
Case Prep: Ventriculoperitoneal (VP) Shunt Placement
Case / Approach Snapshot
- Anatomy at risk: entry point, ventricular target, choroid plexus and deep veins, cortical vessels, eloquent cortex/tracts, catheter path, and distal hardware route.
- Operative steps: confirm indication and side, plan trajectory, prepare hardware, access ventricle or cistern safely, confirm flow/position, tunnel/connect devices when needed, and define infection/obstruction surveillance; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: malposition, hemorrhage, poor CSF return, overdrainage/underdrainage, obstruction, infection, abdominal/pleural complication, slit ventricles, and revision algorithm.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [communicating/obstructive] hydrocephalus due to [etiology] presenting with [headaches/gait instability/cognitive decline/enlarged head circumference] planned for right frontal VP shunt placement with [fixed/programmable] valve.
Figures, Imaging & Video
🎥 Operative videos & resources
- Technique searches: VP shunt placement on YouTube · laparoscopic VP shunt distal catheter placement
- Imaging review: Radiopaedia — VP shunt · Radiopaedia — hydrocephalus
- Open-access anatomy/technique: PubMed Central — ventriculoperitoneal shunt
High-Yield Literature
- Shunt migration in ventriculoperitoneal shunting: A comprehensive review of literature — Harischandra LS. Neurology India 2019. PubMed
- Ventriculoperitoneal Shunt Infection — López-Sánchez C. JAMA dermatology 2020. PubMed
- Techniques and Nuances in Ventriculoperitoneal Shunt Surgery — Pillai SV. Neurology India 2021. PubMed
- The Evolution of Ventriculoperitoneal Shunt Valves and Why They Fail — Stehlik BN. World neurosurgery 2025. PubMed
- Ventriculoperitoneal Shunt-related Intrapelvic Abscess — Zenda T. Internal medicine (Tokyo, Japan) 2020. PubMed
- Ventriculoperitoneal Shunt Complications In Children: An Evidence-Based Approach To Emergency Department Management — Bober J. Pediatric emergency medicine practice 2016. PubMed
- Ventriculoperitoneal shunt — Hauk L. AORN journal 2018. PubMed
- Ventriculoperitoneal Shunt Tap Task Trainer: A Technical Report — Connors J. Cureus 2023. PubMed
- Ventriculoperitoneal shunt tap — Oakes WJ. Journal of neurosurgery. Pediatrics 2008. PubMed
- Ventriculoperitoneal shunt migration into the pulmonary artery: Case report and literature review — González-Pombo M. Neurocirugia 2023. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
 Figure 1.. The ventriculoperitoneal shunt catheter is protruding through the patient’s normal-appearing anus. Source: Spontaneous bowel perforation complicating ventriculoperitoneal shunt: a case report — Cases Journal 2009; CC BY.
Figure 1.. The ventriculoperitoneal shunt catheter is protruding through the patient’s normal-appearing anus. Source: Spontaneous bowel perforation complicating ventriculoperitoneal shunt: a case report — Cases Journal 2009; CC BY.
 Figure 2.. Plain abdominal radiography showing the ventriculoperitoneal shunt catheter within the colonic lumen. Source: Spontaneous bowel perforation complicating ventriculoperitoneal shunt: a case report — Cases Journal 2009; CC BY.
Figure 2.. Plain abdominal radiography showing the ventriculoperitoneal shunt catheter within the colonic lumen. Source: Spontaneous bowel perforation complicating ventriculoperitoneal shunt: a case report — Cases Journal 2009; CC BY.
