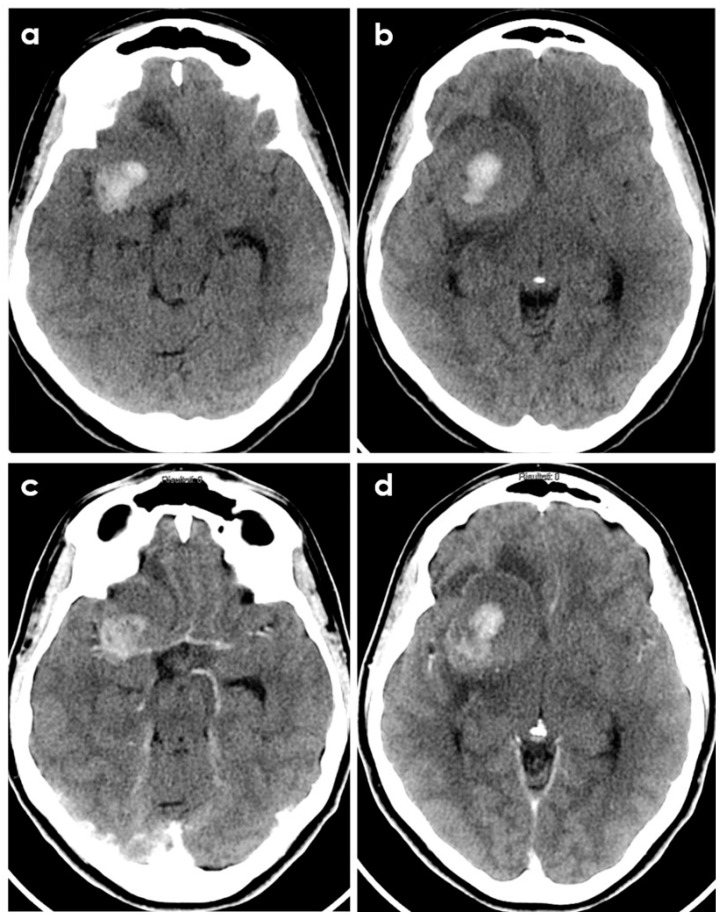 Figure 2. Brain CT of a young patient with biopsy-proven PACNS and ICH at presentation. The patient had a history of headache lasting 6 months before imaging. Panels (a,b) show the non-contrast CT… Source: The Hemorrhagic Side of Primary Angiitis of the Central Nervous System (PACNS) — Biomedicines 2024; CC BY.
Figure 2. Brain CT of a young patient with biopsy-proven PACNS and ICH at presentation. The patient had a history of headache lasting 6 months before imaging. Panels (a,b) show the non-contrast CT… Source: The Hemorrhagic Side of Primary Angiitis of the Central Nervous System (PACNS) — Biomedicines 2024; CC BY.
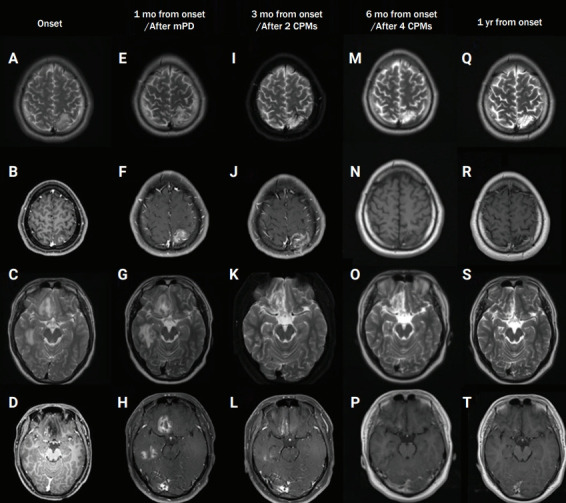 Figure 1.. Serial brain MRI findings at onset (A–D), 1 month after onset, after steroid treatment (E–H), 3 months after onset, after two cycles of intravenous cyclophosphamide (I–L), after… Source: Angiography-negative childhood primary angiitis of the central nervous system diagnosed by open brain biopsy: a case report — Encephalitis 2022; CC BY-NC.
Figure 1.. Serial brain MRI findings at onset (A–D), 1 month after onset, after steroid treatment (E–H), 3 months after onset, after two cycles of intravenous cyclophosphamide (I–L), after… Source: Angiography-negative childhood primary angiitis of the central nervous system diagnosed by open brain biopsy: a case report — Encephalitis 2022; CC BY-NC.