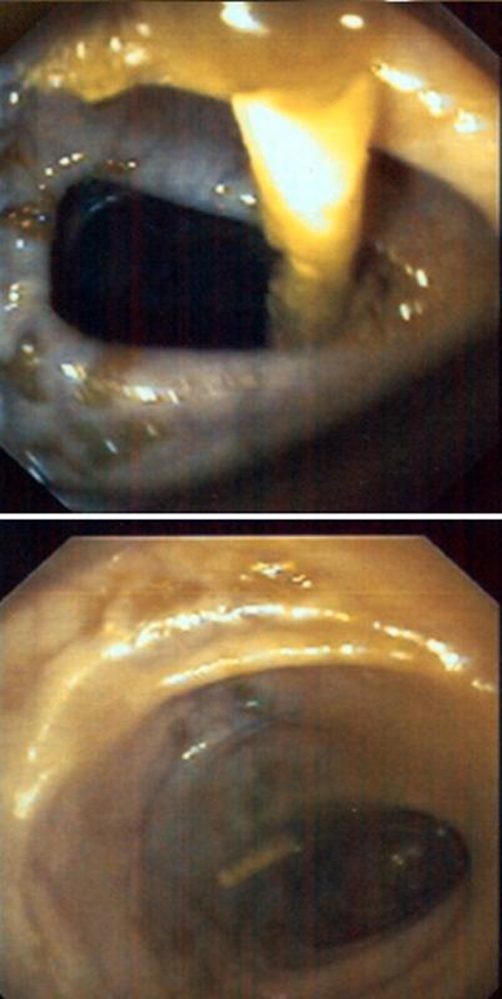 Figure 3.. Sigmoidoscopy showed the distal part of the ventriculoperitoneal shunt catheter within the sigmoid colon and the penetration site at the distal descending colon. Source: Spontaneous bowel perforation complicating ventriculoperitoneal shunt: a case report — Cases Journal 2009; CC BY.
Figure 3.. Sigmoidoscopy showed the distal part of the ventriculoperitoneal shunt catheter within the sigmoid colon and the penetration site at the distal descending colon. Source: Spontaneous bowel perforation complicating ventriculoperitoneal shunt: a case report — Cases Journal 2009; CC BY.
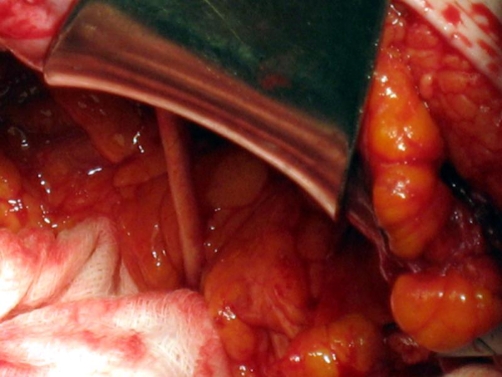 Figure 4.. Laparotomy view: the distal part of the ventriculoperitoneal shunt catheter penetrating the sigmoid colon. Source: Spontaneous bowel perforation complicating ventriculoperitoneal shunt: a case report — Cases Journal 2009; CC BY.
Figure 4.. Laparotomy view: the distal part of the ventriculoperitoneal shunt catheter penetrating the sigmoid colon. Source: Spontaneous bowel perforation complicating ventriculoperitoneal shunt: a case report — Cases Journal 2009; CC BY.
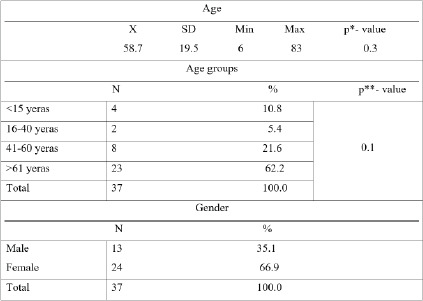 Table 1.. Distribution of patients with implanted ventriculoperitoneal shunts by age and gender *-T test; X- Mean value; SD- Standard deviation; **-Chi-square test of independence Source: Complications and Outcome in Patients With Hydrocephalus Who Have Had a Ventriculoperitoneal Shunt Implanted — Medical Archives 2025; CC BY-NC.
Table 1.. Distribution of patients with implanted ventriculoperitoneal shunts by age and gender *-T test; X- Mean value; SD- Standard deviation; **-Chi-square test of independence Source: Complications and Outcome in Patients With Hydrocephalus Who Have Had a Ventriculoperitoneal Shunt Implanted — Medical Archives 2025; CC BY-NC.
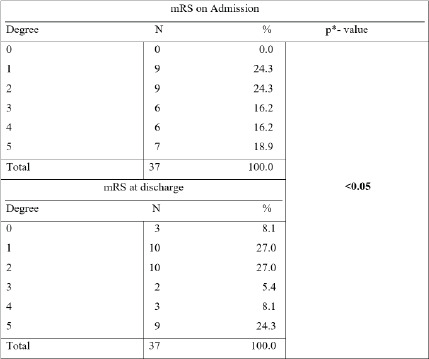 Table 2.. Degree of disability of patients with implanted ventriculoperitoneal shunt mRS on Admission, mRS-Modified Rankin Scale; * - Chi-square test; Source: Complications and Outcome in Patients With Hydrocephalus Who Have Had a Ventriculoperitoneal Shunt Implanted — Medical Archives 2025; CC BY-NC.
Table 2.. Degree of disability of patients with implanted ventriculoperitoneal shunt mRS on Admission, mRS-Modified Rankin Scale; * - Chi-square test; Source: Complications and Outcome in Patients With Hydrocephalus Who Have Had a Ventriculoperitoneal Shunt Implanted — Medical Archives 2025; CC BY-NC.
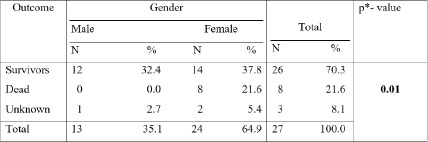 Table 3.. Outcome of patients with idiopathic hydrocephalus who underwent ventriculoperitoneal shunt implantation in relation to gender * - Chi-square test; Source: Complications and Outcome in Patients With Hydrocephalus Who Have Had a Ventriculoperitoneal Shunt Implanted — Medical Archives 2025; CC BY-NC.
Table 3.. Outcome of patients with idiopathic hydrocephalus who underwent ventriculoperitoneal shunt implantation in relation to gender * - Chi-square test; Source: Complications and Outcome in Patients With Hydrocephalus Who Have Had a Ventriculoperitoneal Shunt Implanted — Medical Archives 2025; CC BY-NC.
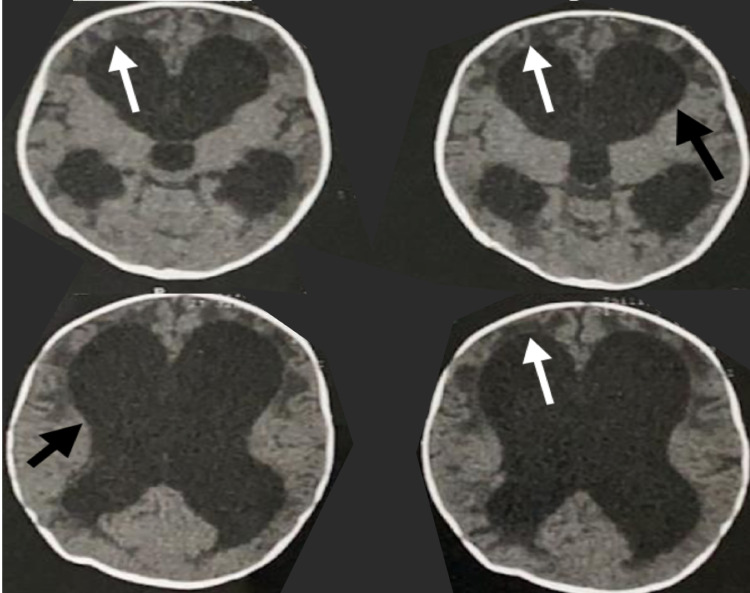 Figure 1. Axial computed tomography (CT) scan Shows enlargement of the ventricles (black arrows) with transependymal edema (white arrows). Source: The Intraventricular Pseudocyst as a Complication of Ventriculoperitoneal Shunt: A Rare Case Report and Review of Literature — Cureus 2021; CC BY.
Figure 1. Axial computed tomography (CT) scan Shows enlargement of the ventricles (black arrows) with transependymal edema (white arrows). Source: The Intraventricular Pseudocyst as a Complication of Ventriculoperitoneal Shunt: A Rare Case Report and Review of Literature — Cureus 2021; CC BY.