History of Present Illness
- Chief complaint: Lesion requiring tissue diagnosis where an open approach is preferable to needle biopsy
- Open biopsy indications:
- Superficial/accessible lesion
- Need for a larger tissue sample (e.g., diagnostic uncertainty, suspected lymphoma after non-diagnostic needle, inflammatory/demyelinating, specialized studies)
- Vascular lesion where needle biopsy is hazardous (visualize and control bleeding)
- Concurrent need for decompression / partial resection (mass effect)
- Failed stereotactic biopsy
- Same diagnostic considerations (lymphoma — avoid pre-biopsy steroids if feasible; infection)
Past Medical History
- Anticoagulant/antiplatelet (stop/correct), immunocompromise, prior malignancy
- Standard PMH
Imaging Review
MRI (T1±Gad, T2, FLAIR, DWI, SWI) ± CTA
- Lesion location/depth, enhancing/representative target, vascularity, eloquence
- Navigation planning (localize lesion for a small targeted craniotomy)
Labs
- CBC, BMP, Coags, type and screen
Neurological Examination
- Baseline focal exam
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: frame/robot/navigation system registered and independently checked, biopsy needle and specimen cups/media ready, frozen/smear pathology available, trajectory images displayed, and immediate CT access planned.
- Special needs: coagulopathy/antiplatelet correction, steroids held when lymphoma is suspected and clinically safe, seizure prophylaxis by lesion/location, BP control, and specimen handling for flow cytometry, cultures, and molecular testing.
- Immediate postop orders: neuro checks, CT head to exclude hemorrhage, BP parameters, dexamethasone only if clinically indicated, antiepileptic plan, pathology follow-up, and escalation plan for tract hemorrhage or nondiagnostic result.
Open Versus Needle Biopsy Decision
- Favor open biopsy when the lesion is superficial/cortical, vascular/hemorrhagic, requires larger architecture for diagnosis, has failed stereotactic biopsy, or needs limited decompression at the same sitting.
- Favor stereotactic needle biopsy for deep, small, multifocal, medically fragile, or eloquent lesions where a craniotomy/corticotomy adds avoidable morbidity.
- If lymphoma is high on the differential, avoid pre-biopsy steroids when clinically feasible and send fresh tissue for flow cytometry in addition to permanent pathology.
- If infection/inflammation is plausible, coordinate specimen handling before incision: aerobic/anaerobic, fungal, AFB, viral/PCR, pathology, and tissue saved for molecular testing when appropriate.
Position & Approach
- Per lesion location; navigation-guided small craniotomy or burr hole over the lesion; Mayfield; lesion at accessible/highest point
Key Surgical Steps
- Navigation-planned incision and small (mini) craniotomy or burr hole over the lesion
- Open dura
- Localize the lesion (navigation, ultrasound, surface appearance — discoloration, abnormal cortex)
- If subcortical: small corticotomy (through a sulcus/non-eloquent cortex) to reach the lesion
- Obtain generous tissue samples under direct vision — including the enhancing/representative portion (avoid necrotic core); take multiple samples
- Frozen section/smear confirmation of diagnostic tissue (re-sample if non-diagnostic)
- Direct hemostasis under vision (bipolar) — advantage of open biopsy for vascular lesions
- ± Limited debulking/decompression if mass effect and tissue confirms a process where decompression helps (judgment)
- Watertight dural closure, bone flap replacement (craniotomy) or closure (burr hole), standard closure
Critical Anatomy & Structures at Risk
- Eloquent cortex / tracts (corticotomy site — use navigation, sulcal entry)
- Vessels — direct visualization aids control (advantage over needle)
- Draining veins, dura/sinuses depending on location
Equipment
- Microscope, navigation, ultrasound, bipolar
- Standard craniotomy/burr-hole set, biopsy/resection instruments (cup forceps, CUSA if debulking)
- Hemostatic agents, dural substitute, frozen-section pathology
Monitoring
- SSEP/MEP/mapping if near eloquent cortex
Anesthesia
- GA; cefazolin; mannitol/steroids per mass effect (hold steroids if lymphoma pending and feasible)
Potential Complications
- Hemorrhage (directly controllable — advantage), edema/mass effect
- Neurological deficit (corticotomy/eloquent), seizure, infection, CSF leak
- Non-diagnostic (less likely than needle given larger sample + frozen confirmation)
Tissue and Rescue Strategy
- Frozen section nondiagnostic: resample the enhancing/rim/solid component, avoid necrotic center, use ultrasound/navigation update for shift, and confirm pathology has enough tissue before closure.