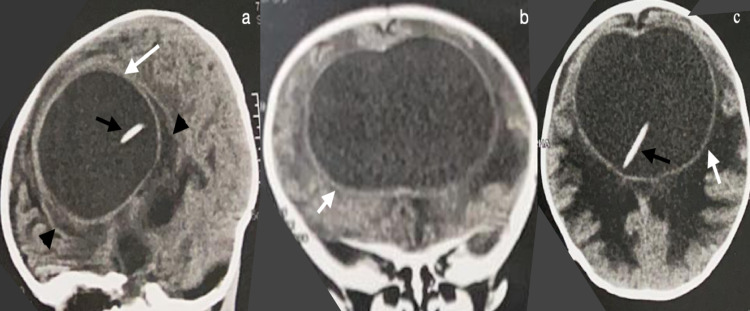 Figure 2. Computed tomography (CT) scan without contrast enhancementCT scan without contrast enhancement in the sagittal (a), coronal (b), and axial (c) planes. Shows pseudocyst (white arrows)… Source: The Intraventricular Pseudocyst as a Complication of Ventriculoperitoneal Shunt: A Rare Case Report and Review of Literature — Cureus 2021; CC BY.
Figure 2. Computed tomography (CT) scan without contrast enhancementCT scan without contrast enhancement in the sagittal (a), coronal (b), and axial (c) planes. Shows pseudocyst (white arrows)… Source: The Intraventricular Pseudocyst as a Complication of Ventriculoperitoneal Shunt: A Rare Case Report and Review of Literature — Cureus 2021; CC BY.
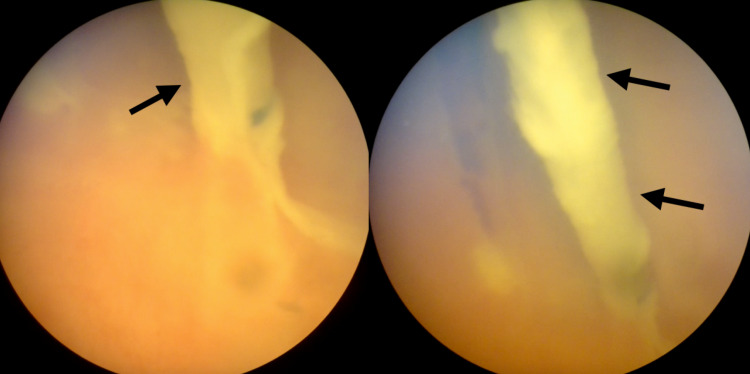 Figure 3. Endoscopic image Showing ventricular catheter inside the cystic cavity (black arrows). Source: The Intraventricular Pseudocyst as a Complication of Ventriculoperitoneal Shunt: A Rare Case Report and Review of Literature — Cureus 2021; CC BY.
Figure 3. Endoscopic image Showing ventricular catheter inside the cystic cavity (black arrows). Source: The Intraventricular Pseudocyst as a Complication of Ventriculoperitoneal Shunt: A Rare Case Report and Review of Literature — Cureus 2021; CC BY.
History of Present Illness
- Chief complaint: Headaches / gait instability / urinary incontinence / cognitive decline / increasing head circumference (pediatric)
- Duration and progression:
- Hydrocephalus type:
- Communicating: Post-SAH, post-meningitis, post-hemorrhagic (neonatal), idiopathic
- Obstructive: Aqueductal stenosis, tumor, Chiari, Dandy-Walker
- Normal pressure hydrocephalus (NPH): Classic triad — gait apraxia, urinary incontinence, dementia (“wet, wobbly, wacky”)
- Prior shunt history: Previous VP shunts, revisions, infections
- Prior EVD/ETV:
- NPH workup: Large-volume LP (improvement after 30-50 mL drainage supports diagnosis)
Past Medical History
- Prior shunt/revisions (dates, sides, types)
- Prior CNS infection (ventriculitis, meningitis)
- Prior abdominal surgery (adhesions affect peritoneal catheter)
- Peritoneal pathology (ascites, peritonitis, prior peritoneal catheter complications)
- Latex allergy (spina bifida patients — high rate)
- Allergies:
- Medications:
Imaging Review
CT Head
- Ventriculomegaly: Frontal horn index, temporal horn size
- Evans index: Frontal horn width / max biparietal diameter (> 0.3 = hydrocephalus)
- Periventricular lucency (acute hydrocephalus)
- Cortical mantle thickness at planned entry site
- Prior shunt hardware
MRI Brain
- Aqueductal flow void (present = patent; absent = stenosis)
- CSF flow study (cine MRI) if obstructive hydrocephalus suspected
- Underlying pathology
- For NPH: DESH (disproportionately enlarged subarachnoid space hydrocephalus) pattern
Labs
- CBC, BMP, Coags
- Type and screen
- CSF studies from LP (if recent LP done — cell count, protein, glucose, culture)
Neurological Examination
NPH Assessment
- Gait: Wide-based, magnetic, shuffling, turns en bloc
- Timed Up and Go (TUG) test: Baseline ___
- Cognition: MMSE/MoCA: ___
- Urinary: Frequency, urgency, incontinence
- Post-LP improvement (if large-volume LP performed): Gait improvement suggests shunt-responsive NPH
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: navigation or endoscope as indicated, shunt hardware/valve setting verified, distal-access tools or general surgery help when needed, antibiotic-impregnated catheter availability, and postop imaging plan.
- Special needs: antibiotic timing, programmable valve documentation, abdominal/chest/vascular distal-site plan, CSF culture plan for revision/infection, anticoagulation plan, and EVD backup if access fails.
- Immediate postop orders: neuro checks, CT or shunt-series timing, valve setting documentation and MRI precautions, wound/abdominal/distal-site checks, infection watch, DVT timing, and follow-up for setting adjustment.
Valve Selection
- Fixed-pressure valve: Low, medium, or high pressure (set at manufacture)
- Programmable valve (preferred): Adjustable pressure setting post-op (e.g., Strata, Certas, proGAV, Codman Hakim)
- Can adjust non-invasively if over/under-drainage occurs
- Initial setting typically medium (e.g., 1.5 or performance level 1.5)
- Anti-siphon device / gravitational valve: Reduces overdrainage in upright position
- On/off valve: Rarely used
Position
- Patient position: Supine, head turned to the LEFT (right side up for right-sided shunt)
- Head: On horseshoe headrest or Mayfield (for navigation-guided proximal catheter)
- Right side exposed: Head, neck, chest, abdomen — all prepped in one field
- Arms: Left arm tucked, right arm on armboard or tucked
Incision Sites
- Cranial: Right frontal (Kocher’s point) or right parieto-occipital (Keen’s point or Frazier’s point)
- Abdominal: Small periumbilical or subcostal incision (for peritoneal catheter insertion)
Key Surgical Steps
Proximal catheter (ventricular):
- Mark entry point (Kocher’s point: 11 cm from nasion, 3 cm from midline; OR occipital)
- Incision (~3 cm), expose skull
- Burr hole
- Open dura
- Pass ventricular catheter to 5-5.5 cm depth (target: frontal horn)
- Aim: ipsilateral medial canthus (coronal), ipsilateral tragus (sagittal)
- OR use navigation for guided placement
- Confirm CSF flow
- Connect to valve
Tunneling:
- Subcutaneous tunnel from cranial incision to abdominal incision
- Use shunt passer (long tunneling rod)
- Pass behind the ear, down the neck (anterior to SCM), across the chest, to the abdomen
- Avoid crossing midline
- Ensure valve sits behind the ear (accessible for programming/palpation)
Distal catheter (peritoneal):
- Abdominal incision — small (2-3 cm) periumbilical or subcostal
- Dissect through subcutaneous tissue, fascia, muscle
- Identify peritoneum, open carefully (avoid bowel injury)
- Insert peritoneal catheter (~20-25 cm of tubing into peritoneal cavity)
- Confirm distal flow of CSF through the system
- Close peritoneal entry tightly around catheter to prevent CSF leak/hernia
- Close all incisions
Alternative distal sites:
- Atrium (VA shunt) — for patients with abdominal pathology
- Pleural space (ventriculopleural) — less common
Critical Anatomy
- Ventricular catheter: Same risks as EVD (cortical vessels, caudate, thalamus)
- Great vessels in neck: Carotid, IJV — tunneling should be superficial to SCM fascia
- Peritoneum: Bowel injury during peritoneal entry
- Subcutaneous tunnel: Avoid skin erosion over hardware (adequate tissue coverage)
Equipment
- Shunt system (valve, ventricular catheter, peritoneal catheter, connectors)
- Valve type: [Programmable — brand and initial setting]
- Tunneling rod (shunt passer)
- Drill (twist drill or perforator)
- Navigation (optional but recommended for proximal catheter)
- Antibiotics: Vancomycin irrigation per protocol
- Antibiotic-impregnated catheter (Bactiseal or Ares — reduces infection rate)
Monitoring
- Standard ASA monitors
Anesthesia
- General endotracheal anesthesia
- Cefazolin 2g IV (some add vancomycin IV per protocol)
- Single-dose abdominal/chest prep
Potential Complications
- Shunt infection (5-10%) — presents days to weeks post-op; treated with shunt removal, EVD, IV antibiotics, then reshunt