- Unexpected high-grade tumor with mass effect: decide whether limited debulking is safe and aligned with consent; do not convert a diagnostic biopsy into a major resection without a clear preoperative contingency.
- Unexpected abscess/pus: obtain cultures before antibiotics if stable, irrigate/decompress as needed, and avoid spilling infected material through clean planes.
- Bleeding lesion: use the open exposure advantage: bipolar under direct vision, hemostatic agents, wider exposure only if needed, postop CT threshold low.
- Eloquent cortex concern: stop at diagnostic tissue if mapping/monitoring changes or the corridor becomes functionally unsafe.
Operative Note Template
Preoperative Diagnosis: [Superficial/accessible] [location] brain lesion of uncertain diagnosis [with mass effect]
Postoperative Diagnosis: Same (pending pathology)
Procedure: Open biopsy of [location] lesion via [mini-craniotomy / burr hole] [with limited decompression]
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Adjuncts: Microscope, navigation, ultrasound, bipolar; frozen section Specimens: Brain lesion (generous directed samples) Complications: None
Indications: [Age]yo [M/F] with a [superficial/vascular/large] [location] lesion where an open approach is preferable (larger sample / direct hemostasis / decompression / failed needle biopsy). [Steroids withheld if lymphoma suspected.] Risks (hemorrhage, deficit, edema) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced and the head fixed. A navigation-planned small craniotomy/burr hole was made over the lesion and the dura opened. The lesion was localized (navigation/ultrasound/surface appearance) [via a small corticotomy through a sulcus for the subcortical lesion]. Generous, directed samples of representative (enhancing, non-necrotic) tissue were obtained under direct vision and frozen section confirmed diagnostic tissue. Direct hemostasis was achieved (advantageous for the vascular lesion). [A limited decompression/debulking was performed for mass effect.]
A watertight dural closure was performed, the bone replaced [for craniotomy], and the wound closed in layers. The patient was transferred to the [floor/ICU]; a postoperative CT/MRI was obtained.
Postoperative Plan
- Floor/ICU per extent, neuro checks
- Postop CT/MRI (hemorrhage, extent)
- Pathology (permanent/molecular; flow cytometry if lymphoma; cultures/microbiology if infection)
- Hold steroids if lymphoma pending (per team), seizure prophylaxis per practice, DVT prophylaxis
- Tumor board / management per diagnosis; follow-up
Chief-Level Case Review
Use these as the senior-level mental model for Open Brain Biopsy (Craniotomy/Burr-Hole Open Biopsy):
- Decision point: The target must answer the question: choose tissue/trajectory/dose based on diagnostic yield, molecular testing, treatment impact, and safest corridor.
- Technical lever: Risk lives along the path: vessels, sulci, ventricles, necrotic center, eloquent tracts, prior radiation, and anticoagulation decide whether the plan is acceptable.
- Bailout: Confirm before committing: frame/robot registration, coordinates, fiducials, trajectory collision, specimen adequacy, and postop scan threshold should be explicit.
- Postop watch: Postop plan should anticipate the rare catastrophe: hemorrhage, edema, seizure, steroid need, neurologic checks, pathology handoff, and treatment-board timing.
Common Pimp Questions
Use these to pressure-test preparation for Open Brain Biopsy (Craniotomy/Burr-Hole Open Biopsy):
- What target coordinate, trajectory, and no-fly-zone were chosen?
- What imaging confirms target accuracy and avoids vessel/ventricle/sulcus violation?
- What specimen, pathology, culture, or molecular study must be obtained?
- What hemorrhage, edema, seizure, or thermal-injury sign must be watched for tonight?
- What postop scan timing and steroid/antiepileptic plan is appropriate?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Frame versus frameless/robot platform and planning software: [attending-specific]
- Trajectory constraints, number of cores/targets, and frozen/permanent pathology plan: [attending-specific]
- Steroid/antiepileptic prophylaxis and postop scan timing: [attending-specific]
- Admit versus discharge threshold and neuro-check frequency: [attending-specific]