- Shunt malfunction — proximal obstruction (most common), distal obstruction, valve failure
- Over-drainage — subdural hematomas/hygromas, slit ventricle syndrome; adjust programmable valve
- Under-drainage — persistent hydrocephalus; lower valve setting or check for obstruction
- Peritoneal complications — pseudocyst, infection, bowel perforation (rare)
- Hardware erosion — especially in pediatric patients with thin skin
- Wound infection — superficial; may be managed with antibiotics vs hardware removal
Operative Note Template
Preoperative Diagnosis: [Communicating/Obstructive] hydrocephalus due to [etiology]
Postoperative Diagnosis: Same
Procedure: Right frontal ventriculoperitoneal shunt placement with [programmable valve type] set at [initial pressure setting]
[Include: ventricular catheter depth, CSF flow confirmation, valve placement, tunneling path, peritoneal entry, peritoneal catheter length, system flow confirmation]
Postoperative Plan
- Floor admission or step-down x 24 hours
- Neuro checks q2h x 24h
- CT head within 24 hours (catheter position, ventricle size)
- Abdominal X-ray (confirm peritoneal catheter position and coiling)
- Shunt series X-rays (skull, chest, abdomen) — baseline for future comparison
- Monitor for signs of over-drainage: Positional headache, subdural collections
- Monitor for signs of under-drainage: Persistent symptoms, enlarging ventricles
- Programmable valve setting: Initial setting ___ ; document for patient records and card
- MRI safety: Document valve type and MRI compatibility; most modern programmable valves are MRI-conditional but may need resetting after MRI
- Wound care: Keep dry x 48h; inspect for CSF leak, redness
- Activity: No heavy lifting x 4-6 weeks
- Educate patient/family on shunt malfunction signs
- Follow-up: 2-4 weeks clinic; CT at 3 months (new baseline ventricle size)
- NPH patients: Repeat gait assessment at 1-3 months; adjust valve if needed
Chief-Level Case Review
Use these as the senior-level mental model for Ventriculoperitoneal (VP) Shunt Placement:
- Decision point: Trajectory and hardware choice should follow the failure mode: obstruction, infection, overdrainage, loculation, slit ventricle, distal failure, or wrong pressure setting.
- Technical lever: Document the system: entry point, catheter target/depth, valve type and setting, distal site, antibiotic-impregnated hardware, and what imaging confirms placement.
- Bailout: Rescue plan is practical: poor CSF return, bloody CSF, malposition, distal access failure, abdominal/pleural complication, or inability to safely pass the catheter.
- Postop watch: Postop orders must be unambiguous: drain height/rate/max output, valve setting, clamp parameters, imaging, antibiotics, ICP/neuro checks, and overdrainage precautions.
Common Pimp Questions
Use these to pressure-test preparation for Ventriculoperitoneal (VP) Shunt Placement:
- What is the working CSF physiology problem: obstruction, absorption failure, overdrainage, infection, or catheter failure?
- Where exactly is the entry point, target, and backup trajectory?
- What valve, catheter, endoscope, or navigation preference does the attending use?
- What is the infection-prevention plan and what cultures/CSF studies are needed?
- What postop imaging, valve setting, drainage level, and neuro-check plan should be written?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Valve brand/setting, antibiotic catheter use, and tunneling side: [attending-specific]
- Navigation/endoscope/stylet preference and ventricular target: [attending-specific]
- CSF culture/lab routine and perioperative antibiotic duration: [attending-specific]
- Postop scan timing, EVD height or valve verification, and activity restrictions: [attending-specific]